


Abstract
Objectives: To determine the impact of applying the best available clinical evidence on the preventive measures to reduce the rate of catheter-associated urinary tract infections (CAUTI) in adult intensive care units (ICU).
Methods: Data were collected from adult ICUs (28 beds) from 2008 to 2016. The proper use of silicon catheter, aseptic insertion technique, emptying bag three-fourth via close circuit, the use of appropriate size catheter, securing the draining tube on the thigh to keep catheter bag below patient’s bladder level and removal of the catheter as early as possible were ensured in all patients.
Results: Rate of UTI and urinary catheter utilization ratios were reviewed during the study period. There was a mean of 6,175 catheter days/year for ICU. Despite the overall rise in the urinary catheterization ratio over these years; we observed a significant reduction in the UTI rate per 1000 Urinary catheter days; from 2.3 in 2010 to 0.3 in 2011 and it was sustained through 2016.
Conclusion: The monthly rates of CAUTI significantly declined after the enforcement of agreed strategies and interventions to prevent CAUTI rates in adult ICU.
Indwelling urinary catheter insertion is common practice in adult intensive care units (ICU) for accurate measurement of urinary output mostly in critically ill and post-operative patients, as well as patients with poly trauma requiring prolonged immobilization, and many of other appropriate indications.1 Nonetheless, these urinary catheters are accounted for 20% to 30% of healthcare associated infections (HAI) resulting in high cost due to over use of antimicrobials, increased length of stay in ICU, hospital stay, morbidity and mortality.2 Catheter-associated urinary tract infections (CAUTI) is the second leading cause of blood stream infection next to Central Line Associated Blood Stream Infection (CLABSI).2 The risk factors for CAUTI with symptomatic urinary tract infection (SUTI), includes prolonged catheterization with each day of catheter in situ increases the incidence of bacteriruria by 3% to 7%, female gender, older age, immune-compromised, diabetes mellitus, orthopaedic, neurological conditions and critically ill patients.3 The risk factors for blood stream infections from CAUTI include neutropenia and renal impairment and is linked directly and indirectly to increasing morbidity and mortality.3 As per National Health Care Safety Network (NHSN) data from 2006 to 2007, CAUTI rate was 3.1 infections per 1000 catheter days in medical and surgical intensive care units.4 The recent surge in the awareness of CAUTI prevention potential lead to many healthcare societies to work on current literature review to improve the outcome in CAUTI rate by practicing evidence based best practice guidelines. The concept of Bundle approach, the integrated synergistic effect of a group of evidence based practices was introduced by the Institute of Health Care Improvement (IHI) in 2001 and first applied for CLABSI prevention resulted in remarkable success rate. Since then the approach has been suggested for CAUTI but no universally accepted CAUTI Bundle been recommended so far.5
King Abdulaziz Medical City, Jeddah is more than 550 bed tertiary care hospital affiliated to King Saud bin Abdulaziz University for Health Sciences serving National Guards and their eligible dependents in the Western Region of Saudi Arabia. Adult ICU is composed of 4 main units with bed capacity of 32 (28 commissioned and 4 non-commissioned beds) with an average of 1000 admissions per year. It serve all medical, surgical, trauma, and oncology patients. The ICU is covered by qualified consultant intensivists at any given time, and managed through a multidisciplinary closed system, however, it is supported by all subspecialty consultants round the clock.
In spite of rigorous infection prevention control campaign and practice in our hospital which is one of the most advanced centre in the Western Region, the CAUTI rate remained high 2.3 in 2008 to 2010 which was a major concern. The intensive care department and the infection control team considered this as an area of quality improvement opportunity; hence, a multidisciplinary CAUTI team was established with an objective of reduction of CAUTI rate in our adult ICU.
The aim of this study was to test the impact of applying the best available clinical evidence interventions on the rate of CAUTI in adult ICU.
Methods
Design
At King Abdulaziz Medical City, Jeddah, a multidisciplinary team was created in Adult ICU in January 2011, that include members from Intensive Care Department, Infection and Prevention Control Department and the ICU Nurse Manager. Infection Control Practitioner acted as the coordinator of the team meetings.
The multidisciplinary CAUTI team reviewed the recent evidence based clinical practice guidelines and comprehensive recommendations for diagnosis, and prevention of HAI, for CAUTI in intensive care units, the expert guidelines from Society of Healthcare Epidemiology of America (SHEA), Infectious Diseases Society of America (IDSA) revised guidelines published in 2010, Centres for Disease control and Prevention (CDC) Guidelines in 2009, Health Care Infection Control Practices published Advisory Committee Guidelines (HICPAC) published in 2009, Infection Control Manual, Chapter 6, from Infection Control Department of King Khalid University Hospital, Riyadh, Kingdom of Saudi Arabia were reviewed in details.6-9
As no definitive CAUTI Bundle has been recommended so far, the team adopted the best available and supported data of CAUTI interventions. 8 components were adopted which include; 1) screening all patients on ICU admission, 2) using only the silicon type of foleys catheter, 3) aseptic techniques, insertion, 4) emptying bag three-fourth via close circuit, 5) choosing the appropriate catheter sizes, 6) securing the draining tube on the thigh, 7) keep catheter bag below patient bladder level and not touching the floor, and 8) removing the catheter as soon as possible.
Strategies
The multidisciplinary team identified three champions from 3 departments; physician, nursing and infection control to educate, monitor and achieve the set targets of this quality project. Educational sessions were organized to the Champions by the Infection Prevention Coordinator under the leadership of ICU Chairman and ICU Nurse Manager to understand the magnitude of the problem and its preventive nature: Set prevention target with timely reduction goal, compliance to the interventions. Good communication, and establishing patient safety culture. Subsequently, these educational sessions were conducted periodically to the entire ICU nurses and staff and competencies were obtained by the staff before the project started. Physicians were trained on the Patient Screening on admission to identify the appropriate indications of the urinary catheter, daily review of the need for renewal or removal of indwelling catheter and identification of symptomatic urinary tract infection (SUTI) with appropriate documentation in the system. Nursing staff were mainly trained on compliance to CAUTI interventions during admission and follow up the CAUTI interventions Daily Maintenance Form (Appendix A). During physician round they are reminded to document removal or renewal of the indwelling catheter. Infection Control Team were monitoring the hand hygiene, maximum barrier precautions and is responsible for daily data collection of CAUTI and catheter days. The Logistic Department was advised to keep constant supplies of Silicone Foleys Catheter of appropriate sizes and CAUTI tool kit, used for the aseptic insertion of urinary catheter. The ICU Nurse Manager is empowered to strictly monitor the daily renewal or removal of Foley catheter and its documentation by physicians, catheter maintenance, completion of CAUTI. Intervention Form by the nursing staff and to coordinate with Infection Control Practitioner Team on data collection, Surveillance Report of the unit on monthly and quarterly basis and send the feedback to all the participants in the project, thus identify the areas for improvement.
Data collection
The study population include all patients admitted to Adult Intensive Care Unit from January 1, 2008 to December 31, 2016. The study is designed to compare the retrospective data collected from January 1, 2008 to December 31, 2010 with prospective data collected from January 1, 2011 to December 31, 2016.
The infection control practitioner is responsible for the data collection on daily basis. Patients with catheter associated UTI that occurred less than 48 hours after admission were excluded.
The CAUTI was defined as per CDC/NHSN criteria as any infection that occurred while the patient had urinary catheter in place within 2 days of catheterization associated with fever, >38°C and positive urinary culture of more >10-5 Colony Forming Unit (CFU).10 The rate of CAUTI was calculated as number of patients with CAUTI divided by the number of indwelling urinary catheter days multiplied by 1000. The catheter utilization days were projected as total number of catheter days divided by total number of patient days multiplied by 100.
The data was collected on daily basis to identify the number of CAUTI patients, total number of patients with urinary catheter, catheter days, and compliance to the CAUTI interventions. Monthly and quarterly performance measures regarding process and compliance were prepared and submitted to the Quality and Patient Safety Department and feedback is conveyed to all the participants for possible improvement in this area of deficiency and the need for completing training program for the participants as per FOCUS-PDCA (find-organize-clarify-understand-select-plan-do-check-act) was organized.
Results
The average rate of CAUTI in Adult ICU was 2.3/1000 days during the year 2008 to 2010. After the implementation of these interventions and preventive measures, the most deficient intervention components was the initial screening of urinary catheter on ICU admission as many patients admitted were critical and physicians were engaged in stabilizing the patient. Since the time and indication for insertion of indwelling catheter for most of the patients in the wards, operating theatres, emergency department were not properly documented; the routine removal was not recommended as per the guidelines was one of the major resistance from the physician. The other deficiencies noted were maintenance of closed system by the nursing staff and occasional supply deficit of Silicone catheters from logistics.
The compliance rate gradually increased with persistent efforts from the team leaders toward the compliance of the CAUTI standard preventive measures along with prioritizing the needs of the patient safety, educational sessions conducted periodically, testing competency of the nursing staff for maintenance of measures, provision of adequate supplies from logistics, continued daily reminders during rounds by the Nurse Manager regarding renewal or removal of the catheter.
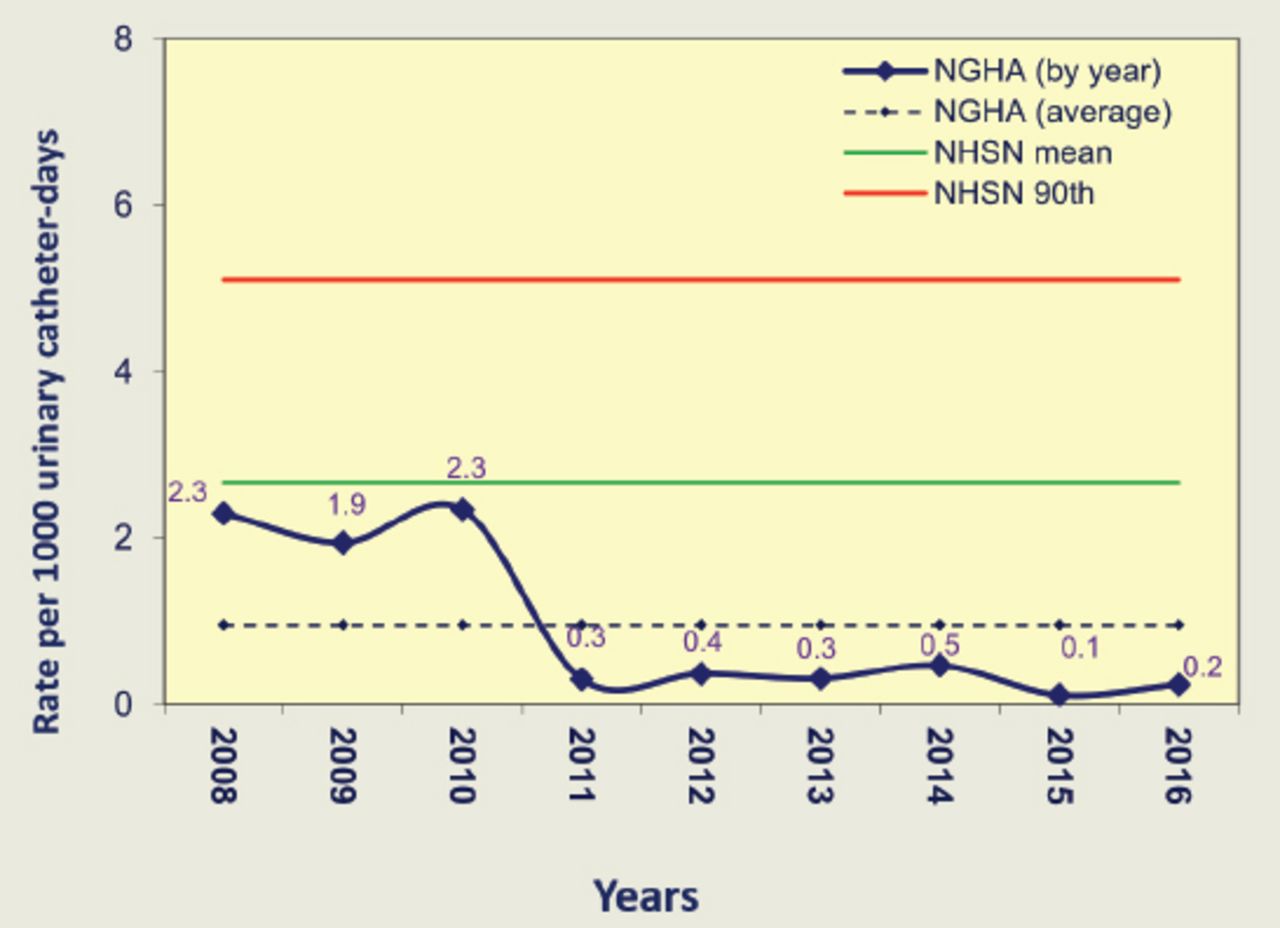
By the end of the first quarter, CAUTI preventive measures compliance reached to 56% with CAUTI rate dropped to 1.9 per 1000 catheter days. By second quarter compliance reached to 80% with CAUTI rate of 0.9/1000 indwelling catheters and by the end of 2011, CAUTI rate was 0.3/1000 indwelling catheters with 98% compliance to CAUTI preventive measures which was a remarkable achievement (Figure 1).
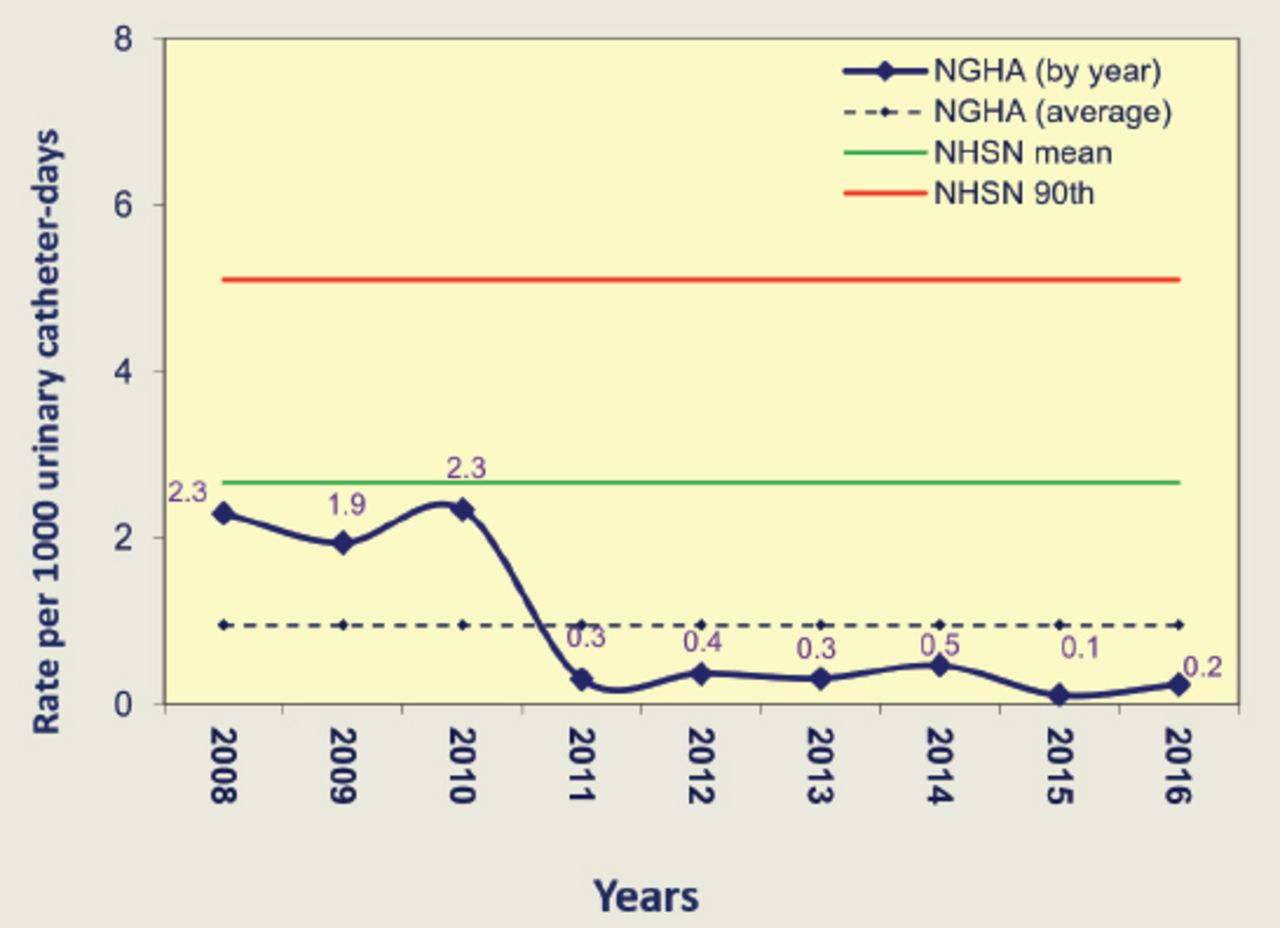
Rate of urinary tract infections per 1000 urinary catheter-days at adult (general) intensive care unit of King Abdul-Aziz Medical City, Jeddah, Saudi Arabia (2008-2016). NGHA - National Guard Health Affairs, NHSN - National Health Care Safety Network
We continued with the objective of sustained results with target compliance of 100% to CAUTI preventive interventions and subsequent years monitored the mean CAUTI rate of 0.3 to 0.5 per1000 indwelling catheter days. For the last two years 2015 and 2016 the CAUTI rate was 0.1-0.2 per 1000 indwelling catheter days. It gave us an immense confidence and satisfaction with our efforts towards the compliance of CAUTI preventive measures.
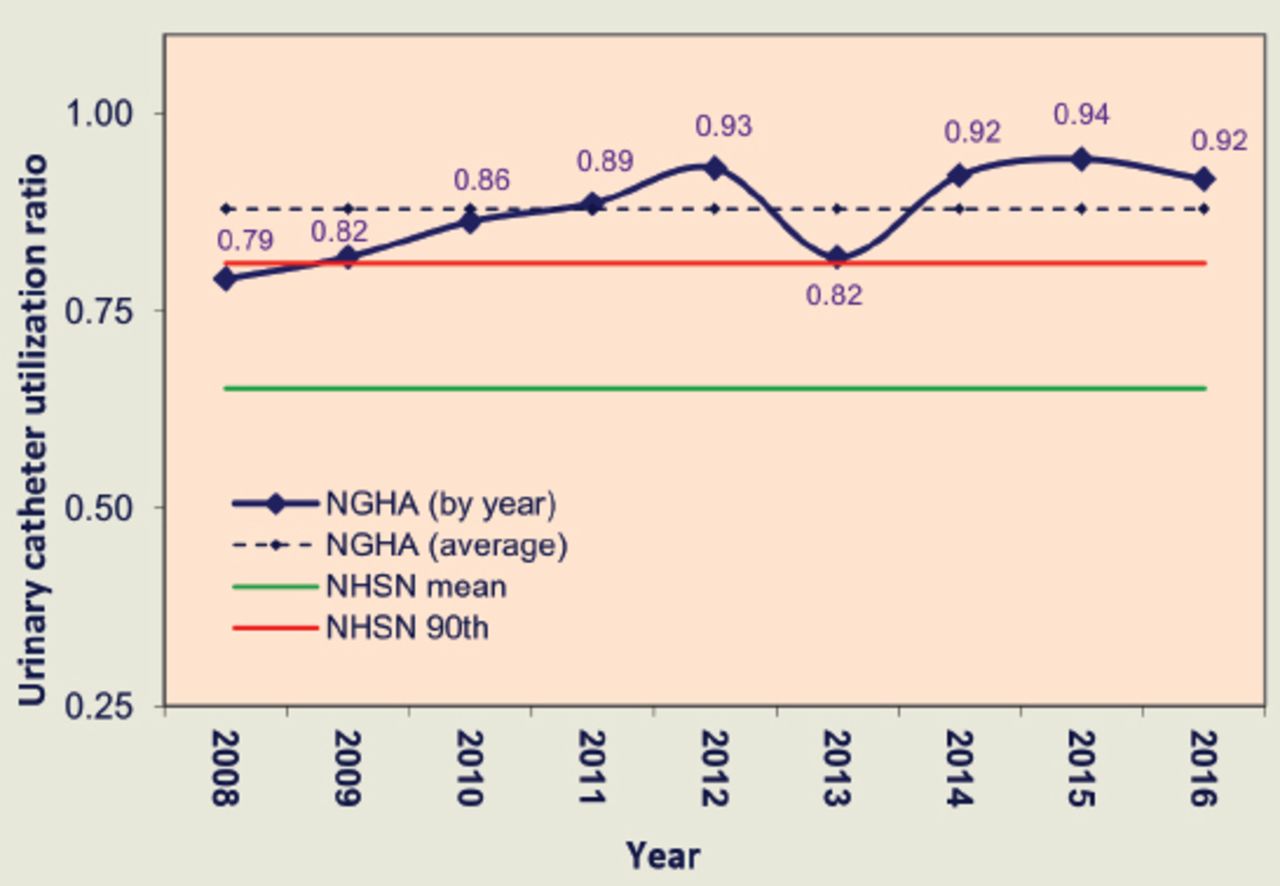
Despite the overall rise in urinary catheterization over these years, we observed reduction in UTI per 1000 urinary catheter days with significant reduction noted from 2.3 in 2010 to 0.3 in 2011 and was sustained through 2016 (Figure 2 & Table 1).
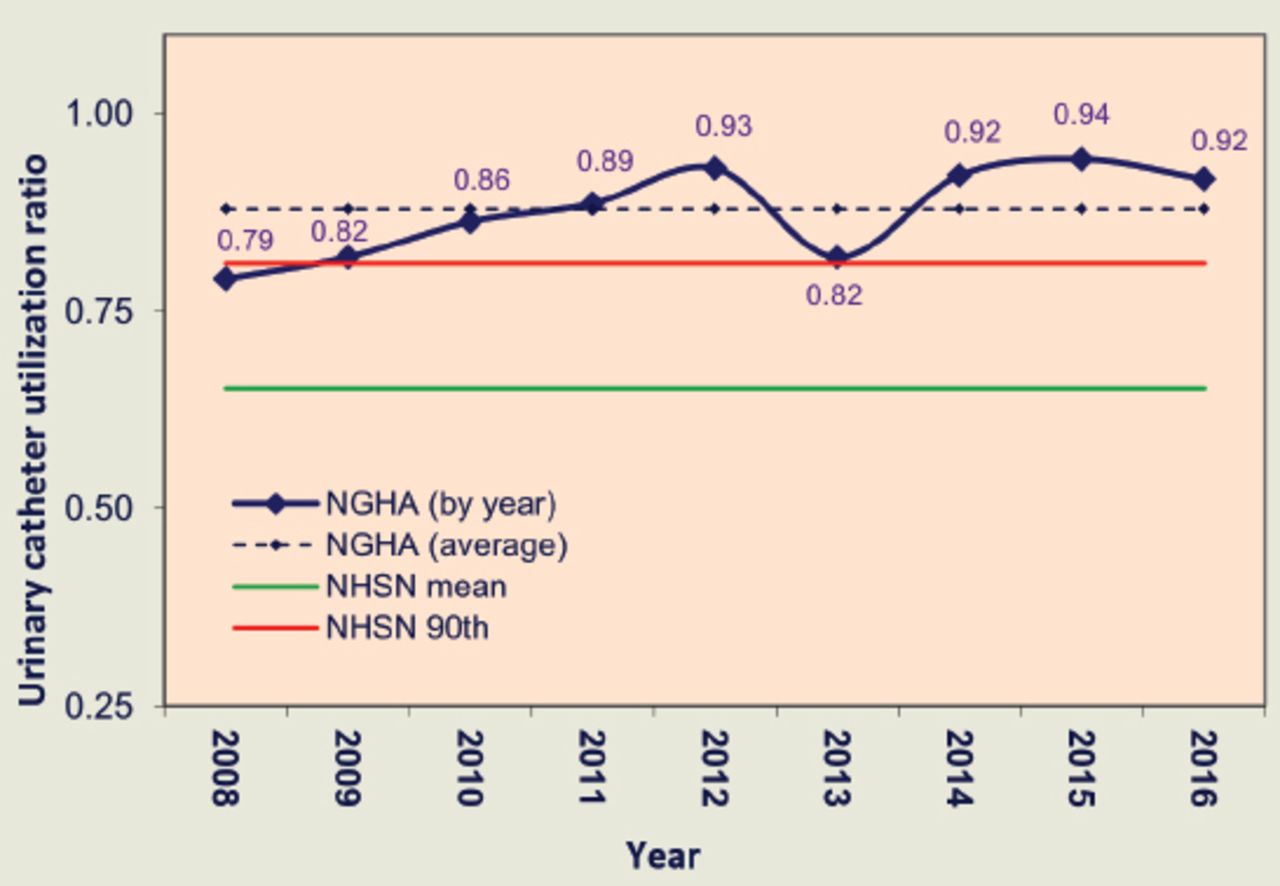
Urinary catheter utilization ratios at adult (general) intensive care unit of King Abdul-Aziz Medical City, Jeddah, Saudi Arabia (2008-2016). NGHA - National Guard Health Affairs, NHSN - National Health Care Safety Network.
Rate of urinary tract infection (UTI) and urinary catheter utilization ratios at adult (general) intensive care units of King Abdul-Aziz Medical City, Jeddah, Saudi Arabia (2008-2016).
Discussion
Urinary catheter insertion is a necessary and important procedure for patient care and management in ICU. In contrast, CAUTI is a serious healthcare associated infection with thoughtful adverse events. Unlike CLABSI, CAUTI has no agreed international standardized preventive Bundles until 2011, the year of our interventions launched. We report in this study our experience when using the best available clinical evidence of preventive measures on the rate of CAUTI in adult ICU and the favorable outcome.
A recent surveillance published from 6 hospitals from 3 Arabian Gulf countries (Saudi Arabia, Oman, and Bahrain) shows that the overall CAUTI rate was 3.2 per 1,000 catheter days. This rate was thought to be 35% higher than the National Healthcare Safety Network (NHSN) hospitals, but 37% lower than the International Nosocomial Infection Control Consortium (INICC) hospitals.10
In our study, the mean CAUTI rate was 2.3 per 1,000 device days in 2008. After applying our systematic preventive measures, we managed to reduce the rate to 0.3 per 1,000 device days during 2011 and rate was sustained to 0.1 & 0.2 in 2015 & 2016 respectively. This rate is lower compared to CAUTI rate reported from the ICUs that reports to NHSN which ranges from 1.2 to 4.5 per 1,000 catheter days in 2011.11
Gaid et al12 reported CAUTI rate of 2.3 to 4.4 in a multicentre study in 12 medical and surgical ICUs in Ministry of Health hospitals in Saudi Arabia using Device Assisted Healthcare Infection, comparing VAP, CLABSI and CAUTI; however, the details of the Methodology of CAUTI preventive measures in this study were lacking. In our study, we started with almost similar CAUTI rate, and based on our locally adopted CAUTI preventive interventions, strict compliance, and periodic monitoring of the surveillance reports and corrections with FOCUS-PDCA program we achieved and sustained the target reduction of CAUTI rate. In a study published by Press et al,13 reported a significant drop in CAUTI rate after the changes of definition of CAUTI by NHSN in 2009 to include only SUTI, excluding asymptomatic urinary tract infection (ASUTI), which needed further validation by many other studies. Another interesting and important finding in our study was the decrease of CAUTI rate despite overall rise in the urinary catheterization ratio over these years (Table 1), which can be explained by the strict compliance of CAUTI interventions and vigilant infection control preventive measures.
Our study has few limitations by the fact that it is from a single centre and from one Adult ICU patient populations with standard protocol management. The study period ranged from 2008 to 2016 at the time wherein changes in the definition of CAUTI by NHSN came in vogue, which mandate further validation of the process of identifying ASUTI and SUTI. Furthermore, the results of this study may be partially cofounded by the change in definition of CAUTI in January, 2009 by the NHSN, the CDC’s patient’s safety surveillance system. However, the strict implementation of nursing care interventions remain important measurements in reducing the rate of CAUTI.
This study highlights the importance of CAUTI care bundle in the future monitoring and implementation of Strategies to Prevent Catheter-Associated Urinary Tract Infections. We also recommend to extend the same to other units, such as CCU and wards and to call upon international campaigns to establish standardized CAUTI care bundle and hopefully to achieve the target of zero CAUTI rate.
In conclusion, we found that monthly rates of CAUTI significantly declined after the enforcement of the established strategies to prevent CAUTI in adult ICUs. Encouragement from the leadership and continuous support from the administration led to the success of this project with admirable outcome. This study also highlighted the importance and the need for international standardized CAUTI care bundle.
Acknowledgment
We would like to acknowledge Ang S. Gor, Ohoud Al-Orabi, from the Intensive Care Department, King Abdulaziz Medical City, National Guard Health Affairs, Jeddah, Kingdom of Saudi Arabia for data collection and support.
Appendix 1 - Catheter-associated urinary tract infections interventions daily maintenance form.
Footnotes
Disclosure
Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 9, 2017.
- Accepted December 9, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.