


Abstract
Objectives: To evaluate the association of vitamin D level with insulin resistance, among healthy student’s obese women, and to identify factors that may elucidate this association.
Methods: One hundred and forty-seven female students between the age group of 18 and 25 years were included in this cross-sectional study, and the related socio-demographic and anthropometric data were obtained. They were selected randomly from Aljouf University, Sakaka, Saudi Arabia between November 2013 and June 2014. Serum 25-hydroxy vitamin D (25[OH]D), glucose, insulin was measured and insulin resistance was calculated using the insulin resistance index (HOMA-IR).
Results: The results showed the percentage of 25[OH]D concentration in female students was 21.3% sufficient, 59.6% mild deficiency, and 19.3% moderate deficiency. The percentage of waist circumferences (WC) were 41.3% (>88 cm) and 58.7% (<88 cm), body mass index (BMI) was 13.6% (obese) and 31.8% (over weight), blood pressure (BP) was 65.7% (<130/85 mm Hg), and 33.2% (>130/85 mm Hg). Based on the cut-off point of 25[OH]D, 17.4% of females had 25[OH]D deficiency, 27.3% insufficient, and 55.3% sufficient. When the females were classified according to the BMI category, the serum 25[OH]D concentrations for obese was the lowest value (54.6%) when compared with the overweight (31.8%) and normal weight (0.9%). 25[OH]D was inversely associated with BMI, fat%, and HOMA-IR.
Conclusion: Our results suggest that vitamin D deficiency is prevalent in women of Saudi who are university students especially in those who are obese. Preventive interventions in order to reduce the tendency of deficiency among college students should focus on the awareness of the essentiality of vitamin D promotion of direct exposure to sunlight (vitamin D3) and consumption of vitamin D fortified food as a part of Saudi diets.
Low vitamin D levels have been seen in one-third of the developed countries.1 A high prevalence of hypovitaminosis D occurs in the Middle East and the North African region, and it is more prominent in women of varying ages.2 A low level of vitamin D is highly prevalent, even in the normal population of the Kingdom of Saudi Arabia (KSA).3,4 Only a few studies have been conducted to evaluate serum 25-hydroxy vitamin D (25[OH]D) levels among the young. The best indicator of vitamin D status is determined by serum 25(OH)D concentrations as it reflects total vitamin D from dietary intake and sunlight exposure.1 Serum 25(OH)D values of <50 nmol/L reflects vitamin D deficiency, and <75 nmol/L reflects vitamin D insufficiency.1 However, some studies suggest that the optimal level of vitamin D status is 50 nmol/L.5 Obesity is associated with a lower level of 25(OH)D in adults and adolescents.6 Based on the body mass index (BMI), children and adolescent obese was 17.1%, according to the United States National Health and Nutrition Examination Survey (NHANES; 1999-2000).7 Vitamin D status is inversely associated with BMI,8 but the causality of this association is uncertain. Obesity has now become an epidemic. The overall percentage of overweight and obese individuals is 47.9%. Among Saudi female university students, approximately 17.4% were obese and 54.2% were overweight.9 There is limited information on the relationship between weight and 25(OH)D level, although in a population, there is a prevalence of vitamin D deficiency, especially in low socioeconomic groups.10 Previous study8 have found an inverse relation between obesity and 25(OH)D level, thus suggesting that adipogenesis may be prevented by the intake of one 25-(OH)2D3.11 Moreover, lower levels of 25(OH)D have been found among obese individuals who take vitamin D supplements and are exposed to UV light compared with non-obese individuals.12 An imbalance in hormones and the metabolism of nutrients may be accompanied by obesity resulting in an increased in insulin resistance and progressive insulin insufficiency associated with visceral fat.13 Nutritional factors, gender, diet, season, and level of physical activity have also been associated with body fat and 25(OH)D.14 Studies performed in KSA reveal an increase in the incidence of obesity due to changes in lifestyle.15 Female adults suffering from obesity are usually sedentary and rarely go outdoors and thus getting limited exposure to sunlight.16 This illustrates the development of Vitamin D deficiency. The bioavailability of vitamin D in obese subjects might be due to the deposition in fat tissues.17 We hypothesized that the level of vitamin D was altered in healthy obese adults (aged 18-25 years) making them predisposed to changes in the level of insulin resistance. The aim of this study is to evaluate vitamin D levels and their association with insulin resistance in healthy female students who are obese, and to identify the factors that may explain this association.
Methods
Study subjects
A total of 147 female students aged 18-25 years were included in this cross-sectional study. They were selected randomly from Aljouf University, Sakaka, KSA between November 2013 and June 2014. We screened them on the basis of their health-information. All candidates suffered from liver diseases, kidney diseases, or diabetes mellitus, or have taken any medication that could affect bone disease and vitamin D status in the past 3 years or who have a history of thyroid, parathyroid, adrenal, or gonadal diseases have been excluded. Other exclusion factors were pregnancy or lactation, and a history of convulsions. All subjects provided their informed consent in writing after the study and its objectives were explain to them. The study was approved by the Medical Research Ethics Committee, Faculty of Medicine, King Saud University, KSA.
Anthropometric measurements
Height in cm and weight (up to an accuracy of one decimal point) were measured, and their body mass indexes (BMI) were calculated.18 Waist and hip (W/H) circumferences were measured and their ratio was calculated.18 Diastolic blood pressure (DBP) and systolic blood pressure (SBP) were measured in the right arm of each subject after they remained in a sitting position after 5 minutes.19 Anthropometric measurements were carried out in sample groups after removal of outer garments and shoes.
Biochemical analyses
Blood samples were taken after fasting, the serum was separated after clotting, and frozen at -20°C until it was analyzed. Glucose level in the serum was estimated by the glucose oxidase technique, while 25(OH)D and insulin were estimated by the enzyme-linked immuno-Sorbent assay (ELISA) (IDS, Tyne and Wear, UK). The inter-assay variability for the 25(OH)D ELISA was 5.2%, and the intra-assay variability was 4.3%, and for the insulin ELISA, inter-assay was 5.7%, and intra-assay was 3.1%. Insulin resistance was calculated from fasting plasma measurements using HOMA-IR (insulin [mU/L] × glucose [mg/dl]/405).20 Vitamin D status was classified as deficient (<20 ng/ml), insufficient (20-29 ng/ml), or sufficient (>30 ng/ml).21
Statistical analysis
Numerical data were expressed as mean ± standard deviation (SD) using the software Statistical Package for Social Sciences version 15 (SPSS Inc., Chicago, IL, USA). Analysis of variance was carried out for the comparison of the groups. Spearman correlation analyses were also carried out. The probability p=0.05 was considered significant.
Results
Table 1 illustrates the demographic characteristics of the female students. The ages were between 18 and 25 years, with a mean age of 20.71 ± 0.17 years.
Demographic characteristics of 147 female students attending the university.
Table 2 illustrates The percentage of 25(OH)D, WC, BMI, and BP levels of female students. Severe vitamin D deficiency was not observed.
The percentage of 25-hydroxy vitamin D (25[OH])D, waist circumference (WC), body mass index (BMI), and blood pressure (BP) levels of female students attending university.
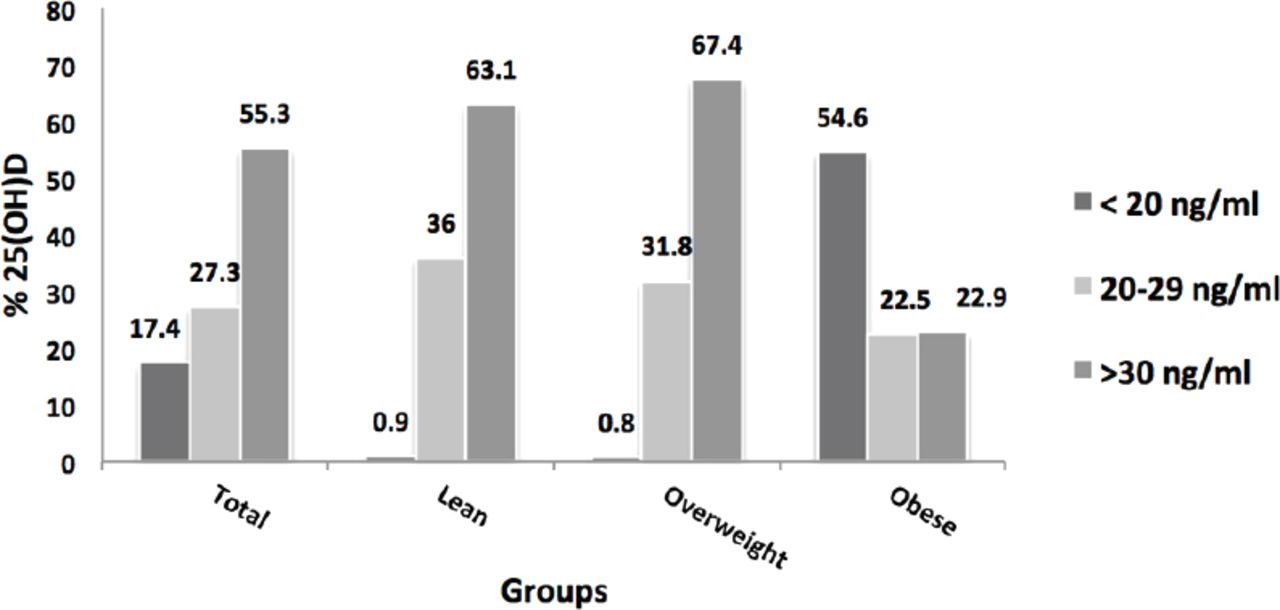
Figure 1 shows the distributions of circulating 25(OH)D concentrations according to the BMI categorized for female students. Based on the cutoff point, the final levels of serum 25(OH)D was within the normal range, but somewhat in the lower side. Approximately 17.4% of the female students had a deficiency of 25(OH)D, 27.3% had an insufficient level, and 55.3% had a sufficient level. When the subjects were classified according to BMI, the serum 25(OH)D concentrations was the lowest for the obese subjects (54.6%) as compared with the overweight subjects (31.8%), and subjects with normal weight (0.9%). This implies that the risk of vitamin D deficiency was greater in obese people than in overweight people and people with normal weight (Table 3).
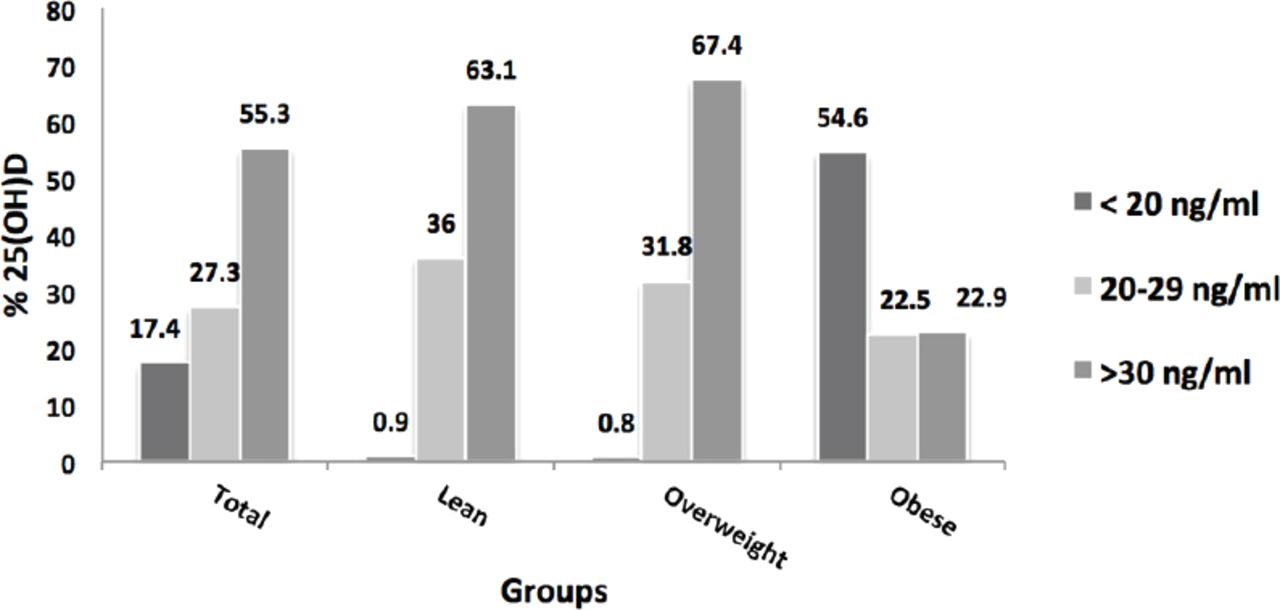
The percentage of 25-hydroxy vitamin D (25[OH]D) for normal, overweight, and obese in Saudi female students attending universities. The distributions of circulating 25(OH)D concentrations according to the body mass index (BMI) categorized among female students. Approximately 17.4% of the female students had a deficiency of 25(OH)D (<20 ng/ml), 27.3% had an insufficient level (>20-29 ng/ml), and 55.3% had a sufficient level (>30 ng/ml). When the subjects were classified according to BMI serum 25(OH)D concentrations was the lowest for the obese subjects (54.6%) as compared with the overweight subjects and subjects with normal weight.
Serum glucose, insulin and insulin resistance index (HOMA-IR) levels according to body mass index (BMI) classification in female students attending university.
Table 4 illustrates the correlation coefficient of 25(OH)D with other parameters. A significant inverse correlation was discovered between 25(OH)D and BMI, fat percentage and HOMA-IR in the female students (p=0.000, p=0.001, p=0.002).
Correlation coefficient between 25-hydroxy vitamin D (25[OH]D) and other parameters among female students attending university.
Discussion
Obesity is a major public health problem and is a risk factor for vitamin D deficiency. An inverse correlation between obesity and 25(OH)D level was observed in several studies, Parikh et al,10 reported an inverse relationship between circulating concentrations of 25(OH)D, BMI, and body fat mass. Exposure of the skin to the sun leads to high levels of vitamin D in the body. However, the level of 25(OH)D continues to have an inverse association with BMI among obese people who take vitamin D supplement and are expose to UV light.21 In the present study, serum 25(OH)D concentrations were found to be lower in obese females as compared with those who were overweight, or had a normal weight.
The prevalence of vitamin D deficiency characterized by the level of serum 25(OH)D lower than <20 ng/ml, was found to be common among obese female students (54.6%) who were healthy. The female students were found to have a deficiency of 17.4%. Several scholars have found a high prevalence of vitamin D deficiency among Arabian women,22 as well as women in other ethinicties.23-25 Ardawi et al,24 found a high prevalence of vitamin D deficiency in Saudi female students attending universities, with vitamin D levels <27 ng/mL. Severe hypovitaminosis D has been observed in more than 52% in young Saudi women, with 25(OH)D levels were <8 ng/ml.25 A number of factors may contribute the low level of vitamin D including insufficient synthesis and other factors may lead to inadequate intake or absorption of 25(OH)D. Furthermore, the dietary intake of vitamin D among Saudi women found to be lower than the recommended level (15 µg daily).26
With regard to the present data, more than half (54.6%) of the obese female subjects were found to have lower levels of vitamin D, while 22.5% had insufficiency levels, and 22.9% had sufficient levels. The low levels of 25(OH)D in obese individuals combined with the storage of vitamin D in the subcutaneous fat tissue lead to a reduction in its bioavailability.27 Furthermore, the low levels of 25(OH)D might be attributed to other factors such as sedentary lifestyle of obese individuals. Such a lifestyle is associated with fewer outdoor activities and reduced exposure to sunlight, which may in turn reduce the production of endogenous vitamin D and therefore, lead to a vitamin D deficiency. Saudi food sources are usually low in vitamin D (this coupled with the limited intake of foods) may also be contributing to the lower levels of vitamin D.28,29 Earlier studies show a link between body fat and vitamin D deficiency, and also demonstrated that low levels of vitamin D can be a risk factor for various diseases, such as osteoporosis, autoimmune diseases, heart disease, and various types of cancer.30,31 The present study shows significant inverse correlation between 25(OH)D and BMI (p<0.000), fat percentage (p=0.001), and HOMA-IR in female students (p=0.002). This result is consistent with other studies.30,31 Al-Daghri et al,32 observed that there is a relation between vitamin D status and insulin sensitivity in Saudi women. The sensitivity of insulin is lower in women who are vitamin D deficient compared with those who are vitamin D-sufficient. A possible mechanism by which deficiency of vitamin D, may affect insulin sensitivity is the elevation of parathyroid hormone levels by the regulation of intracellular free calcium concentrations in target cells. The stimulation of the expression of insulin receptor promotes insulin responsiveness for the transport of glucose indicating that vitamin D may also play a role in insulin action.
With respect to the relation between vitamin D and obesity, we found the significant decline in vitamin D levels due to obesity, which is consistent with the findings of similar studies.33-35 A study conducted on adult females found that the reduction of weight by 10% was accompanied by a significant increased of up to 34% in vitamin D levels compared with the baseline (15.4 to 18.3 ng/ml; p<0.05).36 Another study,37 a weight reduction programme (12 week) in premenopausal women reported that the levels of vitamin D increased by 2.9 ng/ml (from 30.3 to 33.2 ng/ml). Yanoff et al38 found that the effect of adiposity on vitamin D status is independent of dietary intake, socioeconomic factors, gender, and age. This supports the hypnoses that vitamin D is linked to BMI and body fat. Some studies39,40 also suggest that vitamin D is a potentially important in the prevention of certain cancers, autoimmune diseases, heart disease, and hypertension.
In conclusion, this study suggests that vitamin D deficiency is prevalent in female Saudi who are university students especially in those who are obese. This hypovitaminosis of vitamin D is an independent predictor of insulin resistance. Vitamin D is known to be an important mediator of insulin resistance. Preventive interventions in order to reduce the tendency of deficiency among college students should focus on the awareness of the essentiality of vitamin D promotion of direct exposure to sunlight (vitamin D3) and consumption of vitamin D fortified food as a part of Saudi diets. We need further research to ameliorate vitamin D supplementation that elucidates the underlining mechanism of vitamin D receptors and absorption through measuring genetic expression vitamin D3 as important directions for newer therapies.
Acknowledgment
The authors gratefully acknowledge the Deanship of Scientific Research, Aljouf University, Sakaka, Kingdom of Saudi Arabia in helping to carry out this work.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received September 28, 2015.
- Accepted January 26, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.