Article Text

Abstract
Among 1–19-year olds, unintentional injuries accounted for 12% of 5.1 million global deaths from injuries in 2010. Despite this high burden, childhood injuries have not received much attention in global health. This paper describes the major causes of deaths from childhood unintentional injuries and provides a review of interventions for reducing this burden. About 627 741 deaths were due to unintentional injuries in 2010 among 1–19-year olds. The proportionate mortality increased with age—from 12.6% among 1–4-year olds to 28.8% among 15–19-year olds. Deaths from Western sub-Saharan Africa and South Asia accounted for more than 50% of all deaths. Rates in these regions are 68.0 and 36.4 per 100 000 population, respectively, compared to 6.4 in Western Europe. Road traffic injuries (RTI) are the commonest cause of death, followed by deaths from drowning, burns and falls. Male children are more predisposed to unintentional injuries except for burns which occur more frequently among females in low and middle income countries (LMICs). Effective solutions exist—including barriers for preventing drowning; safer stoves for burns; child restraint systems for RTI—but the effectiveness of these measures need to be rigorously tested in LMICs. The general lack of a coordinated global response to the burden of childhood unintentional injuries is of concern. The global community must create stronger coalitions and national or local plans for action. Death rates for this paper may have been underestimated, and there is need for longitudinal studies to accurately measure the impact of injuries in LMICs.
- Injury Prevention
- Mortality
- Global Burden
- Policy
- Interventions
Statistics from Altmetric.com
Introduction
The global burden of disease (GBD) studies have guided donors, policy makers and health managers in planning and priority-setting for improving population health outcomes in recent times. The studies categorise major causes of deaths and disability into three major groups, which include: communicable diseases, maternal, perinatal and nutrition conditions (group I); non-communicable diseases (group II); and injuries (group III).1 ,2 According to the GBD estimates, there were 52.8 million total deaths in 2010 and of these, 5.1 million (9.65%) were due to injuries.3 Despite this burden, injury prevention has garnered less attention at all policy levels. This is especially true for the field of child health in low and middle income countries (LMICs) where most discussions have focused on under-fives and interventions for reducing the global burden from group I conditions.4
Over the last two decades, deaths from communicable diseases, including respiratory infections, diarrheal diseases and neonatal disorders that mostly affect under-fives, have declined remarkably; thanks in part to the coordinated effort at all levels to achieve the Millennium Development Goals (MDG).3 ,5 Deaths from injuries have, however, held steady over the same period and the proportionate mortality due to injuries was higher in 2010 (9.6%) compared to the last two decades (8.8%).3 Interestingly, a significant amount of this global burden of injuries is borne by children; of the total 5.1 million estimated deaths due to injuries in 2010, 12.3% of these were childhood deaths from unintentional injuries occurring among individuals between the ages of 1 and 19 years.6
Notwithstanding the high burden, childhood unintentional injuries have not received much attention in the public health community and among global health leaders. To date, few studies have exclusively looked at the global burden of injuries among children of all age groups and very few have provided evidence-based options for confronting this burden as has been done for other major global causes of childhood death.7 The overall goal of this paper is to present a case for active engagement in child injury prevention by the global health actors. The specific objectives are: to use data from GBD 2010 to describe the burden of childhood unintentional injuries; to provide an overview of intervention options for top causes; and to explore policy framework for reducing the burden especially in LMICs. This paper hopes to stimulate a global dialogue on promoting actions for child injury prevention.
Global burden of childhood unintentional injuries
Injury is defined as ‘the physical damage that results when a human body is suddenly subjected to energy in amounts that exceed the threshold of physiologic tolerance—or else the result of a lack of one or more vital elements, such as oxygen’.8 The term ‘unintentional injuries’ as we have used it in this article refers to injury or poisoning that is not inflicted by deliberate means and includes 10 injury categories.i
Analysis conducted using the 2010 GBD data revealed that unintentional injuries accounted for 627 741 (18%) of the estimated 3.5 million deaths among children between the ages of 1 and 19 years globally. This was in contrast to 2.2% of 4.9 million deaths for children under the age of 1 year; as a result, we will focus on the postinfancy period in this paper. A breakdown of these deaths by age groups shows that the proportionate mortality due to unintentional injuries among all causes gradually increases from 12.6% among the 1–4 years to 28.8% among the 15–19 years globally (figure 1D). The proportionate mortality is generally higher in high income countries (HICs) (such as North America and Western Europe) compared to LMIC regions (such as South Asia and sub-Saharan Africa) (figure 1E); for example, it ranges from 11.2% in the Western sub-Saharan Africa region to 41.2% in the high-income North America.

(A) Per cent of global unintentional injury deaths among 1–19-year olds by region. (B) Per cent of global unintentional injury deaths among 1–19-year olds by region and age group. (C) Death rate from unintentional injury among 0–19-year olds by region. (D) Per cent of global unintentional injury deaths among 1–19-year olds by age group (within region). (E) Per cent of global unintentional injury deaths among 1–19-year olds (within region).
This representation of proportionate mortality, however, hides the huge global disparities in absolute count of deaths due to childhood unintentional injuries comparing regions. While Western sub-Saharan Africa and South Asia regions comprise less than 50% of the world's population, these two regions contribute more than 50% of deaths due to unintentional injuries among 1–19-year olds (figure 1A). The disparity becomes even more noticeable when we look only at the 1–4 years age group; 29% of global deaths in this age group occur in Western sub-Saharan Africa which has less than 5% of the world's population compared to a high income region like North America which accounts for only 0.8% of deaths (figure 1B). The global disparities in the burden of unintentional injury are also reflected in the comparison of death rates between regions. Death rate from unintentional injury among 0–19-year olds in Western sub-Saharan Africa region, 67.98 per 100 000 population, is 10 times the rate in Western Europe region, 6.36 per 100 000 population (figure 1C).
Further analysis of the GBD 2010 data shows that road traffic injuries (RTI) are the commonest cause of death from unintentional injuries globally for individuals between the ages of 1 and 19 years (figure 2). They account for about 210 466 deaths and are mostly due to pedestrian (39%) and four-wheel road injuries (33%). Drowning, burns and falls rank as the 2nd, 3rd and 4th commonest cause of death from unintentional injuries, respectively.
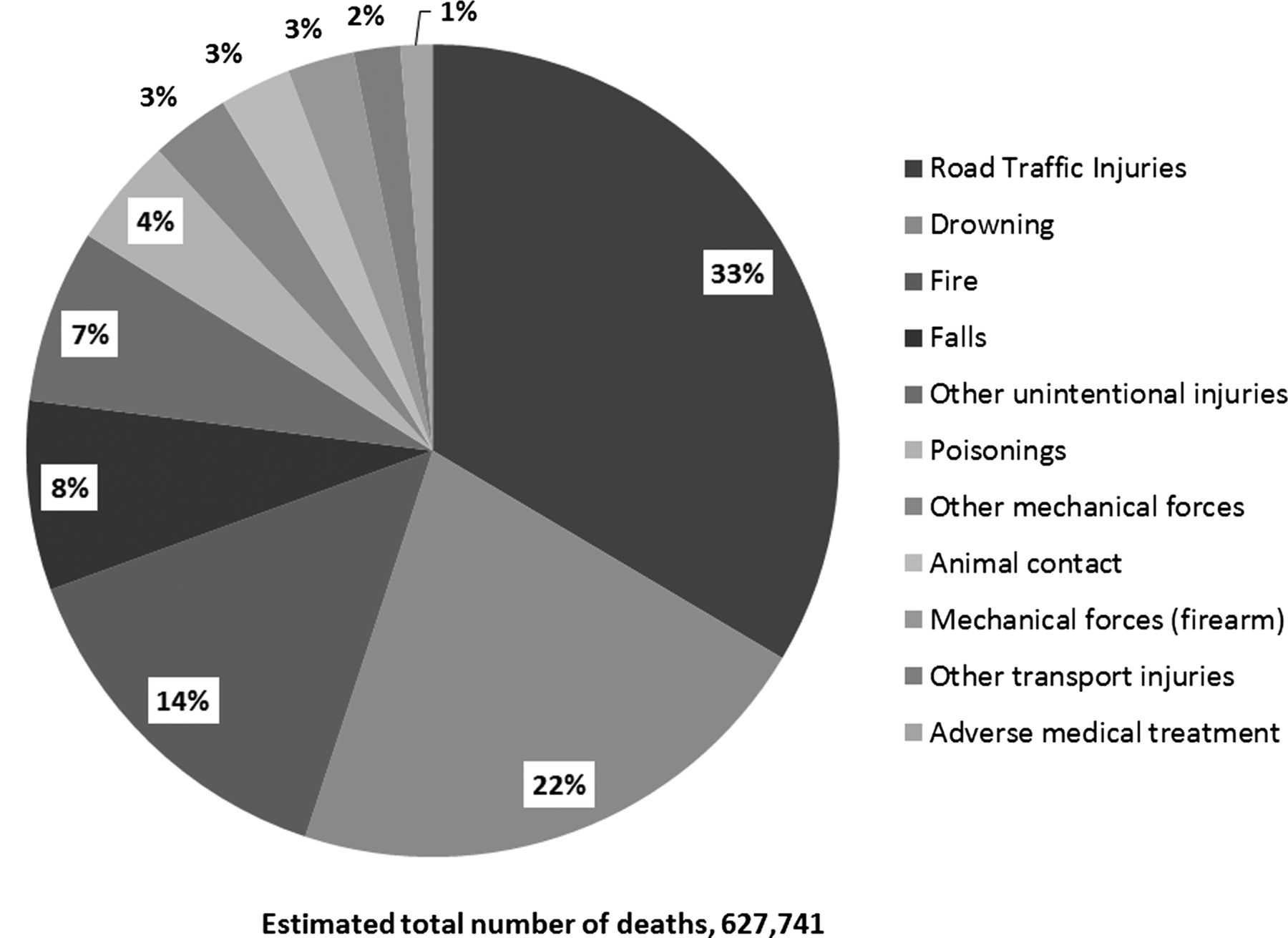
Percentage of deaths from unintentional injuries by specific injury types among 1–19-year olds, global figures in 2010.
Table 1 shows the ranking and counts of injury deaths by regions and demonstrates that close to 50% of the 135 261 estimated global drowning deaths occurs in the South and Southeast Asia regions, while about 30% of the estimated 90 209 global deaths from burns and 20% of the estimated 210 466 global deaths from RTI occur in Western sub-Saharan Africa region alone. Although deaths from RTI rank top in HICs as a major cause of childhood injury deaths, most of these deaths occur in LMIC as shown in table 1.
Top four causes of death from unintentional injuries: ranking of injury types by region
A breakdown of the common causes of death from unintentional injuries by age group and sex (table 2) shows drowning to be the commonest cause among the 1–4-year olds in all LMICs regions except Western sub-Saharan Africa where deaths from RTI and burns rank tops. Indeed, about 46% of all the global deaths from fire among this age group occur in Western sub-Saharan Africa region alone. In the other age groups, deaths from RTI and drowning rank tops in all regions except Western sub-Saharan Africa where burns consistently follows RTI as the second commonest cause of death in all age groups.
Top four causes of death from unintentional injuries: ranking of injury types by age group and region
Male children are generally more predisposed to unintentional injuries in all regions. The percentage of male deaths typically exceeds 55% for all major injury causes by age group, except for burns which occur more frequently among older female children (table 2). Globally, the percentage of male deaths increases with age, on average, for all the major injury causes; except for burns where it decreases with age in the South Asia region, suggesting that young girls growing up in this area are increasingly more predisposed to burns with age.
Potential solutions for confronting the global burden of childhood unintentional injuries
The World Report on Child Injury Prevention (WRCIP) provides a review of interventions that could be implemented to address the major causes of childhood unintentional injuries.4 The report reviewed the strength of evidence for interventions and categorised it into five classes (effective, promising, insufficient evidence, ineffective and harmful) based on the number of studies and consistency of findings. We also supplemented that with a review of the Cochrane Library to identify any systematic reviews that may have been conducted since 2008 as shown in table 3. Some of these interventions are illustrated in figures 3⇓–5.
Potential interventions for addressing the main causes of unintentional injuries

Image—‘fencing to prevent drowning’ used by permission. Photographed by Animesh Biswas, Center for Injury Prevention and Research, Bangladesh.

Image—‘safer cooking area’ used by permission. Photographed by Animesh Biswas, Center for Injury Prevention and Research, Bangladesh.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Image—‘hanging candle holder’ used by permission. Photographed by Bill Birdsall, homepage: http://www.angelfire.com/in2/manythings.
Interventions focused on RTI have perhaps received the most attention in the injury field. In-vehicle child restraint systems have been shown to be very effective based on evidence largely from high income regions,9 and engineering measures that separate pedestrians from vehicles have shown significant promise.4 Use of helmets reduces fatalities and decreases the likelihood of head injury, and these findings are consistent in HICs and LMIC.10 Safety education alone is not sufficient to reduce the burden of road injuries,11 but highly effective when combined with legislation and enforcement of mandatory child restraints and drink-driving laws.4
Evidence seems to support passive interventions, solutions that require little or no action from the individual at risk, as more effective in preventing drowning deaths than active interventions.12 ,13 Hence, engineering measures to eliminate water hazards such as provision of piped water, interposing a barrier between the hazard and the individual such as pool fencing, are known to be very effective.14 ,15 Legislations enforcing pool fencing laws have also been shown to be effective.16 ,17 There is little or no evidence to support the protective effect of swimming lesson. While some have suggested it may lead to increased risk-taking behaviour and lax adult supervision, the real issue may be the need for high-quality studies to assess the effects of swimming lessons in different age groups and settings.4 ,18
Fatal and non-fatal outcomes from burns among children are strongly associated with socioeconomic status and access to medical care.19 ,20 The major sources of burns among children in LMIC are hot liquids, lamps and stoves.21 ,22 Hence, short-term to mid-term solutions that provide safer stoves, lamps and lighting sources, moving these items out of living quarters, have shown some promise in reducing the burden of burns in LMICs.4 Long-term solutions may require engineering measures such as provision of electricity and investment in dedicated burn centres as have been done in high income regions.12 ,23 Battery-powered smoke detectors have been proven to be effective in HICs, especially when combined with education and legislation.24 ,25
Exploring the policy context for childhood unintentional injuries
Situational analysis
A number of reasons have been cited for the lack of a strong global response to the burden of childhood unintentional injuries.26 These include the lack of data on the risks and impact of the problem or the ineffective use of the information on childhood injuries to make a case for global collaboration27; traditional beliefs that injuries are ‘accidents’ which cannot be intervened upon and where a causal explanation exists, the failure to incorporate this understanding in implementing interventions for addressing the injury outcomes26; and the paucity of evidence on the effectiveness and cost-effectiveness of interventions in developing countries.12 ,28
Perhaps, the most important reason may be the way the discourse around child health in LMICs has been construed in recent years. Over the last decades, intervening in child health in LMICs is almost synonymous with addressing issues of communicable diseases and nutritional deficiencies.4 However, deaths from childhood communicable diseases are declining over time and the relative proportion of childhood deaths due to injuries is rising.3 Unfortunately, professionals in the health and medical sector have been slow in catching up to this disease transition.27 Perhaps, this is because the science of energy and injury prevention is not consistent with the prevalent organic causal models for childhood conditions.26 Also, child health service delivery in most LMICs are organised to provide care for preventing and treating childhood communicable diseases with less emphasis on preventing or treating injury outcomes.
Implementing injury prevention interventions requires significant collaborations outside of the medical and public health fields26; and the impact of most interventions is closely associated with the level of human and social development in a particular setting.28 These pose a significant challenge for adopting some interventions that have been successful in HICs to LMICs settings.29 Also, some studies have shown that changing human behaviour, which is usually the target for most health interventions, does not necessarily translate to a reduction in injury fatalities.11 These potential differences between injury and communicable diseases may further challenge adoption of child injury priorities.
The WHO and Unicef issued a global call for action to prevent childhood injuries in 2005 urging stakeholders to include it in priority agenda and to support the development and implementation of global strategy for addressing the issue.29 This was followed by a 10-year action plan to redirect effort at country, regional and global levels to build partnerships and implement effective strategies.30 The action plan aims to coordinate the activities of ministries of health, regional and global offices of the WHO along six main areas of work.ii While similar plans have been adopted in HICs,31 ,32 the policy response from LMICs has been less well coordinated amidst many competing priorities.7
Discussion
The fact that similar injury types (RTI and drowning) are the major causes of death in HICs and LMICs presents an opportunity to adapt effective interventions and transfer knowledge between regions. This will require careful consideration of the context and implementation strategies, external funds and collaboration across all levels.26 ,33 ,34 Some authors have commented that strategies for making injury intervention effective in LMICs may be different compared to HICs.4 ,7 ,28 Perhaps, because the institutional arrangements for implementation differ between regions and success of such programmes are dependent on their acceptability within local context.
It has been suggested that to attract meaningful investment from donors, global health partnerships may be necessary to champion the issue of childhood unintentional injuries.26 These are arrangements between international agencies, NGOs, academia and civil society organised to foster attention on a common cause and often translate into alliances—formal institutional structures created to serve as an organisational base for a cause such as the Global Alliance for Vaccines and Immunisation (GAVI) or Global Alliance for Improved Nutrition (GAIN).26 These alliances were crucial in channelling resources towards issues around communicable diseases and may have contributed significantly to the reduction in the disease burden from these conditions.35 Some authors have, however, cautioned that there are already too many alliances in existence and therefore it might be difficult to organise yet another around childhood injuries with considerable success.36
Partnerships may also be formulated around global campaigns—informal arrangements to promote a particular issue at the global level. For example, WHO has initiated a series of global campaigns on violence prevention in recent years;37 however, these do not appear to be aligned with any partnership or alliance to fund and provide resources. At this point, there are no alliances or global campaigns for child injuries. Indeed, donors may not commit money towards child injury prevention interventions unless they are presented with evidence of effectiveness and cost-effectiveness of these interventions in LMICs along with an accurate characterisation of the burden and active advocacy.
Generating evidence in LMICs settings requires local action and an initial investment in the conduct of implementation research. The inequality in the burden of injuries between LMICs and HICs also exists in the quantity of relevant injury research and capacity to conduct such research.4 ,11 Specific research collaborations between academic institutions in HICs and LMICs on injury intervention studies and other implementation research within populations in LMICs may be a potential solution for addressing this inequality. Current efforts to achieve such collaborations may not be enough and need to be refocused towards implementation science.
The conduct of implementation research would require financial resources and technical know-how in injury research which is still developing in LMICs. Hence, there is a need to build research capacity in collecting routine data for monitoring the burden of injuries, and approaches for distilling evidence for interventions in local settings. Programmes like TEACH-VIP and MENTOR-VIP programmes,38 while reliable, need to be coupled with practical applications through involvement of other key actors such as those involved with the health and management information system at national and local levels.
Injury research is cross-cutting and requires collaboration in multiple discipline including engineering, medicine, law and social sciences. This is true also for the delivery of interventions for addressing the burden of injuries, especially at the national and local levels, which require collaboration among professionals working in different sectors.26 ,39 Unfortunately, professionals in the field of health and medicine work in non-intersecting lacunae; reaching out to colleagues is thus key for promoting child injury prevention.
We commend the scientific effort of studies like GBD 2010 to capture accurate global health information; however, the data from LMICs—especially injury data—are fraught with inaccuracies.40 Better uses of data from health and demographic surveillance system in LMICs have been suggested by the INDEPTH network as one possible solution for getting more accurate data.41 These provide population-based estimates (though not necessarily representative) of the local and regional areas. Other approaches to improve the data context include the development of national injury surveillance systems and inclusion of injury modules in existing national health and demographic surveys.42 ,43
The thrust of health systems in LMICs has been universal health coverage for basic health services. This is often interpreted in child health service delivery as the provision of immunisation services, treatment of communicable diseases and nutritional deficiencies in primary healthcare centres. However, to combat the growing pandemic of childhood injuries, new components of health services that focus on prevention of childhood unintentional injuries and provision of emergency care have to be incorporated into the basic package of health services in most LMICs.44 This will require new training for health service providers and provision of basic infrastructure for provision of such services.
Conclusion
Unintentional injuries are a major cause of childhood deaths globally, and the burden of these deaths is disproportionately borne by populations in LMICs. The main causes of deaths from unintentional injuries among children are RTI, drowning, burns and falls. Potential interventions exist for addressing these causes. However, they need to be first tested in LMICs. There is an urgent need for a global response to the burden of childhood unintentional injuries. This will require major coalitions, alliances and strategic relationships among multiple stakeholders at various levels and a paradigm shift in the way we collect and use health data, prioritise resources and organise health services delivery.
Acknowledgments
We will like to acknowledge Dr Animesh Biswas of the Center for Injury Prevention and Research, Bangladesh and Bill Birdsall for providing the photographs used to illustrate some of the intervention options.
References
Footnotes
-
Contributors OA conducted the data analyses and reviews; and drafted the original manuscript. AA provided the conceptual framework for the manuscript and edited it for intellectual content. OA and AA conducted the revision on the published version.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.
-
↵i Categories of unintentional injuries: road traffic injury (pedestrian road injury, bicycle road injury, two-wheel road injury, four-wheel road injury, other road injury); other transport injury; falls; drowning; fire/burns; poisonings; exposure to firearm (accident discharge); exposure to other mechanical forces (sharp objects, machine); adverse medical treatment (injuries from error in medical and surgical procedures).
-
↵ii WHO six main areas of work: strengthening of country-level standardised data collection measures on injury outcome and cost; developing research agenda on child injuries and interventions; identifying and scaling up of country-level preventive strategies; providing technical support for country-level implementation of prehospital trauma care system and other best practices; capacity development for data collection and injury research through scholarship and mentoring.