
Abstract
Summary
Prevalent vertebral fractures are associated with increased fracture risk, but the magnitude of this effect across a range of BMD T-scores has not been quantified. In this analysis, for any given BMD T-score, incident fracture risk varied up to twelve fold when information regarding prevalent radiographic vertebral fracture status was considered.
Background
Clinical fracture risk evaluation of older women usually includes assessment of bone mineral density (BMD) but often not vertebral fracture status. In this analysis, we quantified the impact of vertebral fracture burden on two year fracture risk across a range of BMD T-scores.
Methods
Data were from 2,651 postmenopausal women who were assigned to the placebo groups of the Fracture Prevention Trial (median observation 21 months) and the Multiple Outcomes of Raloxifene Evaluation Trial (MORE; observation 2 years). Using the Genant visual semiquantitative criteria, we defined prevalent vertebral fracture status as: a) presence or absence of fracture; b) fracture number; c) maximum semi-quantitative (SQ) score (normal=0, mild fracture=1, moderate fracture=2, severe fracture=3); and d) spinal deformity index (SDI) score (sum of SQ scores of T4 to L4 vertebrae). Incident fractures over two years were identified via lateral spine radiographs and outside the spine by questioning of patients and review of radiographs or radiographic reports.
Results
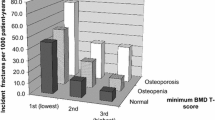
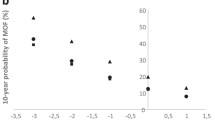
Femoral neck BMD T-score provided significant information regarding fracture risk. Across the range of T-scores, vertebral fracture status provided additional prognostic information. The risk increased with increasing number and severity of prevalent vertebral fractures and SDI, a summary measure of spine fracture burden. Across a range of BMD values, prevalent spine fracture burden as assessed by SDI increased the risk of incident vertebral fractures by up to 12-fold, nonvertebral fractures by about twofold, and any fractures by up to sevenfold.
Conclusions
These findings indicate that at any given BMD T-score, the risk of incident vertebral, non-vertebral, and any fracture depended heavily on prevalent radiographic vertebral fracture status. Assessment of vertebral fracture status, in addition to BMD, provides practical and relevant clinical information to aid in predicting fracture risk in postmenopausal women.



Similar content being viewed by others

References
Cummings SR, Melton LJI (2002) Epidemiology and outcomes of osteoporotic fractures. Lancet 359(9319):1761–1767
Ettinger B, Black DM, Mitlak BH et al (1999) Reduction of vertebral fracture risk in postmenopausal women with osteoporosis treated with raloxifene: results from a 3-year randomized clinical trial. Multiple Outcomes of Raloxifene Evaluation (MORE) Investigators. JAMA 282(7):637–645
Black DM, Cummings SR, Karpf DB et al (1996) Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture Intervention Trial Research Group. Lancet 348(9041):1535–1541
Cummings SR, Black DM, Thompson DE et al (1998) Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures: results from the Fracture Intervention Trial. JAMA 280(24):2077–2082
Black DM, Arden NK, Palermo L, Pearson J, Cummings SR (1999) Prevalent vertebral deformities predict hip fractures and new vertebral deformities but not wrist fractures. Study of Osteoporotic Fractures Research Group. J Bone Miner Res 14(5):821–828
Lindsay R, Silverman SL, Cooper C et al (2001) Risk of new vertebral fracture in the year following a fracture. JAMA 285(3):320–323
Ross PD, Davis JW, Epstein RS, Wasnich RD (1999) Pre-existing fractures and bone mass predict vertebral fracture incidence in women. Ann Intern Med 114(11):919–923
Gallagher JC, Genant HK, Crans GG, Vargas SJ, Krege JH (2005) Teriparatide reduces the fracture risk associated with increasing number and severity of osteoporotic fractures. J Clin Endocrinol Metab 90:1583–1587
Delmas PD, Genant HK, Crans GG et al (2003) Severity of prevalent vertebral fractures and the risk of subsequent vertebral and nonvertebral fractures: results from the MORE trial. Bone 33(4):522–532
Genant HK, Li J, Wu CY, Shepherd JA (2000) Vertebral fractures in osteoporosis: a new method for clinical assessment. J Clin Densitom 3(3):281–290
Cooper C, Atkinson EJ, O’Fallon WM, Melton LJ III (1992) Incidence of clinically diagnosed vertebral fractures: a population-based study in Rochester, Minnesota, 1985–1989. J Bone Miner Res 7(2):221–227
Neer RM, Arnaud CD, Zanchetta JR et al (2001) Effect of parathyroid hormone (1–34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med 344(19):1434–1441
Genant HK, Wu CY, van Kuijk C, Nevitt MC (1993) Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res 8(9):1137–1148
Genant HK, Jergas M, Palermo L et al (1996) Comparison of semiquantitative visual and quantitative morphometric assessment of prevalent and incident vertebral fractures in osteoporosis The Study of Osteoporotic Fractures Research Group. J Bone Miner Res 11(7):984–996
Grigoryan M, Guermazi A, Roemer FW, Delmas PD, Genant HK (2003) Recognizing and reporting osteoporotic vertebral fractures. Eur Spine J 12(suppl 2):S104–S112, Sep 11
Harris ST, Watts NB, Genant HK et al (1999) Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: a randomized controlled trial. Vertebral Efficacy With Risedronate Therapy (VERT) Study Group. JAMA 282(14):1344–1352
Crans GG, Genant HK, Krege JH (2005) Prognostic utility of a semiquantitative spinal deformity index. Bone 37(2):175–179
Genant HK, Siris E, Crans GG, Desaiah D, Krege JH (2005) Reduction in vertebral fracture risk in teriparatide-treated postmenopausal women as assessed by spinal deformity index. Bone 37(2):170–174
Lu Y, Ye K, Mathur AK, Hui S, Fuerst TP, Genant HK (1997) Comparative calibration without a gold standard. Stat Med 16(16):1889–1905
NIH Consensus Development Panel (2001) Osteoporosis prevention, diagnosis, and therapy. JAMA 285:785–795
Genant HK, Delmas PD, Chen P, Yiang Y, Eriksen EF, Dalsky GP, Marcus R, San Martin J. Severity of vertebral fracture reflects deterioration of bone microarchitecture. Osteoporosis International (in press)
Klotzbuecher CM, Ross PD, Landsman PB, Abbott III TA, Berger M (2000) Patients with prior fractures have an increased risk of future fractures: a summary of the literature and statistical synthesis. J Bone Miner Res 15:721–739
Guermazi A, Mohr A, Grigorian M, Taouli B, Genant HK (2002) Identification of vertebral fractures in osteoporosis. Semin Musculoskelet Radiol 6(3):241–252
Faulkner KG (2001) Clinical use of bone densitometry. In: Marcus R, Feldman D, Kelsey J (eds) Osteoporosis. Academic Press, San Diego, CA, USA, pp 433–458
Rea JA, Li J, Blake GM, Steiger P, Genant HK, Fogelman I (2000) Visual assessment of vertebral deformity by X-ray absorptiometry: a highly predictive method to exclude vertebral deformity. Osteoporos Int 11(8):660–668
Binkley N, Krueger D, Gangnon R, Genant HK, Drezner MK (2005) Lateral vertebral assessment: a valuable technique to detect clinically significant vertebral fractures. Osteoporos Int 16(12):1513–1518
Vokes TJ, Dixon LB, Favus MJ (2003) Clinical utility of dual-energy vertebral assessment (DVA). Osteoporos Int 14(11):871–878
Ferrar L, Jiang G, Barrington NA, Eastell R (2000) Identification of vertebral deformities in women: comparison of radiological assessment and quantitative morphometry using morphometric radiography and morphometric X-ray absorptiometry. J Bone Miner Res 15(3):575–585
Wu C, Genant H, von Ingersleben G et al (2004) Validation of lateral DXA imaging for assessment of vertebral fractures. J Bone Miner Res 19(suppl 1):S295
Acknowledgements
The authors thank the investigators and patients from both of the trials. Data were analyzed at Lilly Research Laboratories, Eli Lilly and Company. This study was supported by Eli Lilly and Company. All authors had access to all of the relevant data for this analysis.
Conflicts of interest statement
Dr. Siris serves as a consultant and receives honoraria from Eli Lilly and Company, Merck, Novartis, Procter & Gamble, Amgen, Pfizer and Glaxo-Smith Kline.
Dr. Genant serves as a consultant and receives an honorarium from Eli Lilly and Company, Novartis, Servier, Roche, GSK, BMS and Wyeth.
Dr. Laster serves as a consultant and receives honoraria or financial support from Eli Lilly and Company, Procter & Gamble, Merck, Roche/GSK, Abbott, and Genentech.
Drs. Chen, Misurski and Krege are employees of Eli Lilly and Company.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was supported by Eli Lilly and Company.
Rights and permissions
About this article
Cite this article
Siris, E.S., Genant, H.K., Laster, A.J. et al. Enhanced prediction of fracture risk combining vertebral fracture status and BMD . Osteoporos Int 18, 761–770 (2007). https://doi.org/10.1007/s00198-006-0306-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-006-0306-8