


Abstract
Objectives: To establish retrospectively the relation between the histopathologic grade of colorectal liver metastasis and apparent diffusion coefficient (ADC) values of hepatic metastases of colorectal adenocarcinomas.
Methods: The diagnoses of liver metastases were confirmed with biopsy, surgery, and follow-up imaging findings. Twenty-six patients with 94 liver metastasis were included in the study. Of 94 masses, 59 were poorly-differentiated adenocarcinoma, 18 were moderately-differentiated adenocarcinoma, and 17 were well-differentiated regarding the diameters, ADC values, and ratio index (RI) values. Kolmogorov-smirnov normality test, Kruskal-wallis analysis of variance, Mann-Whitney U test with Bonferroni correction, Spearman correlation analysis, and receiver operating characteristics curve methods were applied to evaluate the statistical relations.
Results: There was a statistically significant difference in terms of ADC values and RI between poorly-differentiated adenocarcinoma and moderately-differentiated adenocarcinoma plus well-differentiated adenocarcinomas. Poorly-differentiated adenocarcinomas have the lowest ADC values and highest RI values among other groups.
Conclusion: Use of ADC values alone can be executed for the diagnosis of focal hepatic masses and also can aid in the differentiation of benign and malignant hepatic lesions.
In the recent years, the importance of diffusion weighted imaging (DWI) has been increasing gradually in the diagnosis and characterization of liver masses.1-3 It is well known that apparent diffusion coefficient (ADC) values change depending on the mass cellularity of focal liver lesions. In this research, we aim to evaluate the association between the histopathologic grade of colorectal liver metastasis and ADC values in liver metastases of colorectal adenocarcinomas retrospectively.
Methods
In our study, we retrospectively reviewed the MRI results of patients with colorectal adenocarcinoma who were recorded in Ankara Ataturk research hospital’s picture archiving and communication system between January 2012 and November 2013. The total sampled size was 50 patients. The MRIs were handled by 1.5 T MR, 32 mT gradient strength unit (Achieva, Philips Healthcare, Best, The Netherlands) with phased-array torso XL coil and all images were evaluated by a radiologist with 12 years experience in handling MR. Diffusion weighted imaging was performed in the transverse plane by using a spin-echo, echo-planar imaging sequence with fat suppression and breath-hold acquisition. The parameters were repetition/echo inversion time of 12000/100/2200 msec., diffusion gradient encoding in 3 orthogonal directions; gradient amplitude (b-value): 0-800 s/mm2, field of view was 385 mm, matrix size was 160-110 pixels, section thickness was 6 mm, section gap was 1 mm, and the number of signals acquired was 1. Diffusion weighted imaging scans were acquired before contrast-enhanced T1-weighted imaging and the acquisition time was 2.23 min. The diagnoses of liver metastases were confirmed with biopsy, surgery, and follow-up images. Ten patients had a lung and mesenteric lymph node metastasis without any hepatic invasion, 10 patients had no DWI and ADC-mapping analysis in their routine abdominal MRI, and 4 patients had an abdominal MRI with poor image quality. Therefore, 24 patients were excluded from the study. Exclusion criteria were the presence of other metastasis without any liver metastasis, poor image quality of DWI, ADC mapping analysis, and abdominal MR exams without any ADC analysis.
Twenty-six patients with 94 liver metastasis were included in this study. Eleven patients were females (42.3%) and 15 were males (57,7%). The mean age was 62.76 ± 7.17. Metastases were re-evaluated in 26 patients, all hepatic masses were between 9-111 mm with a mean diameter of 27.04 ± 19.50 mm. Inclusion criteria was the presence of any proper hepatic masses of colonic adenocarcinomas with clear ADC values. In 6 patients, single hepatic masses were observed and these lesions were confirmed histopathologically via biopsy, the remaining 88 hepatic metastasis in 20 patients were diagnosed by follow-up. Follow-up imaging period was one month to 18 months, one month interval was considered the minimum time to assess the lesions as metastasis. The histopathological criteria for neoplastic grading is the measurement of cellular anaplasia (reversion of differentiation) and this increases with the lack of cellular differentiation, it reflects how much the tumor cells differ from the cells of the normal tissue they have originated from.4-9
As a control group, 82 adult volunteers with normal healthy liver were included in the study. Their hepatic healthiness were assessed and confirmed by blood laboratory tests (hepatic function tests). All volunteers were selected relying on the age and gender. Measurements were made by rounded region of interest in the areas far from vascular structures, ADC values of normal liver were obtained. In addition, maximum diameter values were recorded for all 3 groups.2,3 Region of interests (ROI) were positioned in the hepatic metastatic lesions and the average ADC values were calculated. In the larger and heterogeneous lesions with necrosis, hemorrhage, calcification, and so forth, ROIs were positioned to the homogeneous solid parts in order to clearly measure the ADC. Among 94 masses, 59 (62.8%) were poorly-differentiated adenocarcinoma, 18 (19.1%) were moderately-differentiated adenocarcinoma, and 17 (17%) were well-differentiated. Poorly, moderately, and well-differentiated masses were investigated according to diameters, ADC values, and ratio index (RI) values. Kolmogorov-Smirnov normality test was applied to evaluate the distribution characteristics of the variables. Depending on the normality test results, non-parametric statistical analysis methods were applied throughout the study. Kruskal-Wallis analysis of variance test was applied to understand the significance differences among all groups. Significance of pairwise differences was investigated with Mann-Whitney U test with Bonferroni correction. Descriptive statistics of variables were presented as median (minimum-maximum). To understand the possible correlations among variables, Spearman correlation analysis was used. Receiver operating characteristics (ROC) curve method was also applied to evaluate the possible cut-off values among study groups. Area under the ROC curves (AUC), sensitivity, and specificity values for each cut-off values were calculated. Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, USA) version 22 software. A p-value of <0.05 was considered statistically significant.
Results
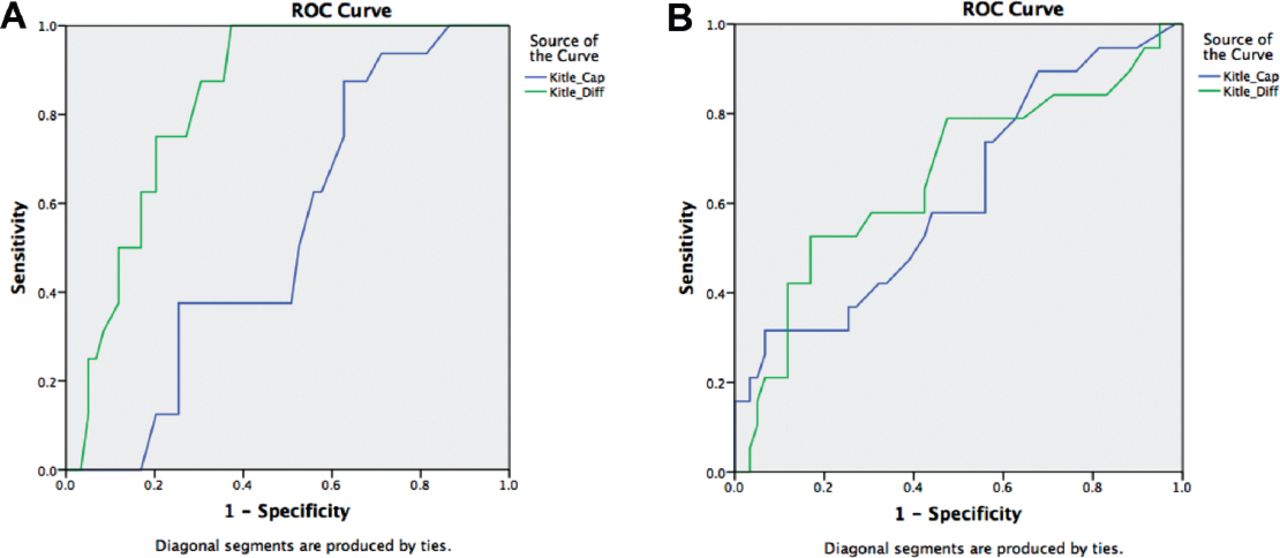
Statistical description of all variables of 3 groups were shown in Table 1. Apparent diffusion coefficient value of control group was measured as 1.04±0.11 and compared with average ADC values of the masses ratio index (RI). Lowest healthy ADC value of liver measured was 0.78, while the maximum ADC value was 2.2. When the values of these 3 groups were analyzed according to mass diameters, there was no statistically significant difference between the groups (p=0.111). Graphics of mass diameter variations are shown in Figure 1. There was a statistically significant difference (p=0.02) between all groups in terms of ADC values of masses. There were statistically significant difference in terms of ADC values between poorly-differentiated and moderately-differentiated adenocarcinomas and also between poorly-differentiated and well-differentiated adenocarcinomas (p=0.02). Poorly-differentiated adenocarcinomas had lower ADC values of masses when compared with both moderately-differentiated and well-differentiated groups. There was a significant difference for RI values between these groups as we observed in ADC values of masses. Statistically significant difference was observed for RI values between poorly-differentiated and moderately-differentiated adenocarcinomas and between poorly-differentiated adenocarcinoma and well-differentiated adenocarcinoma (p=0.008). Poorly-differentiated adenocarcinomas have significantly higher RI values with regard to both moderately and well-differentiated groups. In the well-differentiated adenocarcinoma group, significant positive correlation was observed between mass diameter variable and ADC values (r=0.569, p=0.006). Mass diameters showed significant negative correlation with RI values (r=0.569, p=0.006). In addition, for the moderately-differentiated adenocarcinoma group, similar significant correlations were observed. Significant positive correlation was found between mass diameter variable and ADC values (r=0.526, p=0.015). Mass diameters showed significant negative correlation with RI (r=0.526, p=0.015). Conversely, there was not any significant correlation between mass diameter and mass ADC variables or RI variable (p=0.07). Finally, analyses of ROC curves indicated whether the mass diameters and ADC values of moderately-differentiated and well-differentiated adenocarcinomas can distinguish them from poorly-differentiated adenocarcinomas. Regarding to the mass diameter and ADC values, ROC curves were drawn for poorly-differentiated and well-differentiated groups. Area under the ROC curves below the mass diameter for poorly-differentiated and well-differentiated groups was 0.53. The area under the ROC curve of ADC value was 0.83. A cut-off value was not suggested for a mass diameter between poorly and well-differentiated adenocarcinoma groups due to the low ROC curve area (0.53). For 0.83 AUC, an appropriate cut-off value, 0.665 was determined for ADC value of masses, with regard to sensitivity (87.5%) and specificity (69.5%). A similar ROC curve analysis was performed for poorly-differentiated and moderately-differentiated groups. The area under the mass diameter for poorly-differentiated and moderately-differentiated groups was 0.62. The area under the ROC curve was 0.66. Conforming to these results, the most appropriate cut-off value for mass diameter between poorly and moderately-differentiated adenocarcinoma was 21.5. As poorly and moderately-differentiated groups were differentiated as per diameter values, the sensitivity of the analysis was 73.7% and the specificity was 44.1%. The most appropriate cut-off value was 0.605 for ADC values of masses with 78.9% sensitivity and 52.5% specificity. Examples of metastasis of colonic adenocarcinomas were shown in Figures 2-3.
Descriptive statistics concerning mass diameters, mass differentiation, and ratios of the groups.

Graphics showing the A) mass diameter of the groups (there is no statistically significant difference between groups) and the B) mass apparent diffusion coefficient values. *difference according to poorly-differentiated adenocarcinoma (p<0.05), and C) ratio index of the groups. ADC - apparent diffusion coefficient

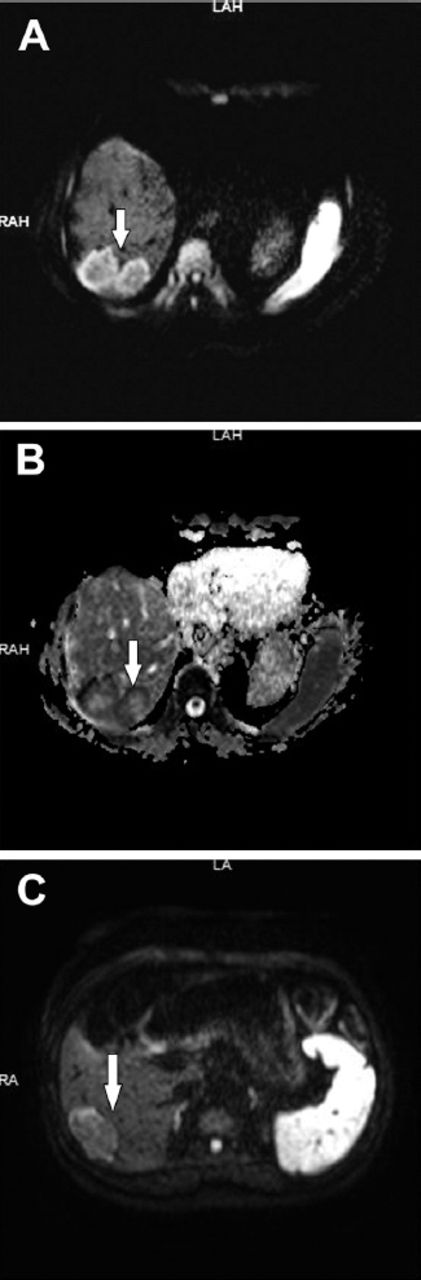
Two poorly-differentiated metastatic masses in right hepatic lobe of posterior segment 6 and moderately-differentiated metastatic mass in segment 7 of right posterior lobe, indicated by arrows (diffusion weighted imaging and apparent diffusion coefficient mapping).

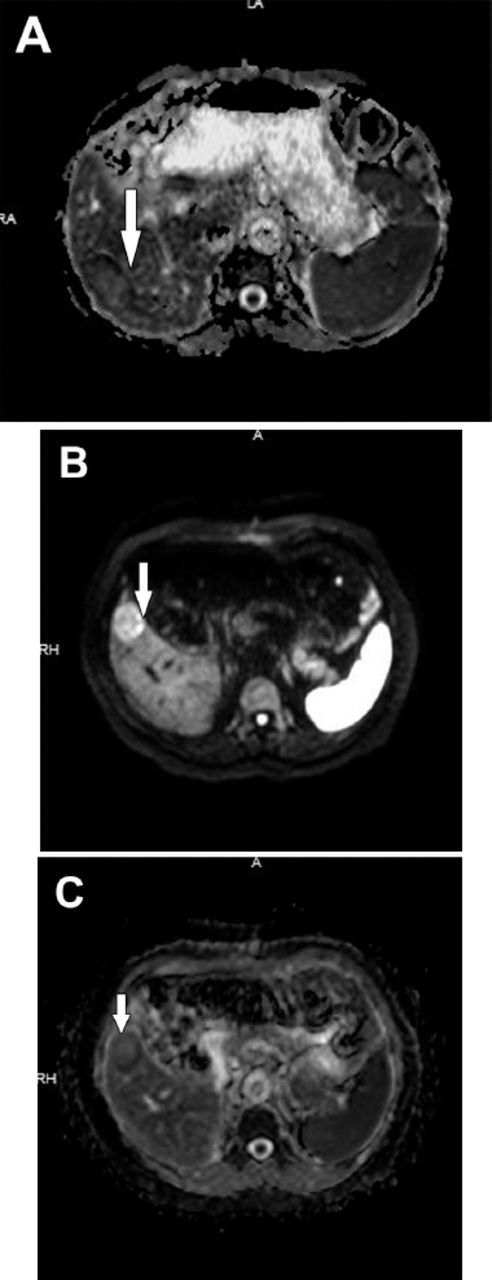
Moderately-differentiated metastatic mass in segment 7 and well-differentiated metastatic mass in segment 5 (diffusion weighted imaging and apparent diffusion coefficient mapping).

Receiver operating characteristics curves showing the A) mass diameter and apparent diffusion coefficient (ADC) values of masses for poorly and well-differentiated groups and B) poorly and moderately-differentiated groups with regard to diameter and ADC values of masses.
Discussion
Liver is the second most common organ for metastatic spread after lymph nodes.4 In 70% of all colorectal carcinomas, hepatic metastasis was presented at the diagnosis.5 Hepatic metastasis can be seen in any segment of the liver.4 Diffusion weighted imaging is routinely implemented in many centers in addition to conventional MRI sequences.6 It is widely used method in the diagnosis of early ischemia in cerebrovascular events, in cranial tumors and infections.7-9 The implementation of the method is increasing gradually in the evaluation of other parts of the body. For the first time in 1994, Muller et al10 used DWI for the diagnosis of focal and diffuse diseases of spleen, muscle tissue, and liver that revealed significant results with regard to healthy organ values. In the following years, diffusion coefficiency of tissues and lesions were calculated by DWI and it was shown that the different ADC values could be strictly beneficial in the differential diagnosis.11-17 Diffusion weighted imaging has significant contributions in the diagnosis of lesions and monitoring the response of oncology patients to treatment. There were few previous reports on DWI, determining and characterizing hepatic focal lesions.
Lower ADC values may represent hyper-cellularity, or malignancy. Therefore, DWI can be useful in predicting tumor grade or histopathological tissue differentiation. Diffusion velocity decreases by the increase of tissue cellularity. Previous study4 has shown that tumors with high cellularity have high metastatic capacity. Adenocarcinomas can be classified as well, moderately, and poorly-differentiated, or as low and high graded according to the dominancy of glandular structures. Well and moderately-differentiated adenocarcinomas are accepted as low grade, and poorly-differentiated adenocarcinomas are accepted as high grade.18 In our study, differentiation levels obtained from the histopathologic examination of adenocarcinoma metastasis are compared with the ADC values and a statistically significant difference was observed between poorly-differentiated adenocarcinoma, well and moderately-differentiated adenocarcinomas (p<0.05). Poorly-differentiated adenocarcinoma group has significantly lower ADC values compared with the both moderately and well-differentiated groups. However, there was no significant statistical difference between ADC values of well and moderately-differentiated adenocarcinomas. Likewise, statistically significant differences were observed between poor and moderately-differentiated adenocarcinoma, and between poor and well-differentiated adenocarcinoma (p<0.05) in terms of RI values. The poorly-differentiated adenocarcinoma group had significantly higher RI values when compared with both moderately-differentiated and well-differentiated groups.
The results obtained from this study indicated compatibility on histopathologic classification of adenocarcinomas. As mentioned before, well and moderately-differentiated adenocarcinomas were accepted as low grade and poorly-differentiated adenocarcinomas as high grade.18 The mean ADC value was 0.60 in poorly-differentiated adenocarcinoma in which glandular tissue density was low and the mean ADC values of moderately adenocarcinomas was 0.76 and well-differentiated was 0.78. The ADC values calculated for moderately and well-differentiated adenocarcinomas had a coincidence with a great extent.
In the ROC curves of poorly-differentiated and well-differentiated groups, cut-off value for ADC was 0.665 with 87.5% sensitivity and 69.5% specificity. Although the cut-off value for ADC was 0.605 between poorly and moderately-differentiated adenocarcinoma groups, the sensitivity was 78.9% and specificity was 52.5%.
Hayashida et al19 defined that histologic features of the brain metastasis can be predicted by DWI signal changes, and ADC values reflected cellularity of brain tumors. In recent years, the importance of quantitative ADC values gradually increased in the differential diagnosis of hepatic lesions, mean ADC values for focal lesions, or normal liver parenchyma showed differences in various studies. Goshima et al20 reported that ADC values of metastasis were between 0.94-2.85×10³ mm2/sec and ADC values of normal liver parenchyma were between 0.69-2.28 x10-4 mm2/sec, We found the mean ADC value for normal liver parenchyma as 1.04 ± 0.11 among 82 patients. The variability in ADC values was dependent upon the selected b-value (0-800) and to other technical parameters. Low b-values (<400) might cause high ADC values than assumed, and high b-values predicted low ADC values than assumed. Thus, MRI, DWI, and ADC mapping should be standardized. Also, DWI was not sufficient alone in the differential diagnosis of hepatic masses. Remarkably, cystic-necrotic changes inside the solid lesions might cause alterations in ADC values, and DWI examination should be evaluated together with other conventional MRI findings.21-23 It was also reported that there was overlapping of ADC values between benign hepatic masses, primary hepatic malignant masses, and metastasis.11,24-26 In our study, mean ADC values of moderately and well differentiated adenocarcinomas correlated to each other. Higano et al27 reported that mean ADC values of liver metastasis were 1.00 × 10-3 mm2/sec with b-values of 400 to 800. Hardie et al28 stated that DWI could be an alternative method to contrast enhanced MRI for detecting liver metastasis. It was also reported that DWI combined with conventional MRI, which was performed by using hepatocyte-specific agent was more convenient than DWI alone especially for detecting small colorectal tumor metastasis.29 In our study, there was no statistically significant correlation between mass dimensions and ADC values. Feurlein et al21 reported that ADC measurements also had an important role in detecting malignancy with addition to history, demography, and clinical findings. Ichikawa et al12 revealed that DWI had higher sensitivity and specificity in the detection of colorectal tumors. Tauli et al25 also reported that metastatic masses had the lowest ADC values among hepatic masses. Likewise, there were several studies11,24,30,31 indicating that ADC values were significantly lower in the other abdominal malignancies.
Quan et al32 was reported that there was not a significant difference between adenocarcinoma metastasis and HCC, the difference between mass ADC and liver parenchyma ADC was found to be significant (mean ADC in 11 HCC patients [0.93 ± 0.06] and mean ADC in 27 metastasis [1.09 ± 0.18]) In our study, there was statistically significant differences between ADC values for both adenocarcinoma metastasis and both between mass ADC values and liver ADC ratios. Magnetic resonance imaging, diffusion weighted MRI, and ADC values of hepatic metastases of gastrointestinal system malignancies were covered in this study, and some important and reliable informations were tried to be contributed to the relevant literature.
Main implication points of this research were the diagnosis of focal hepatic masses can be determined by ADC values solely in order to distinguish benign and malignant metastatic hepatic tumors.
Study limitations
The retrospective study design, which affects the statistics may cause bias to the results and may attenuate the implication of this study. Further study and validation by larger prospective are needed. 1.5 T with lower b-value (<400) may also limit the main aid and diagnostic potentials of this study; however, 3.0 T MR scanners and high b-value use (2000-3000) may provide more appropriate ADC values to assess the histopathological grading of liver metastasis of colonic tumors.
In conclusion, standardization of DWI can be provided together with the technical improvements in MRI and the differential diagnosis of focal hepatic masses can even be determined by ADC values alone to distinguish benign and malignant hepatic masses, whether it is primary or metastatic. In larger serial studies, cellularity of metastatic masses in addition to differentiation degrees can be determined.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received December 8, 2015.
- Accepted February 11, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.