
Abstract
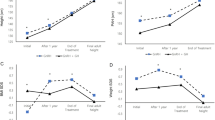
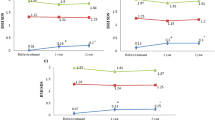
To evaluate the effect of central precocious puberty (CPP) and its treatment with gonadotropin-releasing hormone (GnRH) analogues on final height and peak bone mass (PBM), we measured lumbar bone mineral density (BMD) in 23 girls at final height. Patients were distributed in two groups. Group 1: 14 patients with progressive CPP were treated with GnRH analogues; seven patients received buserelin (1600 μg/daily), subsequently switched to depot triptorelin (60 μg/kg/26–28 days); seven patients were treated with depot triptorelin (60 μg/kg/26–28 days); mean age of treatment was 6.2 years (range 2.7–7.8 years); the treatment was discontinued at the mean age of 10.1 years (range 8.7–11.3 years); final height was reached at the mean age 13.4 years (range 12.0–14.9 years). Group 2: 9 patients (mean age 6.5 years, range 4.8–7.7 years) with a slowly progressing variant of CPP were followed without treatment; final height was reached at the mean age 13.6 years (range 12.5–14.8 years). Lumbar BMD (L2–L4 by dual energy X-ray absorptiometry) was measured in all patients at final height. In group 1, final height (158.9 ± 5.4 cm) was significantly greater than the pre-treatment predicted height (153.5 ± 7.2 cm, P < 0.001), but significantly lower than mid-parental height (163.2 ± 6.2 cm, P < 0.005). Subdividing the girls of group 1 according to the bone age at discontinuation of therapy (i.e. ≤11.5 years, n = 5, or ≥12.0 years, n = 9), the former patients had a final height significantly higher than the latter (163.7 ± 3.9 cm vs 156.5 ± 4.6 cm, P < 0.02). In group 2, final height (161.8 ± 4.6 cm) was similar to the pre-treatment predicted height (163.1 ± 6.2 cm, P = NS) and was not significantly different from mid-parental height (161.0 ± 5.9 cm). BMD values (group 1: 1.11 ± 0.14 g/cm2, group 2: 1.22 ± 0.08 g/cm2) were not significantly different from those of a control group (1.18 ± 0.10 g/cm2; n = 20, age 16.3–20.5 years) and the patients’ mothers (group 1: 1.16 ± 0.07 g/cm2, n = 11, age 32.9–45.1 years; group 2: 1.20 ± 0.08 g/cm2, n = 7, age 33.5–46.5 years). In group 1, the girls who stopped therapy at a bone age ≤11.5 years had significantly higher BMD (1.22 ± 0.10 g/cm2) compared to those who discontinued therapy at a bone age ≥12.0 years (1.04 ± 0.12 g/ cm2, P < 0.05).
Conclusion
In girls with progressive CPP, long-term treatment with GnRH analogues improves final height. A subset of patients with CPP does not require treatment because good statural outcome (slowly progressing variant). In CPP, the abnormal onset of puberty and the long-term GnRH analogue treatment do not impair the achievement of PBM. In GnRH treated patients, the discontinuation of therapy at an appropriate bone age for pubertal onset may improve both final height and PBM.
Similar content being viewed by others

Abbreviations
- BMD:
-
bone mineral density
- CPP:
-
central precocious puberty
- GnRH:
-
gonadotropin releasing hormone
- PBM:
-
peak bone mass
References
Antoniazzi F, Bertoldo F, Zamboni G, Valentini R, Sipresi S, Cavallo L, Adami S, Tatò L (1995) Bone mineral metabolism in girls with central precocious puberty during gonadotropin-releasing hormone agonist treatment. Eur J Endocrinol 133:412–417
Armamento-Villareal R, Villareal DT, Avioli LV, Civitelli R (1992) Estrogen status and heredity are major determinants of premenopausal bone mass. J Clin Invest 90:2464–2471
Bayley N, Pinneau SR (1952) Tables for predicting adult height from skeletal age: revised for use with the Greulich and Pyle standards. J Pediatr 40:432–441
Bertelloni S, Baroncelli GI, Battini R, Perri G, Saggese G (1995) Short-term effect of testosterone treatment on reduced bone density in boys with constitutional delay of puberty. J Bone Miner Res 10:1488–1495
Brauner R, Adan L, Malandry F, Zantleifer D (1994) Adult height in girls with idiopathic true precocious puberty. J Clin Endocrinol Metab 79:415–420
Dawood MY (1994) Hormonal therapies for endometriosis: implications for bone metabolism. Acta Obstet Gynecol [Suppl] 159:22–34
Dodin S, Lemay A, Maheux R, Dumont M, Turcot-Lemay (1991) Bone mass in endometriosis patients treated with GnRH agonist implant or danazol. Obstet Gynecol 77:410–415
Finkelstein JS, Klibanski A, Neer RM, Doppelt SH, Rosenthal DI, Segre GV, Crowley WFJr (1989) Increases in bone density during treatment of men with idiopathic hypogonadotropic hypogonadism. J Clin Endocrinol Metab 69:776–783
Finkelstein JS, Neer RM, Biller BMK, Crawford JD, Klibanski A (1992) Osteopenia in men with history of delayed puberty. N Engl J Med 326:600–604
Greulich WW, Pyle SI (1959) Radiographic atlas of skeletal development of the hand and wrist, 2nd end. Stanford University Press, Stanford
Kletter GB, Kelch RP (1994) Effects of gonadotropin-releasing hormone analog therapy on adult stature in precocious puberty. J Clin Endocrinol Metab 79:331–334
Krall EA, Dawson-Hughes B (1993) Heritable and life-style determinants of bone mineral density. J Bone Miner Res 8:1–9
Lee PA (1994) Laboratory monitoring of children with precocious puberty. Arch Pediatr Adolesc Med 148:369–376
Lonzer MD, Imrie R, Rogers D, Worley D, Licata A, Secic M (1996) Effects of heredity, age, weight, puberty, activity, and calcium intake on bone mineral density in children. Clin Pediatr 35:185–189
Matkovic V, Fontana D, Tominac C, Goel P, Chesnut CH III (1990) Factors that influence peak bone mass formation: a study of calcium balance and the inheritance of bone mass in adolescent females. Am J Clin Nutr 52:878–888
Matkovic V, Jelic T, Wardlaw GM, Ilich JZ, Goel PK, Wright JK, Andon MB, Smith KT, Heaney RP (1994) Timing of peak bone mass in Caucasian females and implication for the prevention of osteoporosis. Inference from a cross-sectional model. J Clin Invest 93:799–808
Matta WH, Shaw RW, Hesp R, Evans R (1988) Reversible trabecular bone density loss following induced hypo-oestrogenism with the GnRH analogue buserelin in premenopausal women. Clin Endocrinol (Oxf) 29:45–51
Mora S, Weber G, Guarneri MP, Nizzoli G, Pasolini D, Chiumello G (1992) Effect of estrogen replacement therapy of bone mineral content in girls with Turner syndrome. Obstet Gynecol 79:747–751
Neely EK, Bachrach LK, Hintz RL, Slemenda CW, Feezle L, Pescovitz OH (1995) Bone mineral density during treatment of central precocious puberty. J Pediatr 127:819–822
Oerter KE, Manasco PK, Barnes KM, Jones J, Hill S, Cutler GB Jr (1993) Effects of luteinizing hormone-releasing hormone agonists on final height in luteinizing hormone-releasing hormone-dependent precocious puberty. Acta Paediatr [Suppl] 388:62–68
Oostdijk W, Rikken B, Schreuder S, Otten B, Odink R, Rouwé C, Jansen M, Gerver WJ, Waelkens J, Drop S (1996) Final height in central precocious puberty after long term treatment with a slow release GnRH agonist. Arch Dis Child 75:292–297
Ott SM (1990) Attainment of peak bone mass. J Clin Endocrinol Metab 71:1082A-1082C
Saggese G, Bertelloni S, Baroncelli GI, Battini R, Franchi G (1993) Reduction of bone density: an affect of gonadotropin-releasing hormone analogue treatment in central precocious puberty. Eur J Pediatr 152:717–720
Scharia SH, Minne HW, Waibel-Treber S, Schaible A, Lempert UG, Wilster C, et al (1990) Bone mass reduction after estrogen deprivation by long-acting gonadotropin-releasing hormone agonist and its relation to pretreatment serum concentrations of 1,25 dihydroxyvitamin D3. J Clin Endocrinol Metab 70:1055–1061
Shankar R, Pescovitz OH (1995) Precocious puberty. Adv Endocrinol Metab 6:55–89
Takahashi Y, Minamitani K, Kobayashi Y, Minagawa M, Yasuda T, Niimi H (1996) Spinal and femoral bone mass accumulation during normal adolescence: comparison with female patients with sexual precocity and with hypogonadism. J Clin Endocrinol Metab 81:1248–1253
Tanner JM, Whitehouse RH, Takaishi M (1966) Standards from birth to maturity for height, weight, height velocity: British children. Arch Dis Child 41:613–635
Theintz G, Buchs B, Rizzoli R, Sloman D, Clavien H, Sizonenko PC, Bonjour J-PH (1992) Longitudinal monitoring of bone mass accumulation in healthy adolescents: Evidence for a marked reduction after 16 years of age at the levels of lumbar spine and femoral neck in female subjects. J Clin Endocrinol Metab 75:1060–1065
Waibel-Treber S, Minne HW, Scharia SH, Bremen T, Ziegler R, Leyendecker G (1989) Reversible bone loss in women treated with GnRH-agonists for endometriosis and uterine leiomyoma. Hum Reprod 4:384–388
Zachmann M (1992) Assessment of skeletal and sexual maturity: theoretical and practical aspects. Clin Pediatr Endocrinol [Suppl] 3:15–33
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Bertelloni, S., Baroncelli, G.I., Sorrentino, M.C. et al. Effect of central precocious puberty and gonadotropin-releasing hormone analogue treatment on peak bone mass and final height in females. Eur J Pediatr 157, 363–367 (1998). https://doi.org/10.1007/s004310050831
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s004310050831