


Abstract
Objectives: To assess the prevalence of common radiological variants of sinonasal anatomy among Saudi population and compare it with the reported prevalence of these variants in other ethnic and population groups.
Methods: This is a retrospective cross-sectional study of 121 computerized tomography scans of the nose and paranasal sinuses of patients presented with sinonasal symptoms to the Department of Otorhinolarngology, King Fahad Hospital of the University, Khobar, Saudi Arabia, between January 2014 and May 2014.
Results: Scans of 121 patients fulfilled inclusion criteria were reviewed. Concha bullosa was found in 55.4%, Haller cell in 39.7%, and Onodi cell in 28.9%. Dehiscence of the internal carotid artery was found in 1.65%. Type-1 and type-2 optic nerve were the prevalent types. Type-II Keros classification of the depth of olfactory fossa was the most common among the sample (52.9%). Frontal cells were found in 79.3%; type I was the most common.
Conclusions: There is a difference in the prevalence of some radiological variants of the sinonasal anatomy between Saudi population and other study groups. Surgeon must pay special attention in the preoperative assessment of patients with sinonasal pathology to avoid undesirable complications.
Radiological anatomy of the nose and paranasal sinuses (NPS) has many variants. These include deviation of the nasal septum, concha bullosa, Haller cell, Onodi cell, dehiscence of the internal carotid artery, and others. Resulting from the proximity of NPS to the orbit and skull base, addressing this region without sound knowledge of the anatomic variations can result in devastating complications during surgery. Computed tomography (CT) scan is the most precise imaging technique to demonstrate NPS. It evaluates the extent of inflammatory diseases and assesses important anatomical landmarks, and their variations.1-3 The advent of relatively less invasive techniques of functional endoscopic sinus surgery (FESS) has provided an important role for CT scan of NPS, both as a diagnostic tool and as an important part of preoperative planning. Its usefulness in the preoperative evaluation in patients undergoing FESS is not doubtful.1-4 Prevalence of radiological variants of NPS might differ among different ethnic groups as reported by Badia et al.5 Our study aims to assess the prevalence of common variants of NPS among Saudi population and compare the results with those reported in other ethnic and population groups.
Methods
This is a retrospective cross-sectional study conducted at King Fahad Hospital of the University, Khobar, Saudi Arabia after obtaining institutional review board approval (IRB 2014-01-329). The hospital is a teaching referral hospital that provides tertiary care services to a population of approximately 4.1 million in the Eastern province of Saudi Arabia.
We reviewed 195 preexisting CT scans of the nose and paranasal sinuses carried out in patients who visited the Otolaryngology-Head and Neck Surgery Department with sinonasal symptoms between January 2014 and May 2014. All patients underwent CT scan of NPS using the same CT system available in the institute. Scans were obtained using a bone algorithm in coronal, axial, and sagittal planes with slice thickness kept 3 mm at maximum. All CT scan films were reviewed using the Picture Archiving Communication System (PACS) (Siemens AG, Munich, Germany) software, and the results were reported in a data sheet. Entry and analysis of the data were carried out using the Statistical Package for Social Sciences (SPSS Inc, Chicago, IL, USA) Windows version 17.
Each scan was evaluated by a senior author for the presence or absence of agger nasi cell, Haller cell, Onodi cell, paradoxical middle turbinate, concha bullosa, pneumatization in the nasal septum and crista galli, septation of the maxillary sinuses, sphenoid lateral recess, intrasphenoid septation, and carotid artery dehiscence. Type of optic nerve, depth of olfactory fossa and type of frontal cells, if present, were also studied.
Of the initial 195 scans, 74 (37.9%) were excluded from the series as the sinonasal anatomy has been altered or obscured due to inflammatory disease (n=27), previous sinus surgery (n=21), and facial trauma (n=3). Scans of non-Saudi patients (n=9) and those younger than 18 years old (n=14) were excluded. The total sample size was 121.
A Medline search was carried out for the material for this comparison in the period from January 1980 to December 2014. The following keywords were used either individually or in combination: nose, paranasal, sinuses, sphenoid, frontal, optic nerve, anatomy, variants, variation, radiology, ethnic, computed tomography, CT scan, endoscopic sinus surgery, and climate. Further, relevant articles to our review were identified using the references that had been retrieved. The articles that were thought to be relevant to the original research work were identified and reviewed out of the 264 retrieved articles.
Results
Of 121 scans, 69 (57%) were for males and 52 (43%) were for females. The mean age was 33.2±12.02 years. The summation of the unilateral and bilateral abnormalities has been reported as the prevalence of variations without consideration of the “half-head” as separate entity. Areated crista galli presents in 108 (89.2%) scans. Pneumatization of the nasal septum was detected in 7 (5.8%) scans. Findings of agger nasi cell, concha bullosa, paradoxical middle turbinate, duplicated middle turbinate, maxillary sinus septation, Haller cell, Onodi cell, sphenoid lateral recess, intrasphenoid septa, and dehiscence of the sphenoid part of the internal carotid artery are summarized in Table 1.
Radiological variants of the nose and paranasal sinuses of 121 Saudi patients.
Review of the type of optic nerve according to DeLano et al6 were: type 1 in 58 (47.9%) scans, type 2 in 57 (47.1%), type 3 in 5 (4.13%) while type 4 was found in one (0.8%) scan only. Review of the depth of the olfactory fossa according to Keros7 were: class I in 8 (6.6%) scans, class II in 64 (52.9%), class III in 36 (29.8%), and class IV in 13 (10.7%) scans. Frontal sinus cells, according to Bent et al8 were present in 96 (79.3%) scans; one scan showed absence of the right frontal sinus. Type I was the most common (72 scans on the right side and 67 on the left). Type II was found in 16 scans on the right side and 18 on the left. Type III was found in 2 scans on the right side and 5 on the left, while type IV was found in 5 scans on the right and 6 on the left. Some scans showed different type of cells on either sides.
Discussion
Variations in the anatomy of NPS are well known and very common. The availability of CT scan, and other imaging modalities along with the development of sinonasal surgery have made physicians more interested in the radiological anatomy of NPS.2,3 During the study, we found few articles that address anatomy of NPS and its variations in Saudi Arabia and other Arab region; so are statistical studies of sinonasal pathologies. The current article represents a basic descriptive study that would aid in future research concerning sinonasal disease in the region. Of the various variants of NPS, we chose to analyze the prevalence of those considered in other similar studies that focus on ethnicity or specific-population. Also, we believe that the chosen variants are those encountered more frequently in the common practice of general otolaryngologists who perform common endoscopic nasal surgeries. Some variants, that we did not consider in our review, lack consistent systematic classifications that can be utilized to compare results between different authors or studies.
The difference in anatomic variations among different ethnic groups has been studied previously. Badia et al5 reviewed CT scans of 100 Chinese patients and compared with 100 Caucasians. They found significant differences in the occurrence of sinonasal anatomical variations among the 2 groups (Table 2).
Prevalence of common sinonasal radiological variants in Saudis and other study groups.
In this study, the presence of several sinonasal anatomical variants were analyzed despite their relevance to the patients’ original symptoms or pathology upon presentation. In addition, we did not consider whether the patient required surgical intervention, or not. Few studies, which we compared our results with, evaluated the presence of these variants in the setting of chronic rhinosinusitis or endoscopic sinus surgery. The size of our sample falls in the range of the sample size of other studies. Comparison of the occurrence of radiological sinonasal variants between our cohort and other studied ethnic and population groups revealed higher frequency of some variants among Saudis. Table 2 compares the prevalence of some variants between different study groups.
Agger nasi cell is the most anterior ethmoid cells. It borders the primary ostium of the frontal sinus. The patency of the frontal recess is affected largely by the size of this cell.1 We found agger nasi cell in 118 patients (97.5%) and was consistently bilateral. Its prevalence is comparable to that reported in Austria, Jordan, and Japan (Table 2).
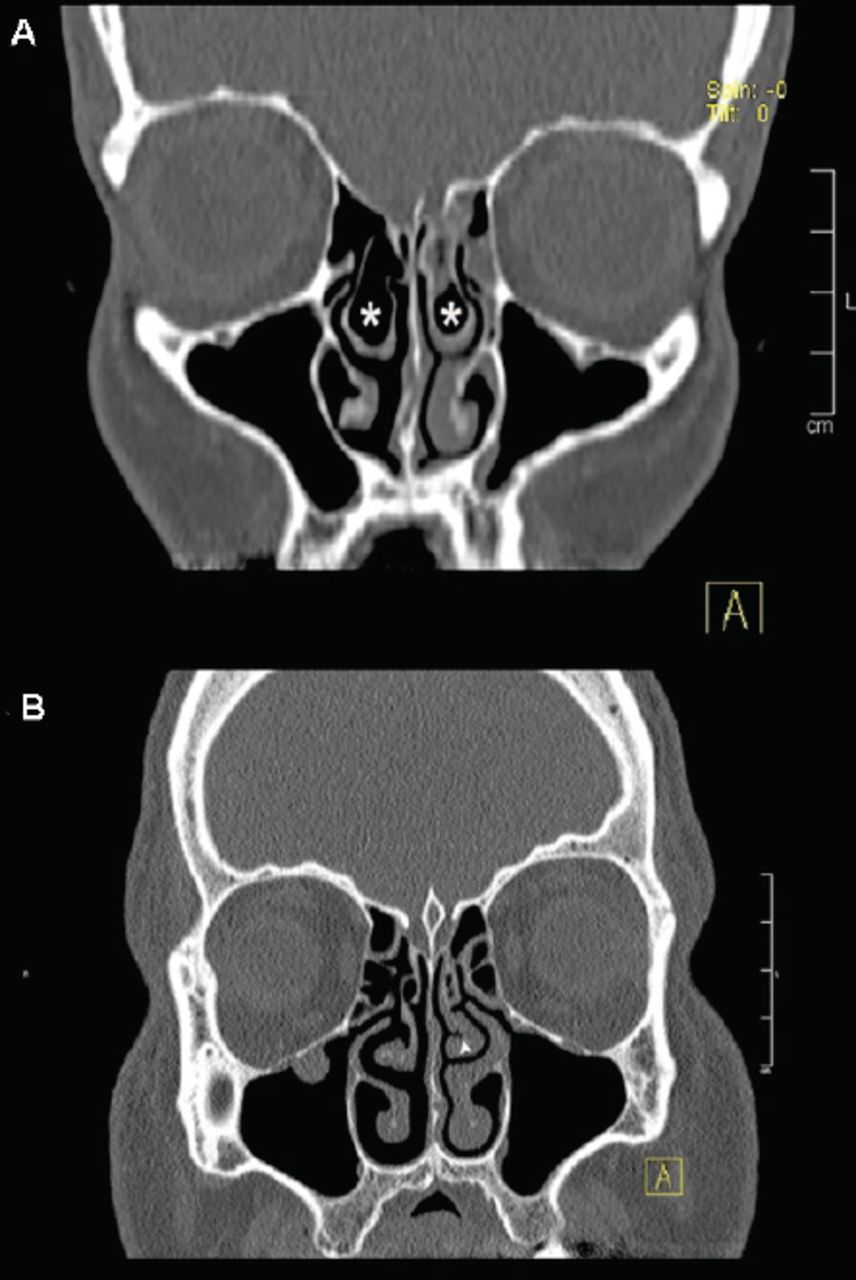
Pneumatization of the middle turbinate is referred to as concha bullosa. (Figure 1A) While some authors define true concha by pneumatization of both vertical lamina and the pulp, others consider pneumatization of any part as concha bullosa.20 We followed the second definition to avoid any inter-observer bias. The concha might block the ostiomeatal complex and pre-dispose to sinus diseases. It might also limit the surgical field exposure in certain cases. The prevalence of this condition has been reported largely in the literature with prevalence that ranges between 14-80%.20 The wide range of the reported prevalence might be explained by the difference in definition of concha bullosa followed by different authors. The finding of concha bullosa in our sample is quite higher than what is seen in other study groups (Table 2).
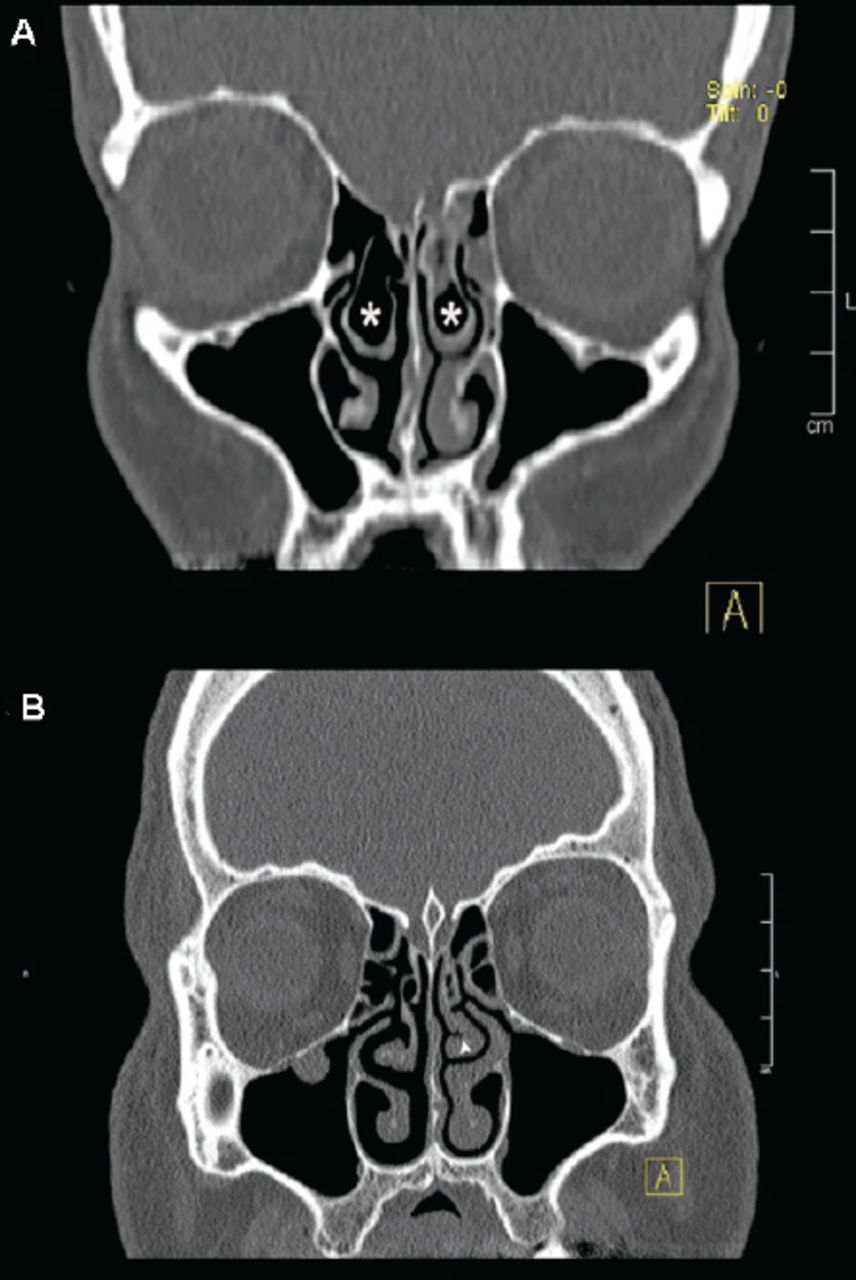
Variations of the middle turbinate. A) Concha bullosa, one of the prevalent variants among our sample, is shown here bilaterally (white star). B) Left paradoxical middle turbinate (white arrow head) with patent ostiomeatal complex.
Al-Dilaijan et al21 studied the prevalence of concha bullosa among symptomatic patients who underwent functional reconstructive nasal surgeries namely, septoplasty or septorhinoplasty with or without functional endoscopic sinus surgery. They found concha bullosa in 115 (59.9%) out of 192 patients; 60 (52.2%) of them had a unilateral concha bullosa while 55 (47.8%) had bilateral concha bullosa. Our findings of concha bullosa were comparable to their findings: Found in 55.4% of the sample, of them 50.75% was unilateral and 49.25% was bilateral (Table 1).
Paradoxical middle turbinate, defined as a projection of the curvature of middle turbinate laterally, is quite important. This condition might lead to chronic rhinosinusitis as it leads to narrowing of middle meatus and subsequently impaired ventilation1 (Figure 1B). This variant was found in higher percentage compared with most of other groups (Table 2).
The most posterolateral ethmoid air cell, known as Onodi cell, is an important variant to be assessed in any CT scan of NPS due to its close relation to optic nerve and internal carotid artery. The rate of Onodi cell in our group is comparable to Nitinavakarn22 group, but higher than the others as shown in Table 3 (Figure 2).
Onodi cells in Saudis versus other study groups.

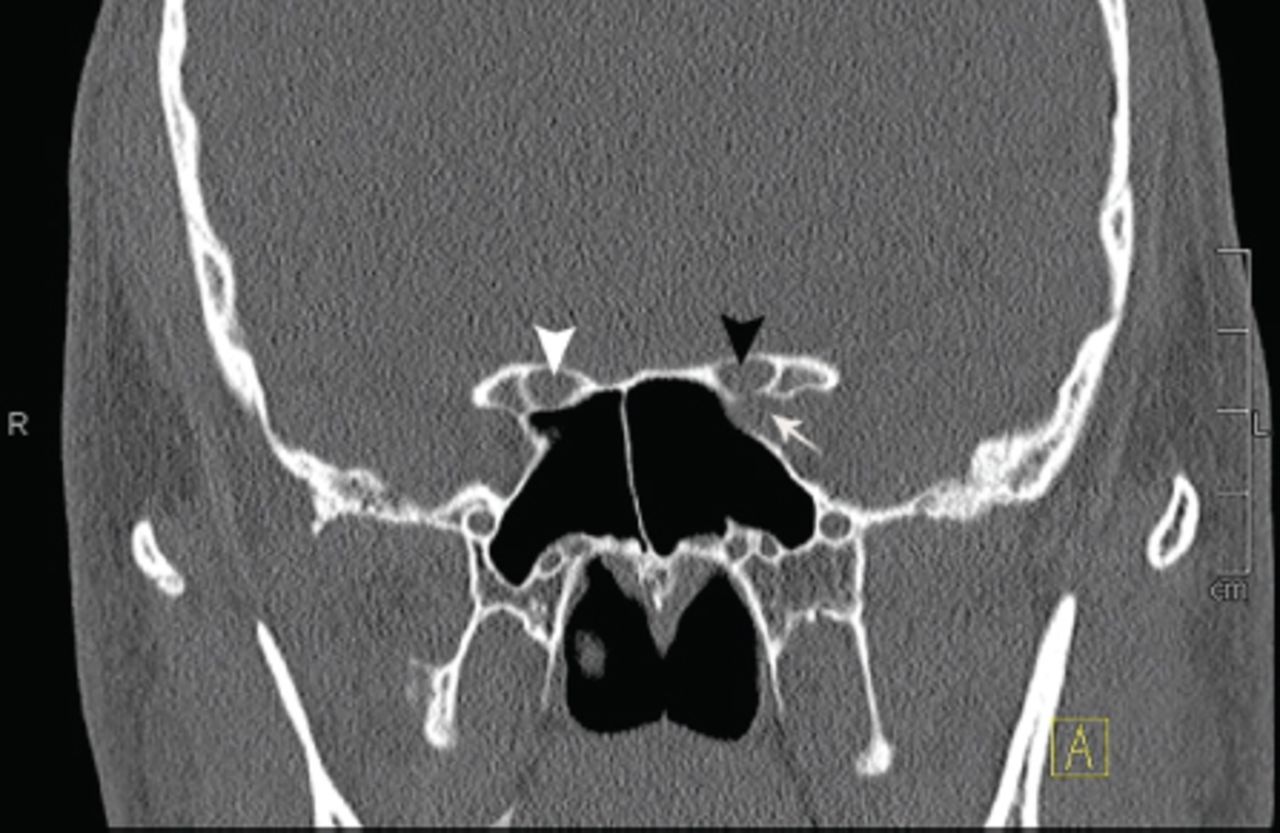
Variations of the posterior paranasal sinuses and related structures. Bilateral Onodi cell (white star), left dehiscent internal carotid artery (ICA) (white arrow). Optic nerve in relation to Onodi cell (black arrows).
DeLano et al6 described optic nerve in relation to sphenoid and posterior ethmoid sinuses into 4 types in their review of 300 patients. Type I described optic nerve adjacent to sphenoid sinus and found in 228 (76%) subjects. Type 2 described optic nerve with indentation on sphenoid sinus and found in 44 (15%) subjects. Type 3 described optic nerve traversing sphenoid sinus and found in 19 (6%) subjects. Type 4 described the nerve adjacent to both sphenoid and posterior ethmoid sinuses and found in 9 (3%) subjects. In comparison, type 1 and type 2 were almost equally prevalent in our group, while type 3 and 4 were rarely seen (Figures 2 & 3). We did not find studies addressing these findings based on ethnicity, but we think such comparison is important to emphasize the importance of this anatomic relation in endoscopic procedures addressing the posterior paranasal sinuses. Keros classify the depth of olfactory fossa into four types.7 Type II was found the most common in our group; followed by types III, IV, and I. Nitinavakarn et al22 reported type II as the most common type in their study in Thailand.

Variation of the sphenoid sinus and related structures. Left dehiscent internal carotid artery (ICA) (white arrow). Type 1 optic nerve on the left side passing adjacent to sphenoid sinus (black arrow head), while on the right side it passes with indentation on the sinus, type-2 (white arrow head).
The internal carotid artery (ICA) passes posterolaterally to the sphenoid sinus wall. Dehiscence of this segment, defined as absence of the bony wall separating the ICA from the sphenoid sinus, makes it vulnerable to high risk of injury during endoscopic surgery.24 Heiwaidi and Omami reported dehiscence in 90 patients out of 300 (30%) in their study in Libya.25 Siricki et al,26 in Turkey, found dehiscence in 21 patients out of 92 (22%). However, the rate is, generally, low at 1.5 to 5%.27 We found dehiscence in 2 scans (1.7%). Both of them were on left side (Figures 2 & 3).
We noticed that the presence of a variant on one side does not necessitate its presence on the other side. Moreover, one can have one variant on one side and another variant of the same structure on the other side, namely, concha bullosa on one side and paradoxical middle turbinate contralateral to it. Such findings should alert the surgeon to study each side of the CT scan separately with attention to these details to understand the underlying pathology and formulate a surgical road map preoperatively, if the patient is planned for surgery.
Research linking modern human nasal morphology with climate, however, has focused mainly on the outer nose and the nasal aperture. It has been suggested in many anthropometric studies that climate affects morphology of the external nose and adaptation of nasal aperture.28,29 Also, it has been suggested that the development of paranasal sinuses and craniofacial skeleton is affected by nasal airflow and positive air pressure in the nasopharynx.30,31 The weather in Saudi Arabia is generally hot in the central regions and hot with high humidity on the coasts. The finding of higher prevalence of some variants in our group could be attributed to the local climate conditions, but this assumption needs further investigations.
Ethnicity is another explanation for the difference in the prevalence of sinonasal variants. Our hospital provides services to eastern province population, which is, more or less, homogenous in origin compared with some other provinces. This postulation makes the sample size less representative of Saudi population. Therefore, a larger multicenter study is recommended
In conclusion, radiological anatomy of the nose and paranasal sinuses is complex with a wide range of normal variants. There is a difference in the prevalence of some variants among Saudi population compared with other study groups. Surgeon must pay special attention in the assessment of patients with sinonasal disease. However, further sinonasal disease-related statistical studies in Saudi Arabia and other Arab countries are undoubtedly recommended to understand behavior of sinonasal pathology in the Arab region.
Acknowledgment
All figures were reviewed by Dr. Saeed A. Al-Jubran (one of the author), Consultant Radiologist, Department of Radiology, College of Medicine, University of Dammam, Dammam, Saudi Arabia for clarity and correctness.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received November 5, 2015.
- Accepted March 14, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.