Article Text

Abstract
All neurologists need to be able to recognise and treat cerebral venous thrombosis (CVT). It is difficult to diagnose, partly due to its relative rarity, its multiple and various clinical manifestations (different from ‘conventional’ stroke, and often mimicking other acute neurological conditions), and because it is often challenging to obtain and interpret optimal and timely brain imaging. Although CVT can result in death or permanent disability, it generally has a favourable prognosis if diagnosed and treated early. Neurologists involved in stroke care therefore also need to be aware of the treatments for CVT (with varying degrees of supporting evidence): the mainstay is prompt anticoagulation but patients who deteriorate despite treatment can be considered for endovascular procedures (endovascular thrombolysis or thrombectomy) or neurosurgery (decompressive craniotomy). This review summarises current knowledge on the risk factors, diagnosis, treatment and prognosis of CVT in adults, and highlights some areas for future research.
- Amyloid
- cerebrovascular disease
- MRI
- stroke
This article is made freely available for use in accordance with BMJ's website terms and conditions for the duration of the COVID-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
INTRODUCTION
Definition and pathophysiology
Cerebral venous thrombosis (CVT) is an important cause of stroke in young adults (mean age 33 years with a two-thirds female preponderance)1 caused by complete or partial occlusion of the cerebral major cerebral venous sinuses (cerebral venous sinus thrombosis) or the smaller feeding cortical veins (cortical vein thrombosis). CVT is frequently missed or diagnosed late because it can mimic other acute neurological conditions and can only be recognised with optimal and timely brain imaging.2 CVT was found in 9.3% of one consecutive autopsy series,3 suggesting that it might often be missed in life. CVT generally has a favourable prognosis if diagnosed and treated early.4 The mainstay of acute treatment is anticoagulation with parenteral heparin, but patients who deteriorate despite treatment can be considered for endovascular procedures (endovascular thrombolysis or thrombectomy) or neurosurgery (decompressive craniotomy).5 6
CVT accounts for 0.5–1.0% of unselected stroke admissions7 and is about three times as common in women than men,8 9 probably partly due to its association with pregnancy, the puerperium and the use of oestrogen-containing oral contraceptives.10
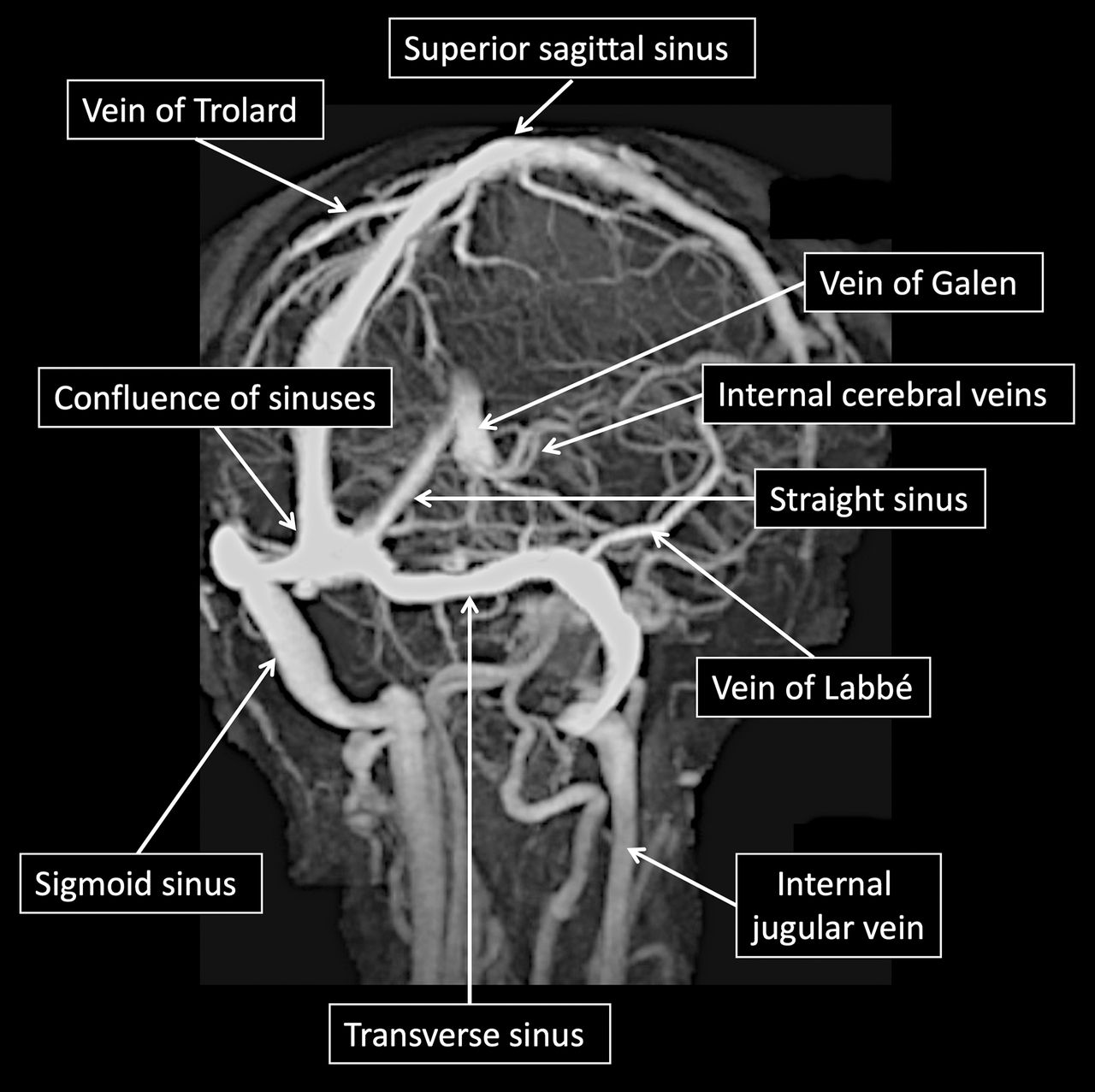
Blood from the brain drains through small cerebral veins into larger veins of the deep venous system (including the internal cerebral veins, basal veins (of Rosenthal) and vein of Galen), which then empty into dural sinuses (including the straight sinus, transverse sinuses and sagittal sinus); these in turn drain mainly into the internal jugular veins (figure 1). Changes in blood stasis, vessel wall abnormalities and the composition of the blood (Virchow’s triad) lead to an imbalance between prothrombotic and fibrinolytic processes, predisposing to progressive venous thrombosis. Obstruction of venous vessels induces increased venous pressure, reduced capillary perfusion and locally increased cerebral blood volume. Although initially compensated for by the dilatation of cerebral veins and the recruitment of collateral vessels, continued elevation of venous pressure can cause vasogenic oedema (due to blood–brain barrier disruption) and decreased cerebral perfusion pressure and cerebral blood flow with tissue infarction11; thus, both cytotoxic and vasogenic oedema can occur.12 The venous territories are less well defined than are arterial territories due to extensive anastomoses between cortical veins, which allow the development of alternative venous drainage pathways after an occlusion. CVT can also block cerebrospinal fluid absorption through the arachnoid villi, which then leads to raised intracranial pressure (with or without tissue injury), typically in association with superior sagittal sinus obstruction.
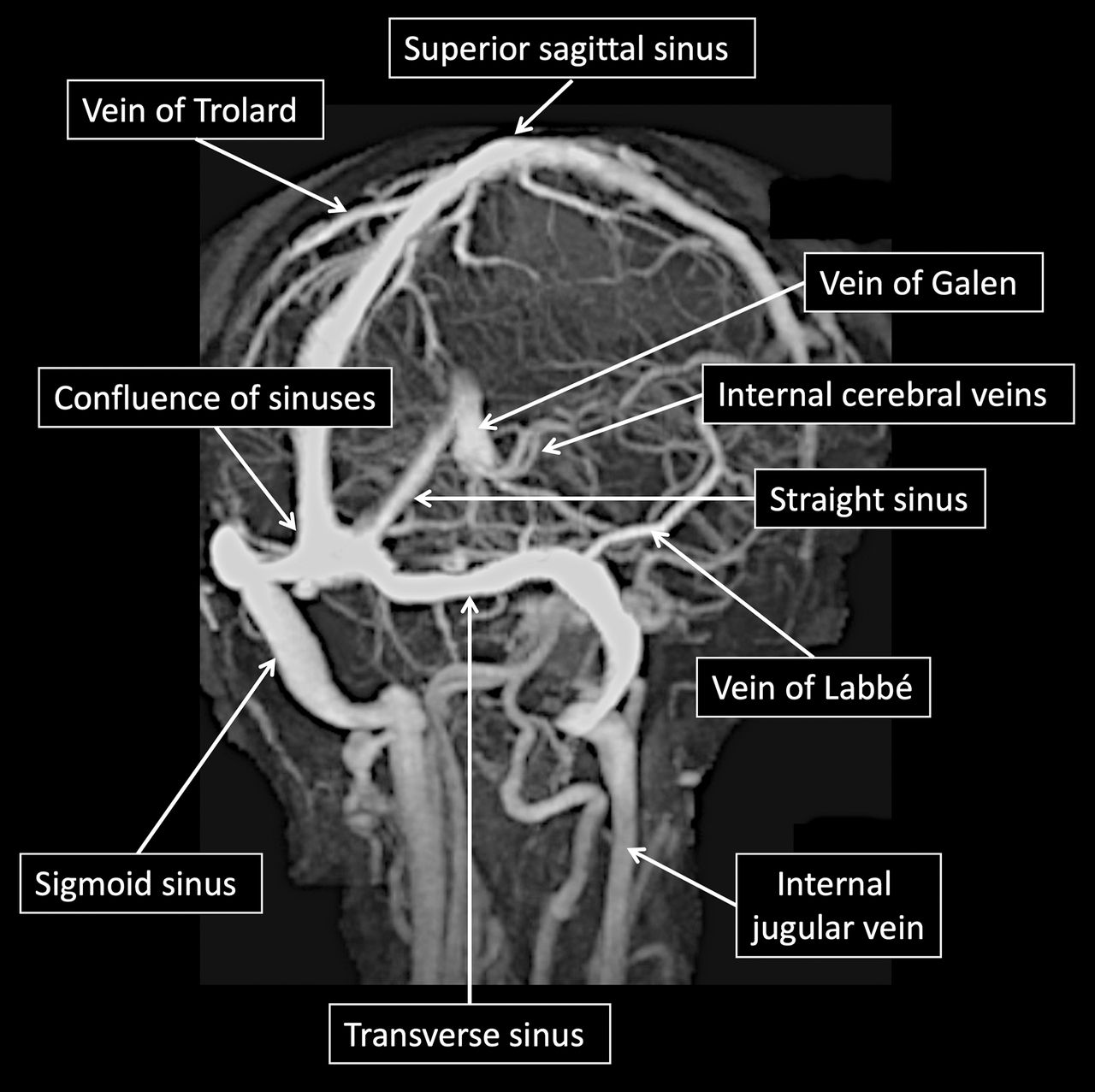
Time of-flight MR venogram of the normal major cerebral veins and venous sinuses. (Image courtesy of Assoc Prof Frank Gaillard, Radiopaedia.org, rID: 51 158).
These pathophysiological changes can cause the typical focal neurological symptoms and signs of CVT, which depend on the territory of the brain that has impaired venous drainage, the acuity of the occlusion (sudden or gradual), the degree of collateralisation and the degree of associated tissue injury (see the section on ‘Clinical presentation’ and table 1). The slow growth of the thrombus and collateralisation of venous vessels probably accounts for the often gradual onset of symptoms, frequently over days, weeks or even months.
Clinical manifestations of cerebral venous thrombosis according to occlusion site
This review aims to provide general neurologists, stroke physicians, general physicians, emergency physicians and neurosurgeons with advice on diagnosis and treatment of patients with CVT. Our management suggestions are in part based on guidelines from the American Heart Association and American Stroke Association11 and the more recent European Stroke Organization and European Academy of Neurology (ESO-EAN) guidelines.13 However, where data are limited, we have offered suggestions based on expert opinion or clinical experience.
SEARCH STRATEGY AND SELECTION CRITERIA
We searched PubMed, Medline and Cochrane Library, from 1995 to May 2020 using the search (((sinus*[TI] AND thrombosis[TI]) OR (thrombosis[TI] AND cerebral [TI] AND (venous[TI] OR vein*[TI] OR sinus*[TI])) OR (‘Sinus Thrombosis, Intracranial’[MESH]) OR (intracranial[TI] AND thrombosis[TI]))) and other relevant terms including ‘aetiology’, ‘pathogenesis’, ‘risk factors’, ‘diagnosis’, ‘therapy’, ‘treatment’, ‘therapeutics’, ‘management’, ‘anticoagulant’, ‘endovascular’, ‘decompressive craniectomy’, ‘prognosis’. We limited the search to human studies and those published in English. This search was supplemented by reviewing additional references from included studies.
RISK FACTORS
Important risk factors for CVT (most likely first) are oestrogen-containing oral contraceptives, prothrombotic (hypercoagulable) conditions (genetic or acquired thrombophilias), pregnancy and the puerperium, infections, malignancy,14 head injury (causing direct trauma to venous structures) and inflammatory diseases7 (table 2). The International Study on Cerebral Vein and Dural Sinus Thrombosis8 found that up to 85% of adult patients have at least one risk factor; the most common was use of oral contraceptives, followed by a prothrombotic condition (more often genetic than acquired) (table 2).
Risk factors for cerebral venous thrombosis (from Ferro et al8)
Heritable thrombophilias associated with CVT include factor V Leiden and the G20210A prothrombin gene mutation,15 as well as antithrombin, protein C and S deficiency.16 Homozygosity for the C655T MTHFR polymorphism has also been reported; this is present in approximately 10% of the normal population and is not considered a sufficient cause of CVT in isolation, although it may predispose to hyperhomocysteinaemia, which in turn can lead to thrombosis.16 In order to understand better the genetic factors involved in CVT, a large consortium genome-wide association study17 is ongoing.
The most common acquired prothrombotic states are pregnancy, the puerperium and oral contraceptives,18 which explain the threefold increase in risk of CVT among women of childbearing potential.10 Moreover, obesity seems to increase the risk of CVT, especially in women using oral contraceptives.19 Antiphospholipid antibody syndrome is also an important (and treatable) cause of CVT, which should be sought in all unexplained cases.20 In patients aged over 55 years, CVT is equally prevalent between the sexes21, and malignancy is a frequent cause (in 25% of patients).
Other less common causes of CVT include local infection (ears, sinuses, mouth, face or neck); head injury with trauma to the venous sinuses, iron deficiency anaemia, inflammatory diseases (systemic lupus erythematosus, Behçet’s disease, granulomatosis with polyangiitis, inflammatory bowel disease and sarcoidosis); and haematological disorders (myeloproliferative diseases associated with JAK2 V617F mutations, paroxysmal nocturnal haemoglobinuria and haemoglobinopathies).22
Many patients have multiple risk factors, so unless a very clear cause is found (eg, direct invasion of a sinus by a local ear infection), most patients need a thorough search for all risk factors (particularly thrombophilias).
CLINICAL PRESENTATION
The symptoms of CVT range from minor to life-threatening11 depending on the sinuses and veins involved, the extent of brain parenchymal injury, chronicity, and the effect on intracranial pressure (table 1). It is helpful to classify the manifestations of CVT into clinical syndromes, which depend on the predominant site of venous occlusion, though often these overlap.10 The superior sagittal sinus is most frequently affected (in 62%), causing a wide range of potential presentations with combinations of headache (from raised intracranial pressure), focal neurological deficits (eg, hemisensory loss, hemiparesis, hemianopia, from parenchymal injury) and seizures (figure 2). Transverse sinus thrombosis (in about 45%, see figure 3) typically causes temporoparietal haemorrhagic infarction (from occlusion of the vein of Labbé) with headache and, if left sided, aphasia, sometimes with seizures. Sigmoid sinus involvement is rare in isolation but can cause mastoid pain and, very rarely, lower cranial neuropathies. Thrombosis of the deep veins (internal cerebral veins, basal veins of Rosenthal, vein of Galen, straight sinus) is present in about 18% and often causes oedema of the thalami, which is challenging to diagnose because it typically causes mental status alteration, reduced awareness or coma, sometimes with gaze palsy (figure 4). Isolated intracranial hypertension (typically from sagittal sinus thrombosis, often long-standing) usually leads to headache, papilloedema and visual impairment. Finally, cavernous sinus thrombosis is much rarer but easy to recognise due to its characteristic presentation with eye pain, chemosis, proptosis and oculomotor palsy, usually associated with infection.7

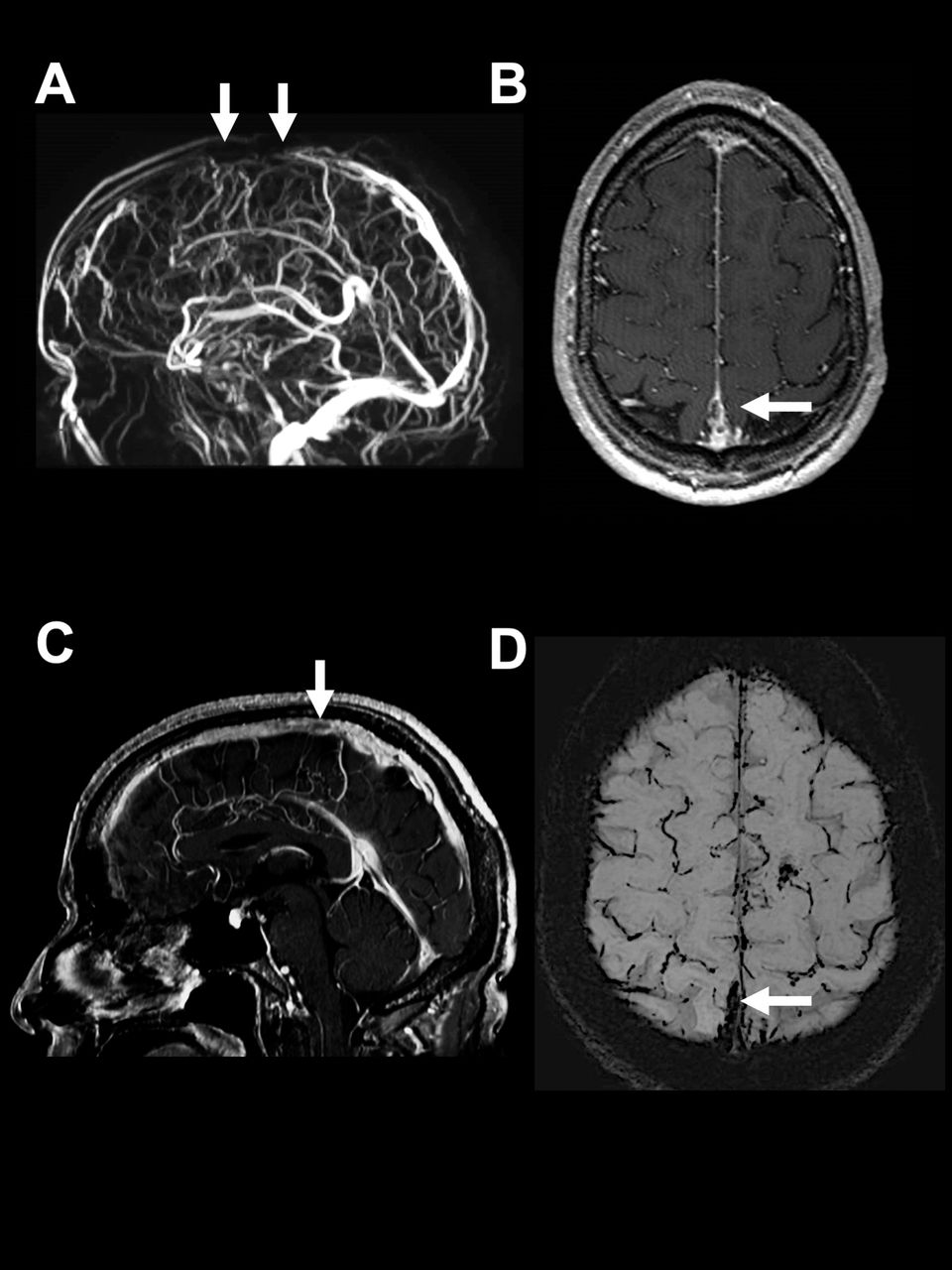
Sagittal sinus thrombosis. (A) MR venogram showing absent venous flow signal in the middle third of the superior sagittal sinus (white arrows); (B) axial gadolinium-enhanced T1-weighted MR scan showing an irregular filling defect of the superior sagittal sinus (white arrow); (C) sagittal gadolinium-enhanced T1-weighted MR scan also showing a focal filling defect indicating thrombus (white arrow); (D) axial susceptibility-weighted imaging showing low signal indicating blood products (thrombus) in the superior sagittal sinus (white arrow).

Transverse venous sinus thrombosis. (A) Area of haemorrhagic infarction of the right temporoparietal region not respecting arterial boundaries with swelling and oedema (white arrows); (B) CT venogram showing absent contrast filling of the right transverse sinus (white arrow); (C) severe haemorrhagic infarction with worsening mass effect that was treated with hemicraniectomy (white arrows).
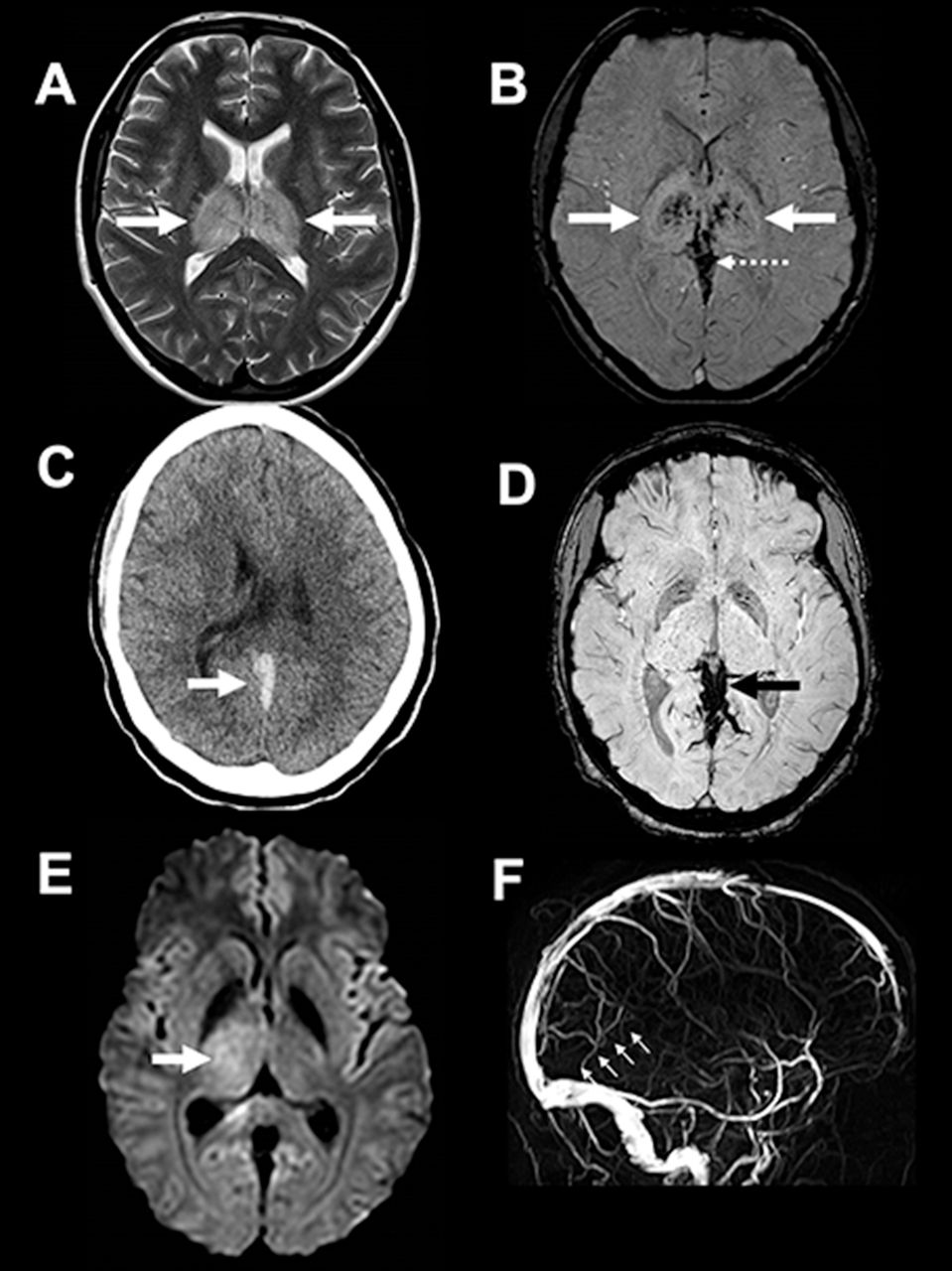
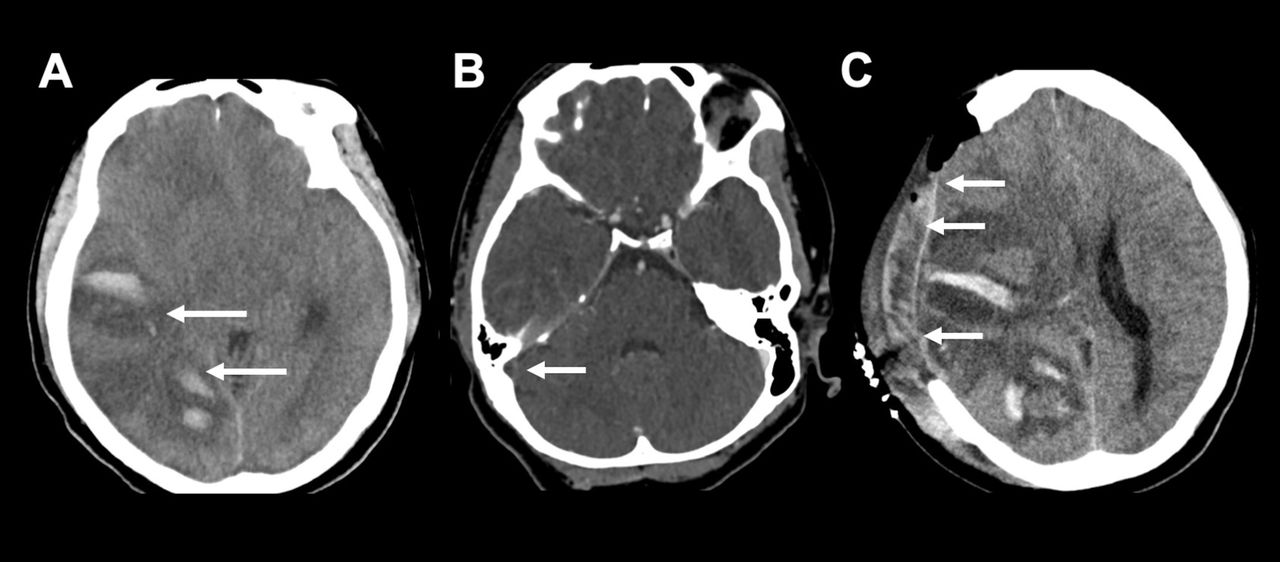
Deep cerebral venous thrombosis. (A) Axial T2-weighted image showing bilateral thalamic high signal (white arrows) in a 21-year-old woman (taking the oral contraceptive pill) who presented with headache, drowsiness and confusion; (B) SWI in the same patient showing petechial haeomorrhage within the areas of thalamic infarction (white arrows), and low signal in the deep cerebral and internal veins consistent with thrombosis (white dashed arrow); (C) unenhanced CT scan of head showing hyperdense acute thrombus in the straight sinus and vein of Galen (white arrow); (D) SWI showing low signal in the internal cerebral veins consistent with venous thrombosis (black arrow); (E) axial diffusion-weighted MR scan showing restricted diffusion in the right thalamus (indicating venous ischaemia; white arrow) in an 18-year-old woman who presented with headache and drowsiness, and who was taking the oral contraceptive pill; (F) MR venogram showing loss of flow signal in the deep venous system (straight sinus, vein of Galen, and internal and basal veins; approximate expected position shown by the dashed small white arrows). SWI, susceptibility-weighted imaging.
Headache is the most common symptom of CVT, reported in about 90% of cases; indeed, it is the only manifestation in about 25% of patients.11 Unfortunately, CVT-related headache does not have specific diagnostic features, though is usually progressive in onset (hours or days); much less often, thunderclap headache can be the first symptom, presumably related to subarachnoid bleeding.23 Headache from CVT can be localised or diffused, sometimes with migrainous headache or aura features.23–25 We suggest that neuroimaging should be performed in the presence of red flags for CVT, which include a headache that is new-onset and persistent; worse with the Valsalva manoeuvre; not improved with regular analgesia; or in a person with typical CVT risk factors or papilloedema (table 3).26
When to suspect CVT in a patient with headache
Stroke-like focal neurological symptoms occur in up to 40% of patients with CVT,8 18 though are often not as sudden in onset as arterial ischaemic stroke or intracranial haemorrhage; motor symptoms are most frequent, followed by visual impairment and aphasia (especially if the left transverse sinus and vein of Labbé are involved), whereas sensory symptoms are less common.18 In a large multicentre cohort, there was brain infarction in 36.4% of patients, haemorrhagic transformation in 17.3% and intraparenchymal haemorrhage in 3.8%.18 In a patient with a stroke syndrome, factors that point towards CVT rather than arterial ischaemic stroke include headache and seizures27(reported in up to 40% cases),8 and infarction on neuroimaging that does not fit a single arterial territory and usually has a prominent haemorrhagic component (figure 3). Reduced consciousness, ranging from drowsiness to coma, can result from raised intracranial pressure, deep venous infarction (figure 4) or both.28
Thrombosis of small cortical veins is usually associated with CVT, but can rarely occur in isolation. The typical symptoms of isolated cortical vein thrombosis are focal neurological deficits (usually anatomically limited due to the smaller territory of cerebral injury) and seizures; raised intracranial pressure is less common than in CVT.
The clinical presentation of CVT varies with age. Most affected children are aged younger than 6 months; in neonates, nonspecific symptoms of lethargy, bulging fontanel or seizures can occur.29 30 Compared with younger patients, those older than 65 years less commonly develop intracranial hypertension, while mental status and alertness disturbances are common; the prognosis of CVT (for dependency, death and recurrent thrombotic events) is worse in elderly patients.21
DIAGNOSIS
Patients with suspected CVT require urgent neuroimaging to confirm the diagnosis, using either CT or MR to visualise the thrombus directly, show impaired venous flow or both (table 4).13 No laboratory test can rule out CVT. The D-dimer level can be normal, especially in mild or chronic cases,31 32 but it has a high negative predictive value for excluding CVT in the specific situation of patients with isolated headache,31 and therefore has been suggested as a component of a preimaging probability score, along with a normal neurological examination and CT scan of head, to avoid unnecessary neuroimaging.33 Routine blood studies (erythrocyte sedimentation rate, blood count, chemistry panel, prothrombin time and activated partial thromboplastin time) should ideally be done before starting anticoagulation treatment (although where there is clinical urgency anticoagulation is started before receiving these results, relying on initial clinical evaluation for evidence of a bleeding diathesis or renal or liver disease).13
Neuroradiological features of CVT
Neuroimaging
Non-contrast CT scan of head is a useful first test (and the first brain imaging in suspected stroke or acute headache in many hospitals): in about one-third of patients, it shows specific signs including venous sinus or deep vein hyperdensity,34 (figure 4C) sometimes termed the dense triangle sign (high attenuation in the sagittal sinus or deep cerebral veins in a triangle shape)35 or the cord sign (high attenuation due to thrombus in the transverse sinus).36 CT can also detect ischaemia (typically not respecting arterial boundaries, often with some haemorrhagic transformation), parenchymal or subarachnoid haemorrhages, or signs of oedema (figure 3). However, plain CT is normal in up to 30% of patients and, even if abnormal, is not specific.7 37 Thus, all patients with suspected CVT require further imaging beyond a plain CT scan.
The ESO guidelines suggest MR venography or CT venography for confirming the diagnosis.13 We prefer CT venography as a ‘lumen-based’ rather than ‘flow-based’ method: compared to the gold standard of digital subtraction angiography (DSA), it has very good diagnostic accuracy (sensitivity of 95% and specificity of 91%).38 CT venography can show absent flow in thrombosed veins or sinuses and partial circumferential enhancement of thrombosed venous sinuses (eg, the empty delta sign39; figure 5). However, false positives can be due to normal sinus hypoplasia or arachnoid granulations.40 MR venography, performed with time-of-flight sequences, also allows assessment of the absence of flow in thrombosed sinuses (figure 2A), without the need for contrast medium41 but with a higher risk of false positives (eg, in the frequent case of a non-dominant (hypoplastic) transverse sinus).

The ‘empty delta’ sign. Axial contrast-enhanced CT scan, where the contrast outlines a filling defect of the sagittal sinus (due to thrombosis), creating the shape of the Greek letter delta (Δ; white arrows) (image courtesy of Dr Bruno Di Muzio, Radiopaedia.org, rID: 57 576).
MRI is the most sensitive technique for demonstrating the presence of the thrombus material, using sequences sensitive to the magnetic susceptibility effects of paramagnetic iron-containing blood components (T2*-weighted gradient echo or susceptibility-weighted imaging; SWI) (figure 2D and figure 4D); the appearance of the clot on different MRI sequences varies depending on its age42 so can also help to date likely CVT onset (table 4). MRI is also the best technique to assess parenchymal involvement fully (ischaemia, haemorrhages, oedema, swelling); furthermore, diffusion-weighted imaging-hyperintense thrombosed sinuses have been reported to have a reduced rate of recanalisation.43
Catheter intra-arterial DSA should be used to confirm the diagnosis only when CT venography or MR venography is inconclusive or there is a suspicion of a dural arteriovenous fistula.11 13 The relationship between dural arteriovenous fistulae and CVT is complex and not fully understood. A dural arteriovenous fistula can rarely complicate CVT, a phenomenon presumed due to the opening of arteriovenous pathways in the wall of the sinus during occlusion or recanalisation. It is important to detect the fistula early (requiring intra-arterial DSA) to allow treatment, for example, with embolisation. Conversely, CVT can occur during the development of an arteriovenous fistula. Whatever the relationship, clinicians need to be aware that these pathologies can co-exist and that they require specific treatments. Isolated cortical vein thrombosis is usually well seen on susceptibility-weighted sequences but can be challenging diagnose, and occasionally also requires intra-arterial DSA to confirm.
TREATMENT
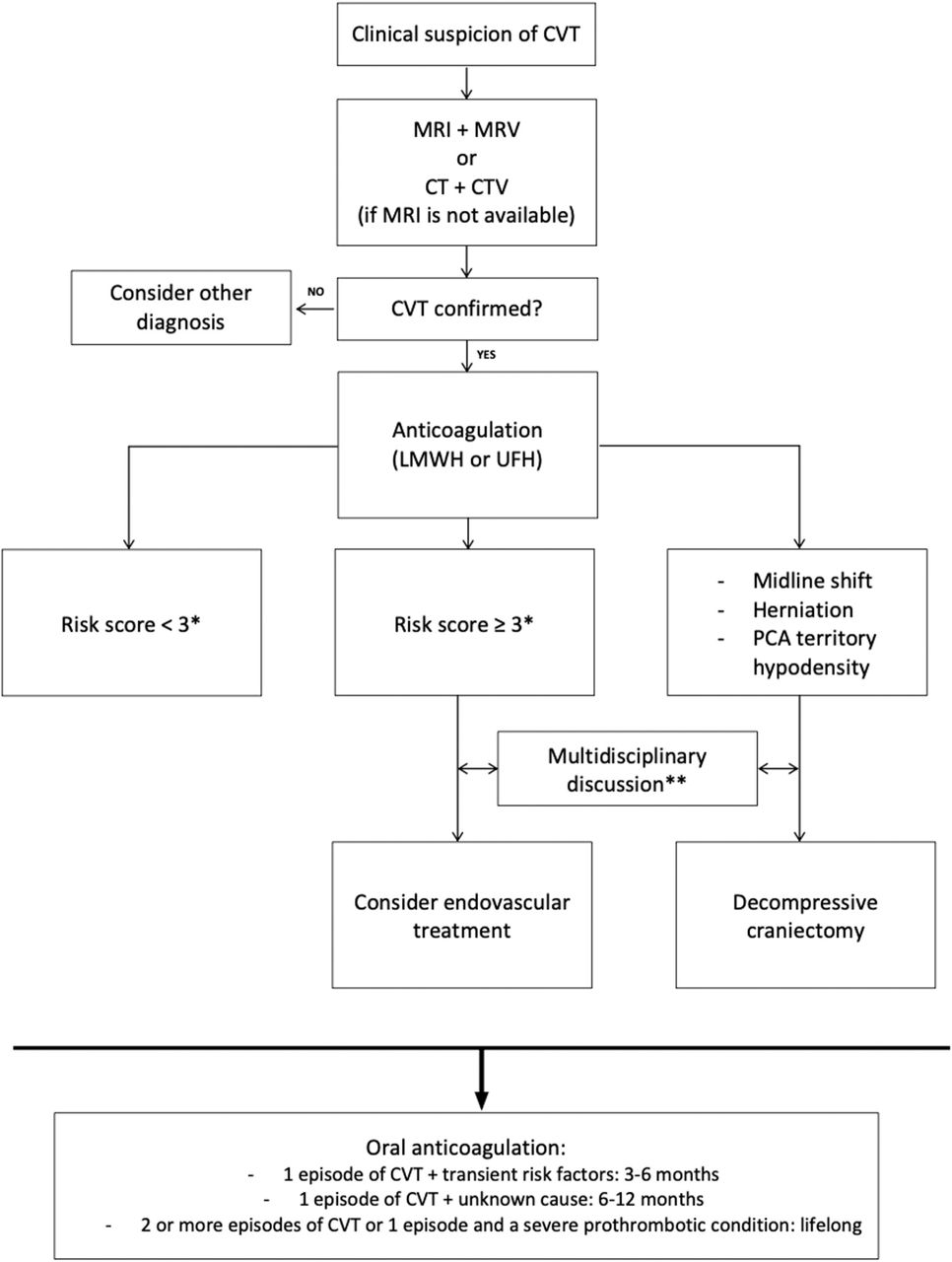
Treatment should be started as soon as the diagnosis of CVT is clearly confirmed, with rapid anticoagulant therapy, treatment of any underlying cause (eg, dehydration, sepsis, stopping any prothrombotic medications), control of seizures and management of intracranial hypertension if required. Figure 6 provides a suggested management decision flow chart.
Anticoagulation
The evidence supporting anticoagulation in CVT is widely accepted and guides clinical practice. However, it is - perhaps surprisingly - fairly weak, being based on data from four randomised controlled trials with methodological limitations. The first placebo-controlled trial of intravenous heparin for CVT (given on average rather late, at about 4 weeks), undertaken in Berlin, was stopped early after an interim analysis showed increased mortality in the placebo arm.44 Another trial (at multiple centres in The Netherlands and the UK) in 60 participants randomly allocated to nadroparin (low-molecular-weight heparin (LMWH)) or placebo (but excluding those requiring lumbar puncture for raised intracranial pressure) found a non-significant improvement in the proportion of participants achieving a good functional outcome for LMWH.45 A Cochrane review of these two trials (n=79)46 found that unfractionated heparin or LMWH treatment was associated with a non-significant reduction in death or dependency (relative risk 0.46, 95% CI 0.16 to 1.31). Only three patients developed a new intracranial haemorrhage, all allocated to placebo. Major extracranial bleeding occurred in one patient randomised to LMWH. Two other trials from India (n=97) used only non-contrast CT for diagnosis and were published only as abstracts (so could not be included in the meta-analysis), but also suggested benefit from heparin.
LMWH is the preferred anticoagulant treatment for CVT, also based on limited trial evidence. An open-label randomised controlled trial including 66 patients with CVT concluded that LMWH in full anticoagulant doses is more effective than unfractionated heparin47 with a lower risk of major bleeding or death. Although there are no large, high-quality randomised trials,48 LMWH is recommended in guidelines from the ESO13 and is our standard practice; we usually give this as split-dose (ie, two divided doses per 24 hours) to minimise the risk of haemorrhagic complications. The ESO guidelines advises that unfractionated heparin should be used in patients with renal insufficiency or in patients requiring very rapid reversal of anticoagulation (eg, imminent neurosurgical intervention).13 However, the summary of product characteristics for LMWH do not include severe renal impairment as a contraindication. We therefore use reduced dose LMWH in severe renal impairment, with specialist haematological advice about dosing and anti-Xa level monitoring. We very rarely use unfractionated heparin as it is very difficult to monitor and ensure therapeutic anticoagulation. Although their alarming radiological appearance can cause anxiety, haemorrhagic venous infarction, intracranial haemorrhage or isolated subarachnoid haemorrhage are not contraindications for anticoagulant treatment in CVT.49
Cortical vein thrombosis is also usually treated with anticogulation (and is our practice) though there are no randomised controlled trials. In a series of 116 patients, most (80%) were treated with anticoagulation, with good outcome (6% in-hospital mortality).50
Preventing further venous thrombotic events
Initial anticoagulation with LMWH (started as soon as the diagnosis is confirmed) is followed by longer-term anticoagulation to prevent further venous thrombotic events; the risk of recurrent CVT is about 2–7% per year, and the risk of other venous thrombosis is about 4–7% per year.8 Current guidelines recommend using oral vitamin-K antagonist (usually warfarin in the UK) at standard-intensity (target internationalised normalised ratio (INR) 2.5, range 2.0–3.0) for between 3 and 12 months.13 The optimal duration of anticoagulation in CVT is uncertain because of the lack of randomised trials or prospective studies, and, in practice, it is decided based on the underlying risk factors for recurrence and bleeding.11 51 However, the following suggested scheme (see figure 6) is supported by expert opinion and guidelines11: patients with one episode of CVT and transient risk factors (dehydration, drugs (eg, oral contraceptives), infections, trauma, surgical interventions) should receive anticoagulation for 3–6 months; patients with one episode of CVT of unknown cause should continue anticoagulation for 6–12 months; and those patients with two or more CVTs (or one episode and a severe prothrombotic condition with a high ongoing thrombotic risk) are usually recommended to have lifelong anticoagulation. These sometimes difficult decisions should involve discussion with haematology. A study comparing the efficacy and safety of short-term (3–6 months) versus long-term (12 months) anticoagulation after CVT (EXtending oral antiCOAgulation treatment after acute Cerebral Vein Thrombosis) is ongoing.52

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Suggested management algorithm for CVT. CVT, cerebral venous thrombosis; CTV, CT venography; LMWH, low-molecular-weight heparin; MRV, MR venography; PCA, posterior cerebral artery; UFH, unfractionated heparin.
The direct oral anticoagulants (DOACs) are an effective, safe and convenient alternative to vitamin-K antagonists and have changed the management of atrial fibrillation and venous thromboembolism. Moreover, DOACs do not require INR monitoring or dose adjustments, have fewer interactions with other medications or need for dietary restrictions, and a lower rate of intracranial bleeding compared with vitamin-K antagonists.53 However, current guidelines do not recommend DOACs in patients with CVT because of the limited quality of the available evidence. A recent exploratory randomised, open-label clinical trial randomly allocated 120 participants with CVT to dabigatran versus warfarin for 6 months (Re-SPECT CVT);54 there were no recurrent venous thromboembolic events in either treatment group, while major bleeding occurred in one patient allocated to dabigatran and two treated with warfarin. The authors concluded that both dose-adjusted warfarin and dabigatran are safe and effective in secondary prevention of any venous thromboembolic events after CVT. Further randomised controlled studies of DOACS for CVT are underway (eg, Study of Rivaroxaban for CeREbral Venous Thrombosis; NCT03178864). Currently, we do not use DOACs routinely after CVT but consider them in patients considered to have a high risk of intracranial bleeding with warfarin. However, depending on the results of ongoing trials, including longer-term follow up, DOACs might become the standard of care for CVT in future.
Endovascular treatment
While anticoagulation aims to prevent the progression of the thrombus and alter the balance of thrombosis and lysis, endovascular treatment aims to reduce thrombus burden rapidly either by locally administrating fibrinolytic agents or mechanically removing it.55 56 Small non-randomised studies, case series and case reports describe a recanalisation rate of 70–90%, but with a substantial rate of intracranial haemorrhage of about 10%.56 57 The recently published Thrombolysis or Anticoagulation for Cerebral Venous Thrombosis trial, a randomised blinded-ended trial designed to establish the efficacy of endovascular treatment, was prematurely stopped for futility58 59: at 1-year follow-up, 22 intervention patients (67%) had an Modified Rankin Scale score of 0–1 compared with 23 control patients (68%) (relative risk ratio 0.99, 95% CI 0.71 to 1.38). There were no statistically significant differences in mortality or symptomatic intracranial haemorrhage. We therefore only rarely consider endovascular treatment in severe cases of CVT that do not improve or deteriorate despite anticoagulant therapy; it is probably most effective for acute rather than well-established thrombosis. We recommend full multidisciplinary discussion (neurology, neuroradiology, sometimes neurosurgery) for complex cases before considering endovascular treatment. ESO guidelines (which formally incorporate the factors we consider in clinical discussions) recommend that endovascular treatment should only be considered in patients with a high pretreatment risk of poor outcome13 60 (table 5).
Prognostic score for CVT60
Treatment of elevated intracranial pressure
In the acute phase of CVT, elevated intracranial pressure (due to space-occupying brain oedema, infarction, intracranial haemorrhage) and brain herniation can rapidly lead to severe brain injury and death. Patients judged to have, or to be at high risk of, raised intracranial pressure should ideally be managed on a neurological critical care unit with rapid access to endovascular and neurosurgical teams. Medical therapy for elevated intracranial pressure includes osmotic therapy (such as mannitol), hyperventilation (PCO2 30–35 mmHg) and elevating the head of the bed. Therapeutic lumbar puncture has been proposed to reduce intracranial pressure in patients with CVT and isolated intracranial hypertension,61 but data in acute CVT are inconclusive. Lumbar puncture is safe in patients without lesions on CT scan of head but is contraindicated in patients with large lesions with risk of herniation.62 Similarly, there is no available evidence in favour of carbonic anhydrase inhibitors, such as acetazolamide, although they can be useful in patients with severe headaches or threat to vision. Corticosteroids should not be used except in the presence of underlying inflammatory diseases (eg, Behçet’s disease, systemic lupus erythematosus).
In the presence of brain herniation or midline shift (‘malignant CVT’), medical therapy alone is often not sufficient to control raised intracranial pressure. Decompressive craniectomy allows the swelling brain to expand and could favour collateral vein drainage in CVT by reducing intracranial pressure. No randomised study has been done, so evidence is limited to single-centre small cohort studies, case series and case reports. Observational data suggest that decompressive surgery can be life-saving; it has a favourable outcome in more than 50% of patients, with a mortality rate of 15–18%.5 63 Despite the low quality of available evidence, the ESO-EAN strongly recommend decompressive hemicraniectomy in otherwise well patients with parenchymal lesion(s) and impending herniation.13 Neuroradiological features that should lead to consideration of craniectomy include uncal herniation, midline shift (>5 mm) and herniation-induced ischaemia in the territory of the posterior cerebral artery territory (which is vulnerable to local mass effect and raised intracranial pressure).5 A persistent intracranial pressure >20 cmH2O is also suggested as a criterion for surgery. The optimal timing of anticoagulation after hemicraniectomy is not clear, being reported between 24 hours and 8 days.5 64 The bone flap is often replaced after 3–6 months, when the brain swelling resolves.5 Given the high probability of poor functional outcome in survivors of hemicraniectomy after CVT, a full and frank discussion with the patient (or, more likely, family members or carers) is essential before intervention. Ventricular shunting does not appear to prevent death or herniation, so is not recommended to treat raised intracranial pressure in CVT.6
Seizures
There is limited evidence regarding primary or secondary prevention of seizures in CVT. In those with both a symptomatic seizure and parenchymal injury from infarction or haemorrhage, antiepileptic drug treatment is appropriate. It is less clear whether to treat patients with a seizure but no supratentorial brain lesion, or with a lesion but no clinical seizures; the guidelines are inconsistent. Our practice is generally to treat only those with clinical evidence of seizures. When seizures are treated, it is important to avoid antiepileptic drugs that interact with the planned anticoagulant treatment. There is no evidence about the optimal duration of treatment. We base our practice on current data that suggest for seizures associated with oedema, infarction or haemorrhage, treatment should be continued for at least 1 year.49
PROGNOSIS
CVT generally has a favourable outcome, with a complete functional recovery reported in about 75% of patients; however, about 15% die or are dependent.8 In the acute setting, risk factors for a poor outcome include male sex, older age, confusion or coma, intracranial haemorrhage, deep vein involvement, infection and malignancy (table 5).8 Despite good physical recovery, many survivors have symptoms of depression or anxiety, or cannot return to work because of cognitive impairment.65 Cognitive decline is under-investigated and under-recognised, especially when deep veins are involved, where it is reported in up to one-third of patients.66 The recurrence risk after CVT is quite low: 2–7% for CVT and 4–7% for systemic thromboembolism8; patients with a severe thrombophilic disorder and those stopping anticoagulant therapy early were identified as being at highest risk.11
Further reading
Bousser MG, Ferro JM. Cerebral venous thrombosis: an update. Lancet Neurol 2007;6:162–70.
Saposnik G, Barinagarrementeria F, Brown RD, et al. Diagnosis and management of cerebral venous thrombosis: astatement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2011;42:1158–92.
Ferro JM, Bousser M-G, Canhao P, et al. European Stroke Organization guideline for the diagnosis and treatment of cerebral venous thrombosis - endorsed by the European Academy of Neurology. Eur J Neurol 2017;24:1203–13.
Key points
Cerebral venous thrombosis (CVT) is a rare but important cause of stroke in young adults; its diagnosis is challenging because of the many and varied symptoms, and depends on rapid and appropriate neuroimaging.
Once CVT is diagnosed, it is essential to make a careful search for an underlying cause, for example, oral contraceptive use or thrombophilia (genetic or acquired).
The treatment includes anticoagulation with parenteral heparin, prevention of recurrent seizures, and decompressive neurosurgery in patients with large space-occupying venous infarction, haemorrhage or both; the role of endovascular therapy remains unproven.
Anticoagulation is generally recommended for 3–12 months or longer depending on the estimated risk of recurrence; direct oral anticoagulants are a promising alternative to warfarin, but we await further trial data.
REFERENCES
Footnotes
LU and MS contributed equally
Contributors LU and MS prepared the first draft with DJW. HC, PC and DJW reviewed the manuscript for intellectual content. DJW and PC prepared the figures.
Funding DJW receives research funding support from the British Heart Foundation and the Stroke Association. This work was undertaken at University College London Hospitals NHS Foundation Trust/University College London, who received a proportion of funding from the Department of Health’s National Institute for Health Research Biomedical Research Centres funding scheme.
Competing interests DJW has received honoraria from Bayer, Portola and Alnylam, outside the submitted work.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed by José Ferro, Lisbon, Portugal, and Teddy Wu, Christchurch, New Zealand.
Other content recommended for you
- Current endovascular strategies for cerebral venous thrombosis: report of the SNIS Standards and Guidelines Committee
- Rare presentation of iron deficiency anaemia with cerebral venous sinus thrombosis in a middle-aged woman
- Management and outcome of spontaneous cerebral venous sinus thrombosis in a 5-year consecutive single-institution cohort
- Direct oral anticoagulants in treatment of cerebral venous thrombosis: a systematic review
- Bilateral thalamic lesion presenting as Broca’s type subcortical aphasia in cerebral venous thrombosis: index case report
- Chinese Stroke Association guidelines for clinical management of cerebrovascular disorders: executive summary and 2019 update of clinical management of cerebral venous sinus thrombosis
- Cerebral venous sinus thrombosis: a case series including thrombolysis
- Cerebral venous thrombosis: comparing characteristics of infective and non-infective aetiologies: a 12-year retrospective study
- Endovascular treatment for cerebral venous thrombosis: current status, challenges, and opportunities
- Headache as the only neurological sign of cerebral venous thrombosis: a series of 17 cases