


Abstract
Objectives: To estimate the rate of the Pilonidal disease (PND) recurrence and to evaluate the associated predictors of the recurrence.
Methods: This is a retrospective study, conducted at King Fahd Hospital of the University in Alkhobar, Kingdom of Saudi Arabia over a period of 10 years from January 2003 until December 2013.
Results: A study of 366 with PND, 19 of those were identified as secondary cases and excluded. Most involved 347 patients were Saudi (82.1%), single (87%), and men (93.1%). The mean age of the sample was 23 ± 8 years, and the mean body mass index (BMI) was 29.7 ± 6 Kg/m2. Overall recurrence rate after the surgical management was found in 25 patients (7.2%). By logistic regression to the recurrence group, young age group, prolong sitting and BMI may increase the likelihood of the disease recurrence.
Conclusion: Pilonidal disease still has challenges in its management. Treatment should depend on the extent and severity of the disease. The recurrence rate in this study is approximately 7.2%. The most predominate factors associated with recurrence were prolong sitting job, young age group, and high BMI.
Pilonidal is literally from the Latin words pilus and nidus which means a nest of hair. Pilonidal disease (PND) is a common clinical problem that leads to decrease in work productivity, especially in healthy young adults. It defines as an infection under the skin that usually occur in the gluteal region.1 It is also reported to occur in the umbilicus and the interdigital spaces.2,3 The incidence reaches to 26/100,000 person with 3:1 male predominance.4 It can be presented as an acute inflammation with a collection of pus, or a chronic sinus that is chronically draining pus. However, the disease can be asymptomatic and undertreated. In a surveillance study of approximately 19,013 candidates, pilonidal sinus was detected in approximately 6.6% of the candidates.5 The aim of this study is to estimate the rate of the disease recurrence and to evaluate the associated predictors of the recurrence.
Methods
This study is a retrospective study that reviews all primary cases of PND who were managed in the King Fahd Hospital of the University in Alkhobar, Kingdom of Saudi Arabia during the period from January 2003 until December 2013. We got the approval of institutional review board at the University of Dammam for the study. The correctness of the diagnosis confirmed by correlating the theater note and the discharge summary. Data collection include patient demographic data, clinical presentation, clinical management, and recurrence rate. In this study, prolong sitting job is defined as the job, which required sitting for more than 6 hours per day as an automobile driver, student, and so forth. All secondary cases who presented with PND and treated before were excluded from this study. All cases of inflammatory bowel disease, hidradenitis suppurativa, perianal fistula, furuncle, or carbuncle were excluded. Patients were diagnosed having recurrent disease through outpatient clinic follow-up if one of the following feature developed as prescribed by Doll et al6 complete wound healing postoperatively, no history of trauma after wound healing, developing one hard criterion (surgical re-intervention, a formation of a new sinus, presence of hair in a sinus opening and discharge of pus) or 2 soft criteria (wound redness, swelling, pain and discharge of fluid).6
The sample was allocated into 2 groups; acute and chronic. For this study purpose the diagnosis definition of acute PND is the presence of acute inflammation or acute collection; with or without sinus while the chronic disease presented with an intermittent or chronic draining of pus.
The surgical technique as described in the operative note was either lay open or primary midline closure. Lay open technique is wide excision of the pilonidal sinus with leaving the wound to be healed by secondary intention. The other technique was excision of the sinus with primary midline closure.
Data analysis were carried out using the Statistical Package for the Social Sciences version 20 (IBM Corp., Armonk, NY, USA). Arithmetic mean used as a summary of the quantitative data. The standard deviation used as a measure of dispersion. Chi-square test and Student t-test used for analytic statistics. Kaplan-Meier Statistics Graph was used to estimate the recurrence rate over a period. Multiple regression was applied to determine the significant predictor of recurrence. P-value of ≤0.05 was considered significant for all statistical analysis.
Results
A 366 PND cases were allocated, 19 of them were identified as secondary PND and excluded. The remaining 347 primary cases were involved in this study. The overall recurrence rate after surgical management found in 25 patients (7.2%). The vast majority of the sample were male (93.1%), Single (87.0%), and Saudi (82.1%). Approximately one-third of the sample has a prolong sitting job. One hundred twenty-seven of the sample presented as acute disease and required urgent surgical intervention. The remaining 220 patients were presented as chronic disease and were managed electively, as shown in demographic Table 1.
Demographic characteristics of 347 patients with pilonidal disease.
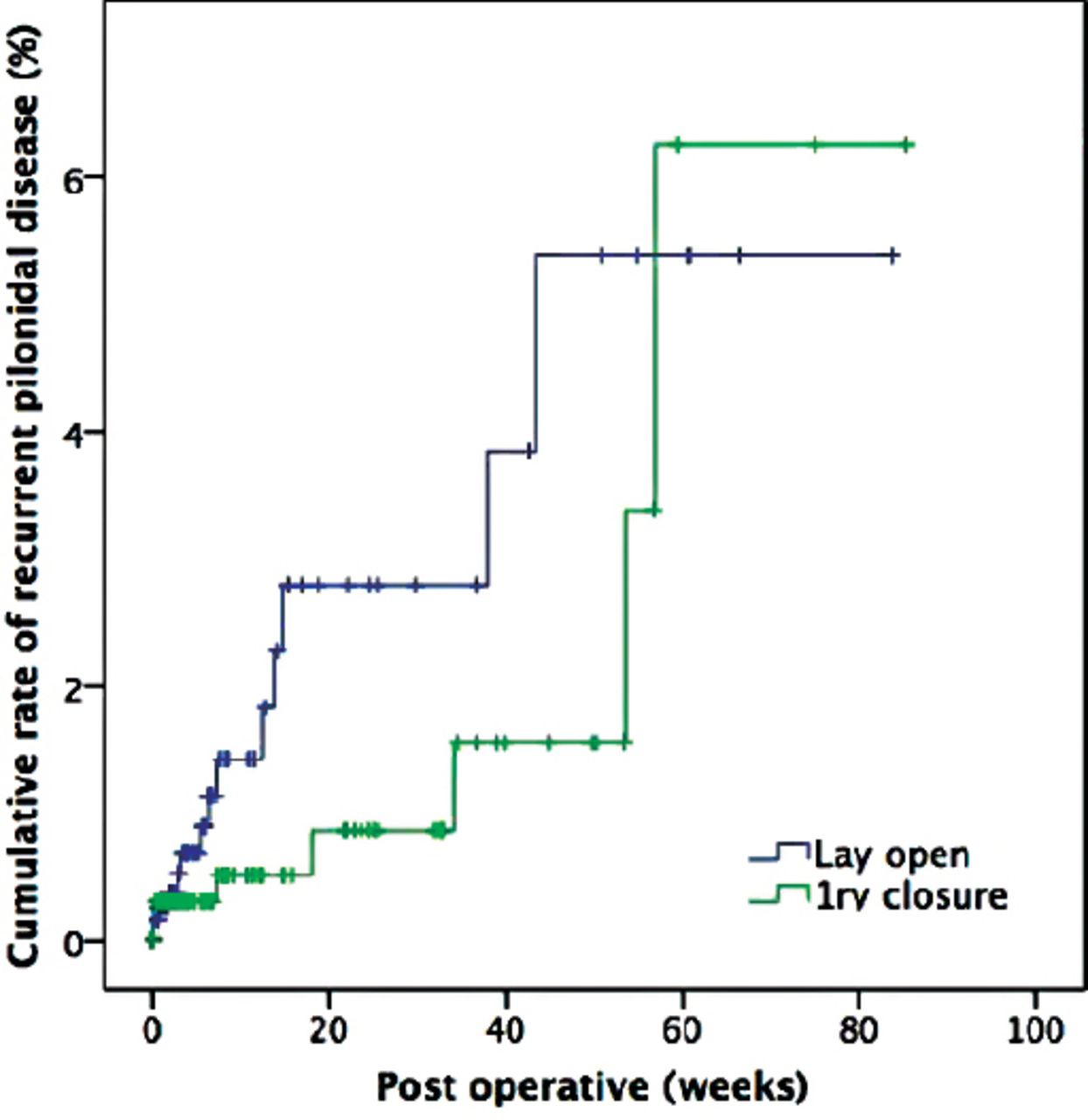
A median follow-up period of 2 weeks (1 to 85 weeks) of 347 patients involved in the study until the end of the study period of December 2013. Within 85 weeks, 7.2% had a recurrence of PND during the follow-up. Figure 1 shows the Kaplan-Meier curve of the cumulative recurrence rate in PND during the 1.6 years following discharge with a wide separation between the 2 treatments curves and higher recurrence rate at the end of the study with primary midline closure.
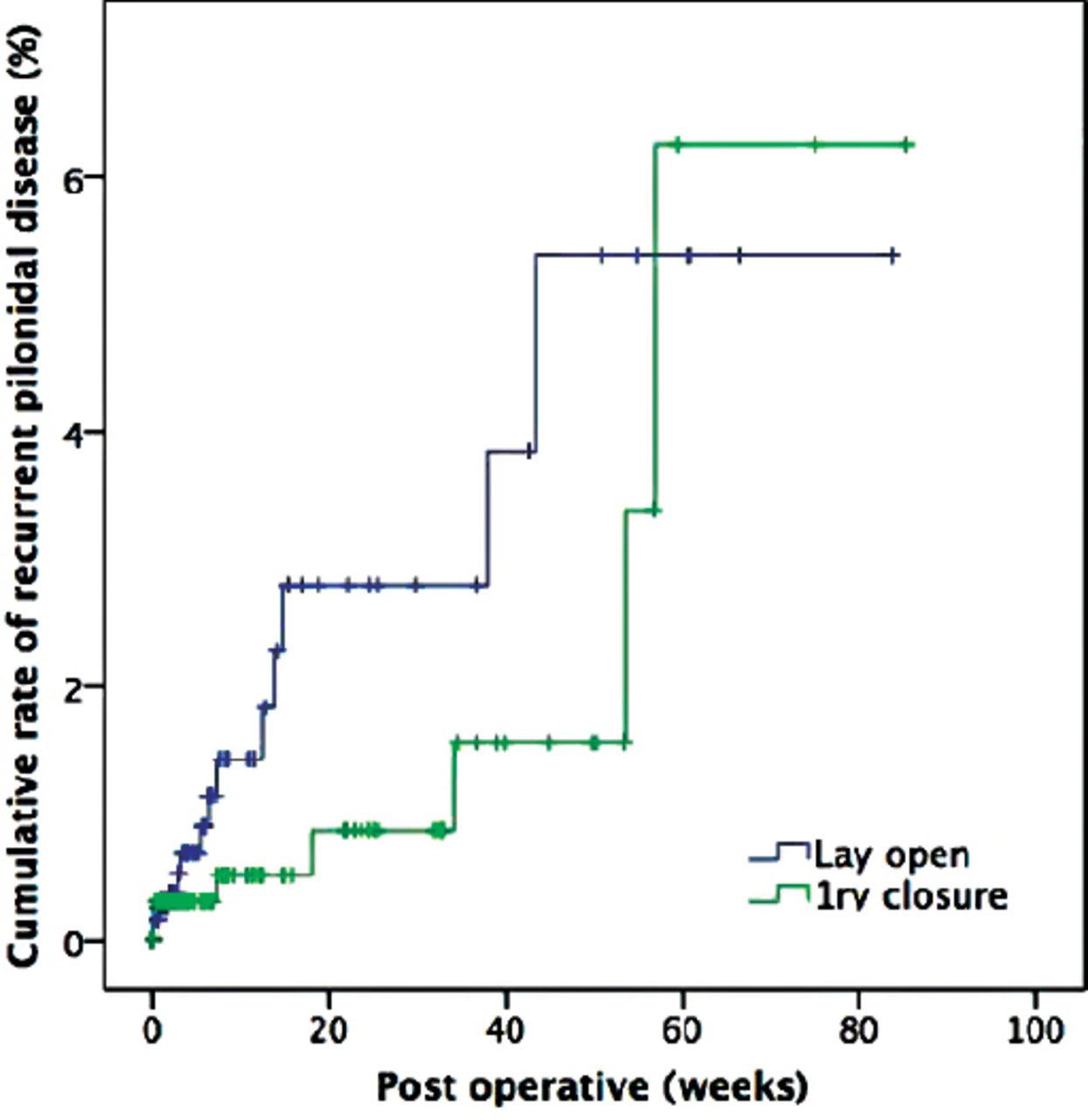
Kaplan-Meier curve of recurrent pilonidal disease in patients following discharge; p=0.17 log-rank test.
The surgical intervention of almost all cases who presented with the acute disease was drainage of the collection with lay open the wound to be healed by secondary intention except for 5 cases underwent closure of the wound over a drain. On the other hand, 45.8% of the patients who presented with chronic disease were managed with excision of the sinus and primary midline closure of the wound. The mean hospital stay of the patients was 4.4 ± 4.6 days (Table 2).
Surgical management of the acute and chronic groups.
A logistic regression was performed to ascertain the effects of age, gender, occupation, smoking, body mass index (BMI), chronicity, type of the operative, measurement of the depth intra-op and post-op antibiotic on the likelihood that participants have recurrence of PND.
The logistic regression model was statistically significant, χ2(4)=40.640, p<0.001. The model explained 29.3% (Nagelkerke R2) of the variance in pilonidal recurrence and correctly classified 92.9% of cases.
Young age was associated with increased likelihood of exhibiting recurrence by 1.19 times. Depth measurement by methylene blue showed 0.27 decrease likelihood of recurrence with a statically significance of 0.03. A BMI with a p-value of 0.05 may also play a role in disease recurrence as shown in Table 3.
Logistic regression for predictor factor of recurrence.
Discussion
The pathogenesis of PND still being in the debate. It could result from a congenital sinus from a failure of coalescence of the primitive ectoderm.7 However, most surgeons accept Karydakis’s theory that the disease is acquired with hair penetrance plays the basic role of the disease. It depends on 3 factors. The loose hair plays the first factor as an invader, which applies some force to be inserted into the skin depending on its vulnerability.8,9 The patient occupation may also play a role in the disease development, in military service members, 11% of cases develop recurrence.10 Levinson et al11 found that male combatant and female driver have the highest risk of developing PND among soldiers.
Many factors found to have an association with the PND. Family history is one of the non-modifiable risk factors for developing PND.12,13 Furthermore, prolong sitting or driving more than 4 to 6 hours with less number of baths per week considered to be a risk for PND.12,14 Bolandparvaz et al12 added overweight with BMI more than 25 Kg/m2 to be significantly associated with the development of PND. Weight reduction and regular baths are important preventive measures to reduce the disease risk occurrence. Our study shows a high mean BMI of 29.7 ± 6 Kg/m2.
Surgical procedure of PND can be conducted using spinal or general anesthesia with no difference between them in the recurrence rate or postoperative pain.15 When PND presented with asymptotic midline pit, the German National Guidelines do not advocate surgery to treat these cases as it has no advantages over surgery of symptomatic patients in terms of decreasing recurrence rate.16
Acute PND presentation with pus collection should be treated with incision and drainage as the mainstay management with delay of the definitive treatment after resolution of local inflammation.16-18 However, adding skin excision and curettage to the incision and drainage of pilonidal abscess shows to decrease the rate of recurrence with chronic sinus.19 Hussain et al20 successfully treated acute abscess collection with aspiration and administration of antibiotics aiming to avoid urgent surgery and leaving the wound open. Most acute cases in our study managed with drainage and lay open the wound technique.
Many surgical techniques prescribed for the treatment of chronic pilonidal sinus involving wide excision with leaving the wound open, limited excision with sinusectomy or sinotomy, primary midline or off-midline closure, and flap based procedures. The ideal technique should be simple, less painful, low cost, can be carried out under local anesthesia with low recurrence rate and shorter time to get back to daily activities.9 Meta-analytic studies showed lower recurrence rate of wide excision leaving the wound open compared with primary closure. However, primary closure wound heals faster.21,22 Off-midline closure has a clear favor over midline closure in terms of decreasing recurrence rate, rate of wound infection and wound dehiscence.21-23 Practice guidelines advocate using off-midline closure to be the standard measure when deciding to close the wound.16,17 The American Society of Colorectal Surgery leaves the method of the treatment to be based on the surgeon and the patient preference, while using the flap-base procedure for the complex and multiple-recurrence chronic disease.18 Milone et al24 studied the use of drain in PND surgery and found no benefit of using a drain in decreasing rate of infection or recurrence.24 Minimally invasive procedure for treating sacrococcygeal pilonidal sinus using video-assisted endoscopy is emerging. It shows to be effective, safe, with faster return to work and daily activities.25,26
Post-operative wound care is one of the important measures studied in the literature. Biter et al27 did not show a benefit of using negative pressure wound device over the standard wound dressing in fastening the healing time.27 Application of local gentamicin collagen sponge over the wound may decrease the rate of surgical site infection with no influence on the disease recurrence.28 The use of laser depilation still lacks reliable data to support its recommendation.16
Doll et al’s6 study stated that recurrence could be up to 22 years with a long follow-up, however, it is not practical to follow up all patient for 22 years. Three-quarter of the recurrence will occur in the first 5 years post-surgery.6 Smoking and BMI fail statistically to have an influence on wound healing or disease recurrence.29,30 Alptekın et al31 demonstrate a higher recurrence rate to be encountered when higher specimen volume excised. This study demonstrates a recurrence rate of 7.2% with a median follow-up of 1.6 years.
The study was limited by relatively small study population that was taken from a specific geographical area with convenience sampling and short follow-up time than other studies.
In conclusion, PND still has challenges in its management. Treatment should depend on the extent and severity of the disease. The recurrence rate in this study is approximately 7.2%. The most predominate factors associated with recurrence were prolong sitting job, young age group, and high BMI.
Acknowledgment
The authors thank Ibrahim A. Alsultan, Ridha H. Alghnnam, and Mohammed A. Alabandi from the University of Dammam, Dammam, Kingdom of Saudi Arabia for their contribution in form of data collection, entry, and in checking the correctness of medical records.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received July 11, 2016.
- Accepted October 19, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.