Article Text

Abstract
Context: Coronary artery disease (CAD) is a major cause of mortality and ill health.
Objective: To assess whether 64-slice CT angiography might replace some coronary angiography (CA) for diagnosis and assessment of CAD.
Data sources: Electronic databases, conference proceedings and reference lists of included studies.
Study selection: Eligible studies compared 64-slice CT with a reference standard of CA in adults with suspected/known CAD, reporting sensitivity and specificity or true and false positives and negatives.
Data extraction: Two reviewers independently extracted data from included studies.
Results: Forty studies were included; 28 provided sufficient data for inclusion in the meta-analyses, all using a cut off point of ⩾50% stenosis to define significant CAD. In patient-based detection (n = 1286) 64-slice CT pooled sensitivity was 99% (95% credible interval (CrI) 97% to 99%), specificity 89% (95% CrI 83% to 94%), median positive predictive value (PPV) across studies 93% (range 64–100%) and negative predictive value (NPV) 100% (range 86–100%). In segment-based detection (n = 14 199) 64-slice CT pooled sensitivity was 90% (95% CrI 85% to 94%), specificity 97% (95% CrI 95% to 98%), median PPV across studies 76% (range 44–93%) and NPV 99% (range 95–100%).
Conclusions: 64-Slice CT is highly sensitive for patient-based detection of CAD and has high NPV. An ability to rule out significant CAD means that it may have a role in the assessment of chest pain, particularly when the diagnosis remains uncertain despite clinical evaluation and simple non-invasive testing.
Statistics from Altmetric.com
Coronary artery disease (CAD) is a major cause of mortality and ill health, resulting in an estimated 7.6 million deaths globally in 2005.1 In the United Kingdom it causes around 101 000 deaths each year2 and is the most common cause of death. Currently, invasive coronary angiography (CA) is regarded as the “gold standard” for the assessment of coronary anatomy. However, conventional CA has limitations. It is an invasive procedure with a small (0.1–0.2%) risk of major complications3 and affords information only on the site and degree of luminal narrowing—providing no data on the extent of atherosclerotic change within the vessel wall. Images are obtained in only two dimensions—though the use of multiple projections enables a more comprehensive assessment of any individual lesion. Finally, there are constraints on the amount of CA that can be undertaken, in terms of the infrastructure and cardiologist time. An accurate non-invasive test for diagnosing CAD that could potentially avoid the need for some CA is, therefore, highly desirable.
Multislice computed tomography (MSCT) has been developing rapidly in recent years. Four-slice machines appeared in 1998, 16-slice in 2001 and 64-slice in 2004. This has resulted in greatly increased temporal and spatial resolution4—facilitating the rapid identification and assessment of atherosclerosis within the moving coronary arteries5 6 and generating considerable interest in the concept that MSCT might potentially reduce the need for invasive CA. The aim of this systematic review was to assess the accuracy of 64-slice CT angiography compared with conventional CA in the diagnosis and assessment of CAD.
METHODS
Search strategy
Highly sensitive search strategies were developed using both appropriate subject headings and text word terms. Full details of the search strategies used are available from the authors. We searched the following electronic databases: Medline (2002– November week 3, 2006), Embase (2002 to December 2006), Biosis (2002 to December 2006), Science Citation Index (2002 to December 2006), Medline In-Process (14th December 2005), Cochrane Controlled Trials Register (The Cochrane Library, issue 4, 2006), Cochrane Database of Systematic Reviews (The Cochrane Library, issue 4, 2006), Database of Abstracts of Reviews of Effectiveness (December 2006), HTA Database (December 2006) and Health Management Information Consortium (2002 to May 2006). In addition, recent conference proceedings and reference lists of all included studies were scanned to identify additional potentially relevant studies. Searches were from 2002 onwards and restricted to English language reports.
Inclusion criteria
We included randomised controlled trials, non-randomised comparative studies or case series involving adults with suspected or known CAD. The index test was 64-slice CT angiography compared with conventional CA as the reference standard. Studies had to report sensitivity and specificity or true and false positives and negatives.
Data extraction
One reviewer screened the titles (and abstracts if available) of all reports identified by the search strategy. Full copies of potentially relevant reports were obtained and two reviewers independently assessed them for inclusion. Data were extracted independently by two reviewers. Disagreements were resolved by consensus or arbitration by a third reviewer.
Quality assessment
Two reviewers independently assessed the methodological quality of full-text studies using QUADAS,7 which was modified to make it more applicable to studies for diagnosing and assessing CAD. Three questions in the original QUADAS tool that related to the quality of reporting rather than methodological quality were excluded (questions 2, 8 and 9). Three questions were added: (a) whether an established cut-off point was used (question 12); (b) whether data on observer variation were reported and within an acceptable range (question 13) and (c) whether data were presented for appropriate subgroups of patients (question 14). Disagreements were resolved by consensus or arbitration by a third reviewer.
Statistical analysis
Where three or more studies reported data, summary receiver operating characteristic (SROC) curves were derived for the following levels of analysis: patient, segment, artery (left main, proximal left anterior descending (LAD), any LAD, left circumflex (LCX), right coronary artery (RCA)), stent and coronary artery bypass graft (CABG). The meta-analysis method used was the hierarchical SROC model,8 fitted using WinBUGS 1.4.9 A symmetric SROC model was used to address the lack of numerical convergence of the full SROC model. Pooled estimates for sensitivity and specificity were reported as medians and 95% credible intervals (CrIs), the Bayesian equivalent of confidence intervals (CIs).
If numerical difficulties were encountered with the symmetric hierarchical SROC model and there was also no evidence of heterogeneity, sensitivity and specificity were pooled using the weighted average method.10 These analyses were carried out using Meta-DiSc software11 and corresponding 95% CIs (rather than CrIs) were reported. This approach was required for the left main artery analysis. Heterogeneity was assessed using the I2 statistic in Meta-DiSc software,11 with a value >50% considered to represent substantial heterogeneity.12
RESULTS
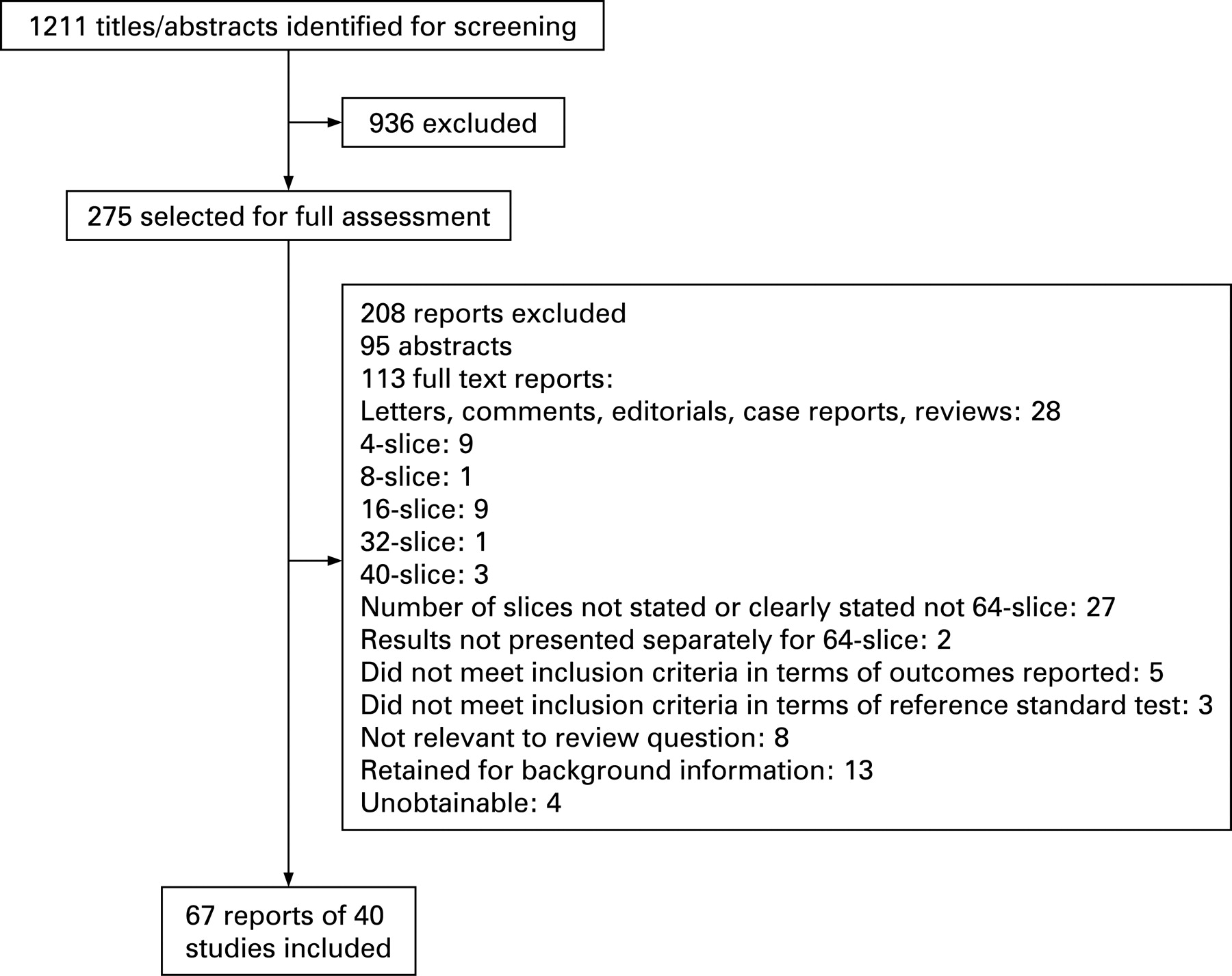
Figure 1 shows the flow of studies through the review. Out of a total of 1211 titles/abstracts screened, 275 were selected as potentially relevant and full papers obtained where possible. Forty studies (21 full text,13–33 19 abstracts34–52), published in 67 reports, met the inclusion criteria. All were non-randomised studies comparing 64-slice CT with a reference standard of invasive CA.

The characteristics of the included studies are available as supplementary table 1. The 40 studies involved more than 2400 people. In 25 studies reporting gender 67% (n = 1184) of participants were men. Across 27 studies reporting mean age this ranged from 54 to 69 years (median 61 years). Most studies reported elective assessment for CAD, with study groups including those with suspected CAD, known CAD, or both. In addition, the following specific groups were studied: patients with previous percutaneous coronary intervention or CABG and those with a suspected acute coronary syndrome.
All studies used 64-slice CT angiography. Most studies (n = 28) used Siemens Sensation 64 machines; other types of equipment used included GE Healthcare Light-Speed VCT (n = 2), Philips Brilliance 64 (n = 2) and Toshiba Multi-Slice Aquilion 64 (n = 1).
Figure 2 summarises the quality assessment for the 21 full-text studies. In all studies conventional CA was the reference standard, results were abstracted only if patients received both 64-slice CT angiography and the reference standard (partial verification bias avoided), patients received the same reference standard (differential verification bias avoided) and the index test did not form part of the reference standard (incorporation bias avoided). In 85% of studies those interpreting 64-slice CT data were blinded to the results of the reference standard test (test review bias avoided) and in 71% of studies vice versa (diagnostic review bias avoided). In 48% of studies the participants belonged to specific groups (spectrum bias)—for example, those with previous revascularisation.

Twenty-eight studies provided sufficient data (true positives, false positives, false negatives, true negatives) to allow their inclusion in the meta-analyses, although the number of studies included for each level of analysis varied (table 1). Figure 3 shows the pooled estimates for the sensitivity and specificity of 64-slice CT angiography for detecting significant CAD for each level of analysis (also available in supplementary table 2). Across studies the median positive predictive value (PPV) and negative predictive value (NPV) along with their ranges for each level of analysis are shown in fig 4 (also available in supplementary table 2). All studies used a cut-off point of >50% or ⩾50% stenosis to define significant CAD.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patient- and segment-based analyses
In 18 studies (n = 1286) 64-slice CT was extremely sensitive in patient-based detection of CAD, with a pooled sensitivity of 99% (95% CrI 97% to 99%). Specificity was lower at 89% (95% CrI 83% to 94%). The median NPV across studies was very high at 100% (range 86–100%), while PPV was 93% (range 64–100%). The wide range of PPVs is probably due to the studies being heterogeneous in terms of their populations and the prevalence of significant CAD (median across studies 58%, range 23–96%). The median false positive rate across studies was 10% (range 0–50%), representing an overestimation of the presence of non-significant stenosis as significant, as opposed to finding CAD where none existed. There was very low statistical heterogeneity for sensitivity (I2 = 0.1%) and moderate statistical heterogeneity for specificity (I2 = 31.7%).
In 17 studies reporting coronary artery segment-based detection (n = 14 199), compared with patient-based detection, pooled sensitivity was lower (90%, 95% CrI 85% to 94%), specificity higher (97%, 95% CrI 95% to 98%), median PPV lower (76%, range 44–93%) and NPV similar (99%, range 95–100%).
Five of 18 studies in the pooled estimates for patient-based detection of CAD, and three of 17 for segment-based detection, were abstracts. A sensitivity analysis undertaken to examine the effect of removing abstracts from the pooled estimates found that this did not affect the results. For patient-based detection sensitivity remained unchanged at 99% (95% CrI 97% to 99%), while specificity increased slightly to 91% (95% CrI 84% to 95%). For segment-based detection sensitivity also remained unchanged at 90% (95% CrI 84% to 94%), while specificity decreased slightly to 96% (95% CrI 94% to 98%).
Artery level analyses
At artery level pooled sensitivity and specificity were both highest for the left main artery (95% (95% CI 84% to 99%); 100% (95% CI 99% to 100%), respectively). Pooled sensitivity was lowest for the LCX at 85% (95% CrI 69% to 94%). Pooled specificity estimates for all of the arteries were very high at ⩾96%. Across studies the median PPV and NPV were also both highest for the left main artery (100%, range 90–100%; 100% (all five studies) respectively). The median NPVs for all of the arteries were very high at ⩾98% (ranges: LAD 95–100%; LCX 93–100%; RCA 94–100%). The median PPV was lowest for the LCX (81%, range 56–100%).
Specific subgroups
In six studies reporting patency of stents (n = 317), with a cut-off point >50% or ⩾50% in-stent restenosis defining a positive test result, sensitivity was 89% (95% CrI 68% to 97%) and specificity 94% (95% CrI 83% to 98%), while across studies the median PPV was 77% (range 33–100%) and NPV was 96% (range 71–100%). Stents caused some problems for 64-slice CT. Leber and colleague reported that of nine stents without any restenosis on conventional CA four were false positives on 64-slice CT due to artefacts caused by the dense stent material.18 Importantly, the utility of CT angiography appears to be greatly influenced by the diameter and strut thickness of the stent.29 In three studies 21% (59/276) of stents were classed as unevaluable and excluded from analysis,28 29 36 while the remaining three studies did not report this information.
Four studies reported patency of bypass grafts (n = 543). Both sensitivity and specificity were very high (99%, 95% CrI 95% to 100%; 96%, 95% CrI 86% to 99%, respectively), while across studies the median PPV was 93% (range 90–95%) and NPV was very high at 99% (range 98–100%).
Only three studies assessed the diagnostic performance of 64-slice CT in patients admitted to hospital with suspected acute coronary syndromes (n = 232).16 35 46 Across these studies the median (range) values were 100% (97–100%) for sensitivity, 100% (79–100%) for specificity, 100% (87–100%) for PPV and 100% (94–100%) for NPV.
Technical limitations
Scans could not be adequately evaluated in 2% (11/718) of patients (n = 13 studies), 8% (997/12 476) of all arterial segments, 21% (59/276) of stented segments (n = 3 studies) and 0% (0/231) of bypass grafts (n = 2 studies). Three per cent (11/404) of scans of the left main artery, 5% (74/1641) of the RCA and 6% of both the LAD (104/1789) and the LCX (93/1444) could not be evaluated. Studies reported that poor image quality was caused by factors including irregular heart rhythm, sinus tachycardia >90/min, calcification, vessel motion or small vessel calibre in distal segments.
It is unclear to what extent the exclusion or otherwise of small diameter vessels affected 64-slice CT performance as only seven studies provided this information, with five excluding segments <1.5 mm in diameter from analysis19 23 25 30 31 and two analysing all vessels regardless of size.20 27 Across the five studies excluding segments <1.5 mm the median sensitivity was 87% (range 85–94%) and specificity 96% (range 76–97%) compared with median sensitivity of 90% (range 86–94%) and specificity of 96.5% (range 95–98%) for the two studies analysing all segments.
Coronary artery calcification may make scans more difficult to interpret. Ghostine and colleagues noted that heavily calcified segments accounted for 21 (81%) of 26 false negative results.15 In the study by Raff and colleagues the false positive rate increased as calcification became more severe, with a 2% (14/709) false positive rate in segments rated as “no calcification”, 6% (5/89) in those rated as “mild”, 13% (6/48) in those rated as “moderate” and 18% (16/88) in those segments rated as “severe”.27
DISCUSSION
This study suggests that 64-slice CT angiography is highly sensitive for patient-based detection of significant CAD (⩾50% stenosis), with a very high NPV. This high NPV was also apparent in analyses based on individual coronary arteries and segments. At artery level the best results for 64-slice CT were in those arteries such as the left main and LAD arteries where significant CAD carries the poorest prognosis. Based on a few small studies, broadly similar results were demonstrated in patients who had undergone prior coronary artery stenting, CABG and those with a suspected acute coronary syndrome.
Prior studies
We did not identify any other published systematic reviews focusing on 64-slice CT. Several systematic reviews of MSCT5 6 53–55 included 64-slice CT studies, all of which are included in our review. A systematic review by Stein and colleagues5 of multidetector (four-slice and higher) CT for the diagnosis of CAD identified one 64-slice CT study by Leschka and colleagues.19 The authors concluded that the preliminary data with 64-slice CT suggested that it was more sensitive and specific than 16-slice CT, and that multidetector CT had the potential to be used as a screening test in appropriate patients. The USA Technology Evaluation Center6 (a subsidiary of the private providers Blue Cross and Blue Shield), in a review of CT angiography (32-slice or higher) identified six 64-slice CT studies.18 19 21 26 27 30 The authors reported that in patient-based analysis the 64-slice CT studies showed high sensitivities and specificities compared with the reference standard of conventional coronary angiography.6 A technology assessment by Patel and colleagues,54 undertaken for the USA Medicare Coverage Advisory Commission included CT angiography (16-slice or higher) and identified six 64-slice CT studies.14 18 19 21 27 30 The authors concluded that the sensitivity and specificity of 64-slice CT in patient-based analysis looked promising.54 Systematic reviews and meta-analyses by Sun and colleagues55 (four-slice or higher) and Hamon and colleagues53 (16-slice or higher) identified seven14 18 19 21 26 27 30 and nine13 18 19 21 22 26 27 30 32 64-slice CT studies, respectively. Both reviews undertook meta-analyses at patient, vessel and segment level, although neither presented separate pooled estimates for the group of 64-slice CT studies. In patient-based analysis Sun and colleagues55 reported pooled estimates (95% CI) of 91% (88% to 95%) sensitivity and 86% (81% to 92%) specificity. The authors concluded that diagnostic accuracy was significantly improved with 64-slice scanners compared with four- and 16-slice scanners.55 In patient-based analysis Hamon and colleagues53 reported pooled estimates (95% CI) of 96% (94% to 98%) sensitivity and 74% (65% to 84%) specificity. The authors concluded that MSCT had shortcomings difficult to overcome in daily practice, with continuing moderate specificity in patient-based analysis in patients with high prevalence of CAD. They stated that studies evaluating the diagnostic performance of the newest-generation MSCT, and including patients with low to moderate CAD prevalence, would be critical in establishing the clinical role of this emerging technology as an alternative to CA.53
Radiation doses
Although CT is regarded as non-invasive, it delivers a higher radiation dose than conventional CA and concerns have been raised about indiscriminate or repetitive use and, in particular, the risks in younger people or women of childbearing age.56 Hausleiter and colleagues57 reported an effective mean (SD) radiation dose of 11.0 (4.1) mSv for 64-slice CT. By comparison estimates of mean effective doses for conventional CA include <5 mSv by a British Cardiovascular Society Working Group,58 and 4–8 mSv by the Technology Evaluation Center.59 In this review six studies15–18 22 28 reported a 64-slice CT radiation dose for the patient population as a whole and six20 21 26 27 30 31 reported it separately for men and women. The radiation dose for men ranged from 7.5 mSv30 to 15.2 mSv20 21 and for women from 10.2 mSv31 to 21.4 mSv.20 21 Two30 31 of these studies, using ECG-controlled dose modulation to reduce the tube current during systole, reported the lowest radiation doses: 7.5 mSv30 and 8.6 mSv31 for men and 10.2 mSv30 and 12.2 mSv31 for women. One study19 used an alternative technique, automatic exposure control,60 to reduce radiation dose exposure but did not report the actual dosage values that the patients received. With the development of more modern technologies and methods, it may be possible to reduce the radiation dose further. Einstein and colleagues61 have estimated that a single 64-slice CT scan would result in an increase in lung cancer and breast cancer risk, especially if used in younger patients (for example, an estimated lifetime attributable cancer risk of up to 1 in 114 after a combined heart and aortic scan in a 20-year-old woman, compared with 1 in 715 for a 60-year-old woman after a heart scan using ECG-controlled dose modulation).
Strengths and limitations
The current review included both full-text studies and conference abstracts in an attempt to obtain the latest available data. All studies used the same reference standard of conventional CA and only data for those who received both index test and reference standard were included in the meta-analyses. A limitation was that non-English language studies were excluded. No adjustment was made for studies which used multiple samples from each participant for some levels of analysis.
Implications for practice
Given the high sensitivity and NPV, the main role of MSCT may be to rule out significant CAD, and thereby reduce the need for invasive CA. There are several clinical situations where this may be particularly useful. In patients with a very low probability of CAD it is unlikely that MSCT would be recommended, particularly given the radiation doses involved. Likewise, when the probability of CAD is high conventional angiography is likely to remain the preferred investigation in most patients. However, very many patients fall into an intermediate category where the diagnosis of CAD remains uncertain after clinical assessment and simple non-invasive testing. Currently, this may necessitate either myocardial perfusion scanning or invasive CA. It seems likely that MSCT may have an increasing role in this setting.
There are other specific settings where MSCT may be of particular value. For example, in patients with acute chest pain a test with the ability to rule out significant CAD rapidly and effectively—or provide a definitive diagnosis—has obvious potential. The limited data currently available suggest that this may indeed be the case.62 In patients with a history of CABG invasive angiography may be more technically difficult, time consuming and associated with higher radiation doses. MSCT may, therefore, have some advantages in selected patients after surgical revascularisation. Likewise, many patients who are scheduled to undergo surgery for valvular heart disease and other non-coronary cardiac conditions currently undergo “routine” invasive angiography—much of which might be replaced by MSCT.20 63
CONCLUSION
Although further work is required to determine the prognostic utility of MSCT and to clarify its precise clinical role, the currently available data suggest that it will play an increasing role in the evaluation of patients with known or suspected CAD. The technology continues to evolve and data are awaited on the marginal costs and benefits of the next generation of MSCT, the 256 and higher-slice CT machines.
Acknowledgments
NW designed the study. CF developed the search strategies, obtained papers and formatted the references. GM screened the search results. GM and XJ undertook data extraction and quality assessment. JAC and GM analysed and interpreted data. GM drafted the manuscript. GH, SW and NW provided expert advice. All authors commented on drafts and approved the final manuscript. GM is guarantor.
REFERENCES
Supplementary materials
web only appendix 94/11/1386
Files in this Data Supplement:
Footnotes
Competing interests: None.
Funding: This paper was developed from a Health Technology Assessment of the clinical and cost-effectiveness of 64-slice or higher computed tomography angiography as an alternative to invasive coronary angiography in the investigation of coronary artery disease, which was funded by the UK National Institute for Health Research Health Technology Assessment programme (project number 06/15/01). The Health Services Research Unit is core funded by the Chief Scientist Office of the Scottish Government Health Directorates.
The authors’ work was independent of the funding source. The views expressed in this report are those of the authors and not necessarily those of the funders
▸ Additional tables are published online only at http://heart.bmj.com/content/vol94/issue11