


Abstract
Objectives: To describe the effectiveness of HIV guidelines in prevention of mother-to-child transmission (PMTCT).
Methods: A retrospective review from January 2009 to December 2018 at the King Abdulaziz University Hospital (KAUH), Jeddah, Kingdom of Saudi Arabia. The main outcome measures were characteristics of HIV-exposed patients and transmission rate.
Results: A total of 18 HIV-positive mothers and their 26 infants were included. The mean age of mothers at delivery was 31.69 years, and 50% were under 30 years old. All mothers received lifelong ART, except one who was not diagnosed until the 27th week of gestation. Among the mothers, 83% complied with treatment regimens, and 11% had ART resistance. Human immunodeficiency virus polymerase chain reaction (PCR) was undetectable in 19 pregnancies. Seven mothers had opportunistic infections and treatment was immediately initiated. After reviewing the infants’ HIV PCR tests, the transmission rates of HIV were 0% for both spontaneous vaginal delivery and cesarean section.
Conclusion: Many challenges face the efforts to decrease vertical HIV transmission, and a particular focus on the transitions between stages of care is needed. We believe that early screening, counseling, and regular follow-up have contributed to MTCT elimination.
There has been a noticeable increase in the extent of the human immunodeficiency virus (HIV), impacting individuals, population health, and economic growth.1 In Saudi Arabia, 10,217 HIV cases were recorded between 2000 and 2009; this number has been increasing each year.2 The high incidence of HIV brings to attention the need to establish multiple strategies that minimize the prevalence rate. The Saudi Ministry of Health (MOH) has reported that total elimination of HIV would be achieved by 2030, through the “90-90-90: Strategy for the Eradication of HIV.”3 This is applied by early HIV screening so that medical treatment can be provided before symptoms develop, which will reduce patient mortality and prevent HIV spread.4 Previously, screening was voluntary and only for pregnant women at high risk for HIV infection.4,5 Nowadays, screening is mandatory during antenatal visits, to prevent mother-to-child transmission (MTCT) of HIV. Mother-to-child transmission can occur in utero, intrapartum, and through breastfeeding, the cumulative rate of MTCT of HIV without medical care was 35-40%.1,6 Furthermore, transmission could be minimized to less than 1% through adherence to antiretroviral therapy (ART) during gestation.7 Furthermore, the optimal mode of delivery may reduce the rate to less than 2%.8 Polymerase chain reaction (PCR) tests are reliable in detecting HIV during gestation and in the neonatal period.9
This study aimed to review the approaches followed at the King Abdulaziz University Hospital (KAUH), Jeddah, Saudi Arabia, with HIV-positive mothers and infants outcomes from 2009 to 2018.
Methods
This is a retrospective descriptive study targeting all HIV-positive mothers and their delivered infants from January 2009 to December 2018 at KAUH. The ethical committee of KAUH has approved this study. We excluded 3 infants: 2 twins considering the high risk of infection in the firstborn twin, and one infant whose file could not be accessed. Our sample size included 18 HIV-positive mothers aged 24 to 50 years old and their 26 infants. The mothers were already known cases of HIV except for one who was diagnosed, in the 27th week of pregnancy during antenatal visits, based on enzyme-linked immunosorbent assay (ELISA) and Western blot tests. Descriptive data were created for all variables, based on KAUH’s strategies followed by the AIDS Clinical Trials Group Protocol 076 to reduce the risk of MTCT of HIV,10 consisting of the mother’s current treatment, compliance, and resistance to ART, and immunologic and virologic statuses.
Other variables were near-term CD4 T-lymphocyte counts (categorized as <200 cells, 200-399, and ≥400 cells/mm3), intrapartum prophylaxis, and mode of delivery. Antenatal visits and coinfections diagnosed in pregnancy were recorded as well as gestational age measured by ultrasound (US). Newborn data included HIV PCR tests and HIV antibody measurements calculated at birth and 2 to 4, 6, 12, and 18 months. It also comprised infant gender, birth weight, Apgar score, postpartum prophylaxis, and breast feeding status. All data were obtained from the medical records, and infants who lost to follow-up in the pediatric clinic were reported. Simple descriptive statistics including percentages, means, and standard deviations were calculated using Microsoft Excel.
Results
We reviewed the medical records of 18 mothers and their 26 infants delivered at KAUH between 2009 and 2018. The mean age of mothers at delivery was 31.69 years, and 50% were under 30 years old. All of them were prescribed lifelong ART before pregnancy, except for one mother who started ART at 27 weeks of pregnancy. During 15 of the pregnancies (65.2%), the mothers were receiving nucleoside reverse-transcriptase inhibitor (NRTI) therapy plus a protease inhibitor (PI); in 4 pregnancies (17.4%), the mothers were receiving NRTI/non-nucleoside reverse-transcriptase inhibitor (NNRTI) therapy; in 2 pregnancies (8.7%), they were on NRTI/PI/integrase inhibitor (IH); in 1 pregnancy (4.3%), the mother was on NRTI/IH; and in 1 (4.3%), the mother was on NRTI/NNRTI/PI.
Table 1 details the types of ART used by the HIV–positive mothers for each pregnancy concerning their CD4 cell counts. Fifteen mothers were compliant with their treatment regimens while 3 were not compliant, because of either depression or expiration of ID (iqama), and one mother had an unknown reason in her 3 pregnancies. Antiretroviral therapy resistance was noticed in 2 cases; one was a non-compliant mother with depression for one year, who developed resistance to the NRTI emtricitabine and was then assigned to a PIs/NRTI combination (boosted lopinavir, Truvada, and raltegravir). The other patient acquired resistance to the combination NRTI/NNRTI/PI and was treated with boosted lopinavir, lamivudine, and efavirenz, which was later switched to the NRTI/PIs (Truvada, boosted darunavir and raltegravir). Twenty of the 26 pregnancies (76.9%) ended with vaginal delivery. Eighteen of the patients who delivered vaginally had undetectable viral loads; however, 2 had CSs planned but delivered by emergency SVD instead. Their viral loads reached 49,421 and 4,245 copies/mL. Six pregnancies were delivered by CS: 4 were associated with a viral load of more than 1000 copies/mL, and the remaining 2 had undetectable viral loads (one was accompanied with AIDS and a history of pulmonary tuberculosis, while the other had the obstetric indication severe preeclampsia).
- Types of ART used in the treatment of HIV–positive mothers in relation to their CD4 cell counts.
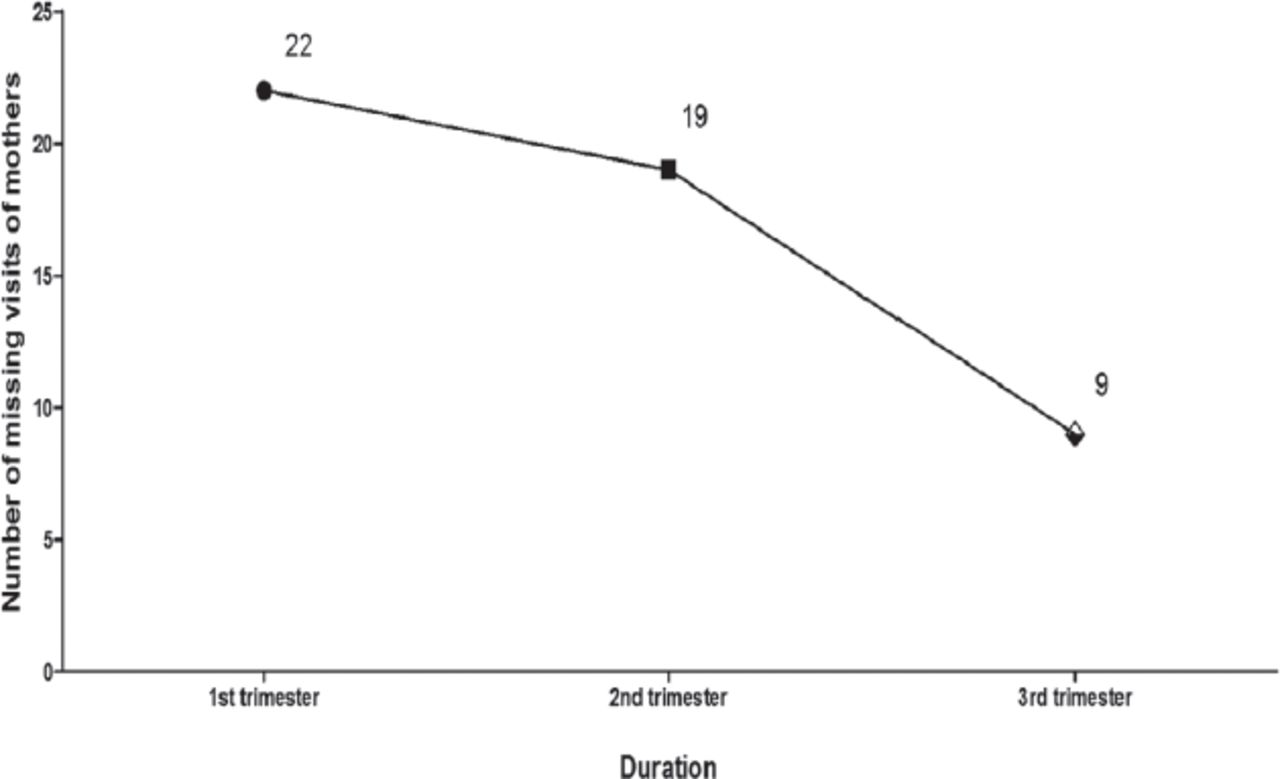
Table 2 summarizes the deliveries of the HIV-positive mothers in relation to total deliveries each year, compliance with ART in the antenatal period, and the effect of viral load on the mode of delivery. All mothers received zidovudine (AZT) prophylaxis during labor as part of hospital protocol. Opportunistic infections were found in 7 mothers (during 11 pregnancies), with one of the following infections for each: disseminated cytomegalovirus, Pneumocystis carinii pneumonia, intra-abdominal tuberculosis, Human papillomavirus type 6, Candida esophagitis, cryptococcosis of the central nervous system, and pulmonary tuberculosis. All mothers started treatment at the time of diagnosis. There were 18 recorded antenatal visits for 26 pregnancies. The highest number of visits were registered in the third trimester; as they became closer to their due dates.
- Number of deliveries of the HIV–positive mothers related to total deliveries each year, their compliance to ART antenatally, and the effect of the viral load on mode of delivery (N=26).
Figure 1 shows the number of missed antenatal visits. Each of the 26 newborn babies was carefully checked after birth by 1- and 5- minute Apgar scores: 1-minute scores were recorded for 25 of the newborns, and the score was missing for one newborn. The lowest scores were found in 2 newborns, who scored 2 and 6 out of 10 (8% of the cases), indicating that the infants required ventilation assistance and immediate resuscitation. However, in 96.2% of the cases, the 5-minute Apgar score was reassuring. The infant mortality rate was 0.04 (3.8%), which was a case with severe intrauterine growth restriction (IUGR).

- Missed antenatal visits of HIV-positive mothers for each pregnancy (N=26).
Table 3 shows an overview of newborn characteristics. Human immunodeficiency virus PCR results of samples that were collected after birth were undetectable for all newborns. None of the newborns proved to have HIV infection since there were no 2 consecutive positive HIV PCR assays confirmed. Furthermore, the HIV-antibody test was positive in 4 cases. Laboratory test results are summarized in Table 4.
- Characteristics of HIV-positive mothers’ newborns (N=26).
- Laboratory test results for HIV-exposed children, (N=25)*
Figure 2 shows the number of HIV-exposed infants who were lost to follow-up for unclear reasons.

- Number of HIV-exposed infants lost to follow-up (LTFU) (n=25*). *Excluding one infant who died immediately after birth.
Discussion
The most significant policies legislated to restrict HIV transmission in Saudi Arabia include lifelong ART for HIV-positive women and AZT prophylaxis during labor. For the newborn, exclusive formula feeding plus AZT prophylaxis starting from birth to 6 weeks of life will decrease the risk of transmission to less than 2%.11,12 In some settings, these strategies may not be sufficient to prevent MTCT of HIV and HIV antigens could be detected. This study was designed to describe the PMTCT of HIV between 2009 and 2018 at KAUH and to discuss how HIV screening tests could change the epidemiology of HIV in Saudi Arabia. Maternal HIV viral load is considered the most critical factor in determining full viral suppression after the initiation of ART by the time of delivery.13 A study has reported that HIV transmission rates were 20% for untreated women and 1.2% for women receiving ART.14 In this study, ZDV was used during the intrapartum period, following the AIDS Clinical Trials Group 076 Protocol,10 to reduce transmission risk. According to this study, the majority of the mothers had undetectable viral loads by the time of delivery (64.4%), and eventually, the transmission rate was zero. These low rates were comparable to other studies.15,16 Moreover, we observed no transmission among 9 cases with detectable viral loads, due to either failure of diagnosing HIV at the right time or inability to control HIV replication because of nonadherence to regimens.17,18
The data in the study described the loss to follow-up (LTFU) in infants after delivery, based on clinic schedules. The median ages at first and last infant follow-up visits were 3 weeks and 18 months, respectively. The reason for their LTFU could be that when the infant’s first HIV PCR result is negative, the mother dismisses further follow-up.19 The major challenge facing today’s PMTCT care program is keeping the patients under medical care, typically up to 24 months of age. A meta-analysis of HIV-exposed infants showed that their LTFU within 3 months of birth was 33.9%.20 These analyses determine the magnitude of LTFU, which is critical to the global PMTCT response. Exploring the reasons for LTFU may be used to inform further policy development and resource allocation for PMTCT programs to achieve the elimination of pediatric HIV infection in the Kingdom of Saudi Arabia.
Our findings also emphasize the ongoing need for preconception care of HIV-positive women,because they present later in pregnancy than what is recommended by current guidelines.21 This study strongly emphasized the implementation of research to evaluate ways to improve the integration of services,22 particularly transitions from antenatal to delivery and pediatric care. A variety of research-based studies suggest strategies to improve follow-up care for HIV-exposed infants, such as an integration of services,22 male husband,23 active patient tracking,24 nutritional supplements,25 use of mobile technology for reminders,22 and accompaniment between clinics.26
Although the interpretation of infant outcomes in the study was limited due to LTFU even with available DNA PCR results, outcomes were excellent, especially among infants whose mothers were compliant within the PMTCT care program. A previous study noted that 35% of HIV-positive infants not receiving ART were expected to die during the first year of life and 52% by 2 years of age.27 These findings support that follow-up and early initiation of ART will suppress the viral load, slow disease progression, and reduce mortality rates.27 Additionally, the study did not adequately identify women at risk. However, since the overall rate of transmission was statistically equivalent to zero, it suggests that large-scale prevention applications have the potential to achieve superior results.
The principles of MOH recommendations for HIV screening of pregnant women have remained unchanged for a long time in Saudi Arabia. Human immunodeficiency virus screening was voluntary and offered only for high-risk women during antenatal visits,28 and the MOH has enforced the HIV screening test for all pregnant women as a routine part of prenatal care in 2019. There remains a particular challenge facing the screening program. For instance, screening services are unacceptable among Saudi individuals, partially due to lack of awareness about HIV and not expecting that it exists in Arab, Muslim cultures. Instead, most men and women do not realize that they are potentially at risk. Often, these limitations have served to not adhere with the guidelines,29 even with the established laws by the Bureau of Experts at the Council of Ministers; a Saudi citizen who is infected with HIV is entitled to free medical care and has the protection of his or her privacy.30 Even though, we acknowledge that effective programs are complicated by social barriers, stigmatization, and discrimination associated with the disease, all of which may prevent individuals from seeking voluntary HIV testing and counseling.31
Finally, the screening test should be modified to ensure that it is accessible across the country, such as to the 17.9% of the population living in rural areas.32 More awareness campaigns, educational seminars, and innovative healthcare policies for attracting Saudi pregnant women to undergo HIV screening tests are fundamentally needed.
Intrapartum care for HIV-positive mothers includes 2 mg/kg/hour of AZT followed by 1 mg/kg/hour administered intravenously as soon as signs of labor begin and until the infant is delivered. Within the first 8 to 12 hours after birth, the newborn infant should receive AZT syrup 2 mg/kg/dose every 6 hours for 6 weeks. If the mother’s viral load is above 1000 copies/mL, CS is preferred to prevent MTCT, and AZT must be administered 3 hours before the procedure and until the newborn is delivered. Otherwise, vaginal delivery is recommended.28 There is no need to isolate the mother or her baby; however, breast feeding is contraindicated. Postpartum care for HIV-exposed newborns includes referring to an infectious disease pediatrician to determine the baby’s status. The diagnosis of HIV in exposed infants depends on serial blood tests: HIV antibody test (ELISA), and HIV viral load measurements (PCR test).33
Study limitations
While the present study provides insights into the prevention of MTCT of HIV, it has been affected by some limitations. First is the small number of enrolled subjects which may affect the generalization of our findings among all Saudi regions. The second limitation is being conducted from a single center which may carry some sort of selection bias and affects the credibility of our results. Nonetheless, we believe that this report is a preliminary groundwork for future research in Saudi Arabia aiming to curb HIV transmission to newborns.
In conclusion, ensuring HIV screening for all pregnant women is crucial to detect the disease and prevent transmission to newborns. Various studies have assessed the efficacy of screening tests, counseling, ART, elective CS, breastfeeding avoidance, and early ART for newborns; and all have contributed to MTCT elimination. Therefore, it is important to establish HIV/acquired immunodeficiency syndrome (AIDS) awareness and educational efforts together with mandating HIV screening programs and linking to care which can lead to MTCT elimination in the community.
Acknowledgment
The authors gratefully thank Editage for their language editing services.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received June 20, 2021.
- Accepted August 10, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.