Article Text

Statistics from Altmetric.com
Learning objectives
Develop an understanding of extracorporeal membrane oxygenation (ECMO) and the differences between veno-venous and veno-arterial ECMO.
Develop an understanding of the range of conditions that can be managed with ECMO and the contraindications.
Develop an appreciation of the common complications that patients suffer when supported with ECMO.
Introduction
Extracorporeal membrane oxygenation (ECMO) is an advanced form of temporary life support, to aid respiratory and/or cardiac function. It has been used since the early 1970s and is based on cardiopulmonary bypass technology and diverts venous blood through an extracorporeal circuit and returns it to the body after gas exchange through a semi-permeable membrane. ECMO can be used for oxygenation, carbon dioxide removal and haemodynamic support. Additional components allow thermoregulation and haemofiltration. The two most common forms of ECMO are veno-venous (VV) and veno-arterial (VA). In VV-ECMO, used to support gas exchange, oxygenated blood is returned to a central vein. In VA-ECMO, used in cases of cardiac or cardiorespiratory failure, oxygenated blood is returned to the systemic arterial circulation, bypassing both the heart and lungs.
History
The first adult survivor of ECMO was reported in 1972 in a patient who developed respiratory failure following a trauma.1 This was followed in 1976 with report of successful outcomes in moribund infants.2 The first randomised controlled trial (RCT) of VV-ECMO was performed in 1979 in 90 adult patients with respiratory failure and reported a high mortality rate and ECMO-associated complications.3 Today, this outcome is attributed to the old ECMO technology used and poor ventilatory management of patients. This trial diminished significantly the initial enthusiasm for ECMO in adult patients even if good outcomes continued to be observed when ECMO was used in young patients.4 In 1989, a group of enthusiast clinicians formed the Extracorporeal Life Support Organization (ELSO) and established a voluntary registry to help advance ECMO technology and practice. Subsequent demonstration of benefits in paediatric ECMO5 encouraged clinicians to test the use of VV-ECMO in adult patients with respiratory failure. This led to another multicentre RCT in adults (the conventional ventilation or extracorporeal membrane oxygenation for severe adult respiratory failure trial).6 In this trial, patients randomised to receive VV-ECMO in a single referral centre had a 63% survival to 6 months without disability compared with 47% for those patients who were not transferred to the referral centre. Only a proportion of the transferred patients were supported with VV-ECMO and there was no statistically significant difference in outcome between patients who were supported with VV-ECMO when compared with the ones who were not. Around the same time, the extensive use of VV-ECMO during the H1N1 pandemic with substantiated evidence7 led to a rapid increase of its use in patients with acute respiratory failure due to H1N1 and other conditions. In 2011, the National Health Service in England commissioned a National VV-ECMO service to provide support for those patients presenting with an acute respiratory failure anywhere in England. The last RCT of the use of VV-ECMO in the respiratory patient has shown no benefit of ECMO itself,8 but the trial validity was commented on9–11 and a subsequent Bayesian analysis challenged the initial results.12
Concomitantly to these trials in the patients with acute respiratory distress, clinicians increased the use of ECMO to support other conditions such as isolated cardiac or cardiorespiratory failure. This has continued to increase as demonstrated by multiple case reports and some case series.13 A large propensity matched trial was published14 and suggested benefits of using VA-ECMO in patients who suffer a cardiac arrest in hospital.
Supporting a variety of patients with ECMO has continued to expand and is now used in multiple conditions where heart and/or lungs have failed.
Indications
While there are no widely agreed guidelines on the indications and contraindications for ECMO support, there are consensus statements, and ELSO has published recommendations for the use of ECMO in critically ill patients.15 16
Veno-arterial extracorporeal membrane oxygenation
VA-ECMO can help support patients with cardiogenic shock that is refractory to maximal therapy (which may include inotropic drugs and intra-aortic balloon pump therapy) (box 1).17 It can be used for patients who are believed to have a reversible cause of their cardiogenic shock or as a bridge to further mechanical circulatory support, such as a ventricular assist device, or cardiac transplantation. Other percutaneous mechanical circulatory support devices exist such as the percutaneous axial flow devices: TandemHeart system (CardiacAssist) and the Impella (Abiomed) and can be used as an alternative in certain situations.18 VA-ECMO can also be a salvage treatment option in the setting of cardiac arrest with unsuccessful advanced life support. So-called ‘extracorporeal cardiopulmonary resuscitation’ (eCPR) may be considered especially when cardiac arrest occurs in an intensive care or cardiac catheter laboratory setting where VA-ECMO can be rapidly instituted,19–21 but is being used in the prehospital setting in some countries.22 Although there are no RCTs, recent guidance has been published suggesting that for suitable patients, a ‘collapse-to-start eCPR interval’ of 60 min and a ‘door-to-extracorporeal life support implantation time’ of <30 min should be the goal.23
Indications for cardiac veno-arterial extracorporeal membrane oxygenation (VA-ECMO)
Potential indications for cardiac ECMO
Acute myocardial infarction
Fulminant myocarditis
Acute exacerbations of chronic heart failure
Cardiac failure due to intractable arrhythmias
Postcardiotomy cardiac failure
Primary graft failure following cardiac transplantation
Acute heart failure secondary to drug toxicity
Postcardiac arrest (as part of advanced life support)
Concomitant respiratory failure is not a requirement for considering VA-ECMO over other forms of mechanical circulatory support and in fact, cardiac-associated respiratory failure due to pulmonary oedema can be exacerbated by VA-ECMO in the absence of adequate left ventricular emptying. In this situation, alternative support can be considered, for example, it is now possible to incorporate ECMO components, such as an oxygenator, into a ventricular assist device circuit—hence providing a hybrid system with extracorporeal membrane oxygenation.
Veno-venous extracorporeal membrane oxygenation
Support with VV-ECMO is indicated for patients with acute respiratory failure with refractory hypoxaemia or hypercapnia despite optimal ventilation (box 2). It is instituted in patients presumed to have a reversible cause for their respiratory failure. VV-ECMO allows to decrease the ventilatory insult caused by mechanical ventilation. In the setting of isolated respiratory failure, VV-ECMO is preferred since lung perfusion maintains endocrine pulmonary function. VV-ECMO is simpler to use and has a lower rate of complications than VA-ECMO.24
Indications for respiratory veno-venous extracorporeal membrane oxygenation (VV-ECMO)
Examples of indications for support with VV-ECMO
Reversible causes of acute respiratory failure
Acute respiratory distress syndrome associated with viral or bacterial pneumonia
Graft dysfunction following lung transplantation
Trauma—extensive pulmonary contusion
Pulmonary embolism
Inability to provide adequate gas exchange without risk of ventilatory injury
Pulmonary haemorrhage
Severe bronchospasm
Contraindications
Support with ECMO is an advanced form of life support with significant inherent risk and the decision to commence therapy should not be taken lightly. A multidisciplinary team should be involved in all decisions with involvement of cardiology and respiratory physicians, cardiothoracic surgeons and specialist intensivists. Careful patient selection is essential with consideration of comorbidities and clinical prognosis (box 3). The use of ECMO is contraindicated in patients with non-recoverable cardiac or respiratory failure who are not candidates for transplantation or permanent mechanical support.15 25 However, this status may not be known at the time of presentation and ECMO can be used as a ‘bridge to decision’ and as a ‘bridge to candidacy’ if it is believed that a patient may become a candidate for transplantation.
Situations in which extracorporeal membrane oxygenation (ECMO) is unlikely to be successful (modified from Schmidt et al47)
Situations in which ECMO is unlikely to be successful
Wrong choice of ECMO configuration
Chronic respiratory or cardiac disease with no hope of recovery or transplant
Out-of-hospital cardiac arrest with prolonged low blood flow
Severe aortic regurgitation or type A aortic dissection if using veno-arterial ECMO
Refractory septic shock in adults with preserved left ventricular function
Allogeneic stem cell transplantation
Advanced age in acute respiratory distress syndrome
Acute respiratory distress syndrome with advanced multiorgan failure
Prolonged pre-ECMO mechanical ventilation
Centre inexperienced with ECMO
Relative contraindications for ECMO support include contraindications to therapeutic anticoagulation (such as active bleeding), severe peripheral arterial disease (not relevant for VV-ECMO) and pre-existent severe multiorgan failure.25 26 When the circuit involved arterial access (VA-ECMO), severe aortic regurgitation and aortic dissection are contraindications.
ECMO circuit design
ECMO circuits consist of vascular access cannulae, tubing coated with an anticoagulant, a centrifugal pump, a polymethylpentene hollow-fibre oxygenator (figure 1), a temperature control system, monitors and access points. Additional components, such as a haemofilter can be incorporated into the circuit as required. Cannulation can be performed percutaneously, or in the case of VA-ECMO, centrally via sternotomy.27 28
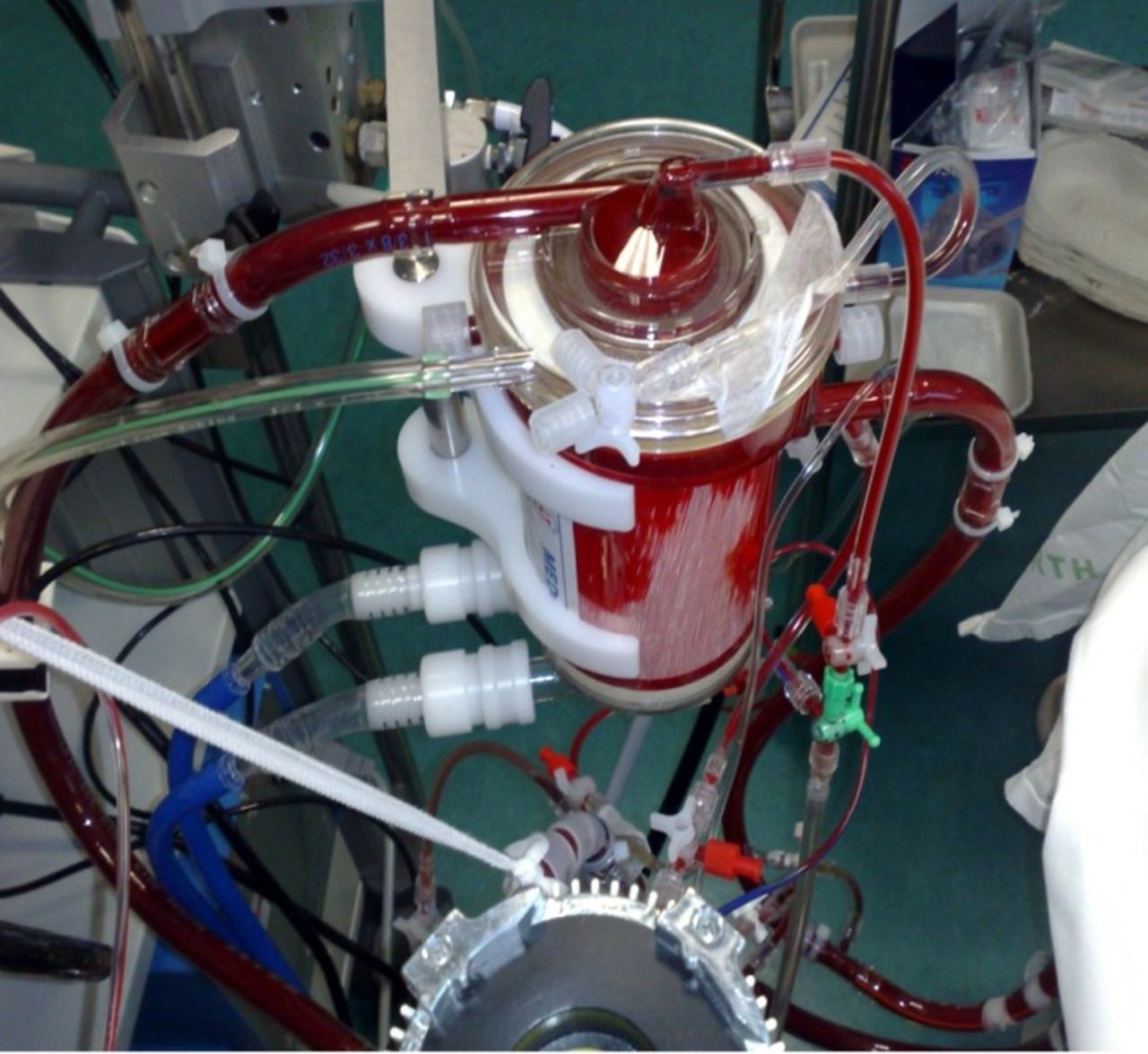
Photo of a membrane oxygenator.
Veno-venous extracorporeal membrane oxygenation
In support with VV-ECMO, access to the central venous system is required. Deoxygenated blood is drained from the vena cavae and oxygenated blood is returned to the right atrium. Traditionally this has been performed with two separate cannulae, using femoral and internal jugular veins, accessed percutaneously or by surgical cut-down. One problem that can occur is mixing and recirculation, if the cannulae are positioned suboptimally. Recirculation occurs when returned oxygenated blood is immediately drained back to the ECMO circuit through the drainage cannula.
Dual lumen cannulaes have been designed and they efficiently drains blood from the superior and inferior cavae, and returns oxygenated blood to the right atrium, directing it through the tricuspid valve therefore reducing the opportunity for recirculation (figure 2). It was thought that the single cannulation would lead to reduced bleeding and vascular complications and would allow for greater mobilisation,29 but this has not always been proven in practice.
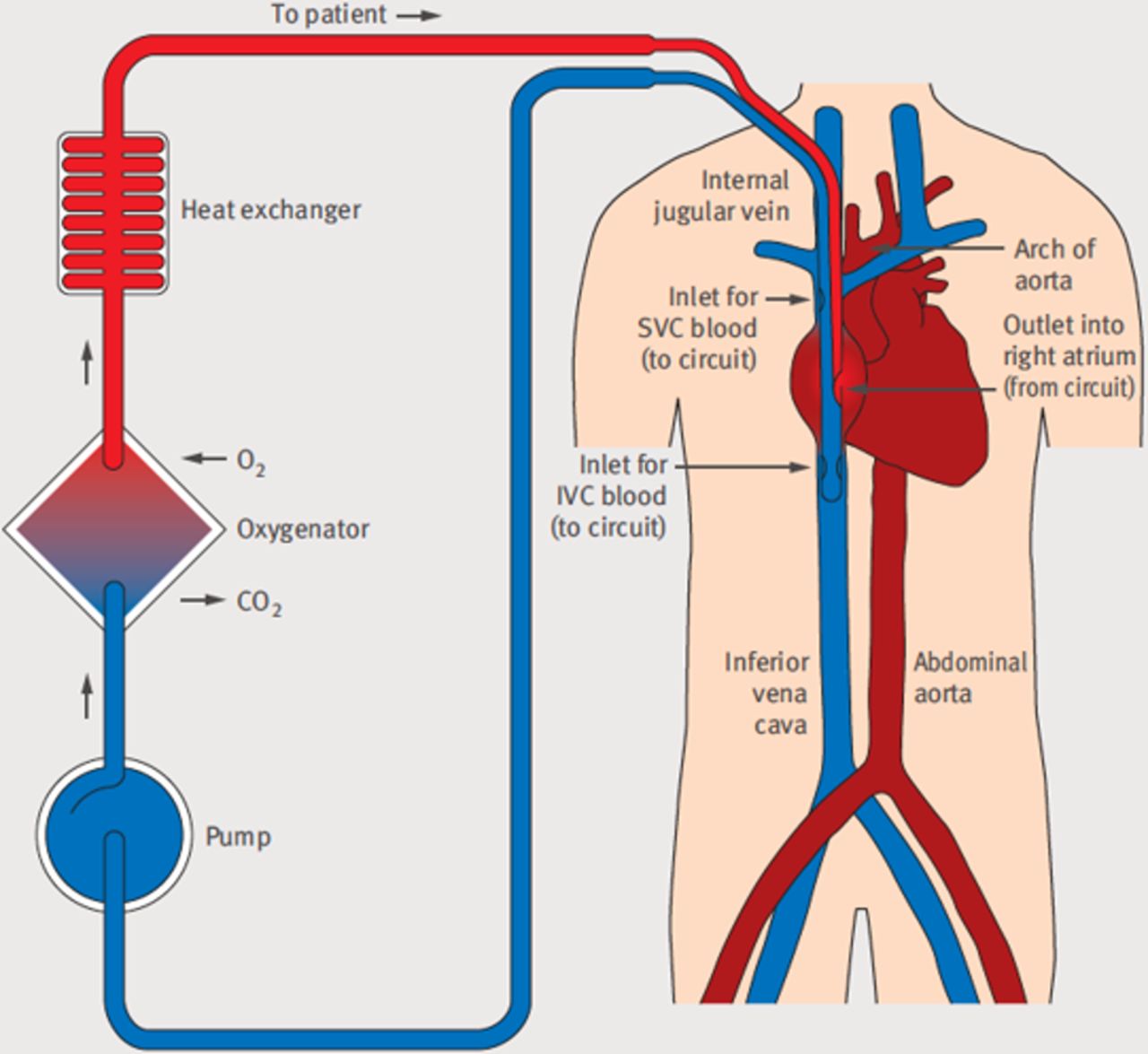
Dual lumen cannula version of veno-venous extracorporeal membrane oxygenation for respiratory failure: deoxygenated blood from both the superior and inferior venae cavae passes into one lumen of the double lumen cannula. Blood flows in tubing to a pump and on to an oxygenator and heat exchange unit, before being returned to the right atrium through the second lumen with an oxyhaemoglobin concentration approaching 100%. Here, oxygenated blood mixes with deoxygenated blood that has bypassed the double lumen cannula. This mixture of oxygenated and deoxygenated blood (oxyhaemoglobin saturation of around 80%) is pumped by the heart through the non-functioning lungs into the aorta and on to the organs and tissues of the body. Blue: intravascular deoxygenated blood; red: intravascular oxygenated blood; dark red: intravascular and intracardiac mixed oxygenated and deoxygenated blood; IVC, inferior vena cava; SVC, superior vena cava. Reproduced from Gaffney et al. 28
Veno-arterial extracorporeal membrane oxygenation
In VA-ECMO, the venous drainage cannula is inserted into the vena cavae or right atrium, either percutaneously through the femoral or internal jugular vein, or centrally (figure 3). Blood is returned to the patient through a cannula in either the ascending aorta if inserted centrally, or peripherally in the femoral or subclavian artery which can be performed percutaneously or via surgical cut-down. The common carotid artery commonly used in neonatal/paediatric VA-ECMO30 is not used in adult patients.

{kind=link}
{kind=link}
{kind=link}
Configurations of veno-venous (VV) and veno-arterial (VA) extracorporeal membrane oxygenation (ECMO) cannulation. (A) An alternative VV-ECMO cannulation; deoxygenated blood is drained from the femoral vein with oxygenated blood being returned to the right atrium. (B–D) Various VA-ECMO configurations. (B) Blood is drained from the femoral vein and returned to the femoral artery where oxygenated blood flows in a retrograde direction up along the aorta; when some residual cardiac function remains, oxygenated extracorporeal life support blood mixes with deoxygenated blood ejected from the left ventricle. (C) A cannulated carotid artery, a site often used in infants. (D) Central cannulation: transthoracic right atrial and aortic cardiopulmonary bypass cannulae. Blue: intravascular and intracardiac deoxygenated blood; red: intravascular oxygenated blood; dark red: intravascular and intracardiac mixed oxygenated and deoxygenated blood. Reproduced from Gaffney et al. 28
Central VA-ECMO uses larger cannulae and therefore can generate greater flows and therefore haemodynamic support. This is most commonly used in patients with postcardiotomy cardiac failure following any type of cardiac surgery.26
Femoral arterial cannulation is associated with three major problems: ‘differential cyanosis’ (which is also known as Harlequin syndrome, North-South syndrome or differential oxygenation), limb ischaemia and increased afterload for the left ventricle.
Differential cyanosis
Oxygenated blood is pumped retrograde through the descending aorta into the ascending aorta to perfuse the coronary arteries and cerebral vessels. However, if there is native left ventricular output there will be a ‘mixing zone’ where ejected native anterograde and reinfused retrograde blood meet. In the context of concomitant inadequate ventilation, the blood exiting the left ventricle will be relatively deoxygenated. As native cardiac function recovers the mixing zone can move distally into the descending aorta therefore resulting in the coronary and cerebral circulations receiving deoxygenated blood. Monitoring of cerebral saturations and right radial artery blood gases can be indicative of this ‘differential cyanosis’.31 Strategies to manage this include increasing ventilatory support of the lungs to improve oxygenation of the pulmonary venous blood and increasing the flow through the femoral arterial catheter with the aim of displacing the mixing zone to the ascending aorta.25 26 31 Alternatively, the ECMO configuration can be altered to veno-venoarterial, with placement of an additional reinfusion catheter typically into the internal jugular vein (but femoral venous return is also described) such that a proportion of the oxygenated blood is reinfused into the native cardiac circulation therefore, increasing oxygen saturation of ejected blood.32
Limb ischaemia
Ipsilateral ischaemic limb injury due to obstruction of distal femoral arterial blood flow which can lead to critical limb ischaemia necessitating fasciotomies or amputation can occur following femoral arterial cannulation for VA-ECMO. This can be avoided by placement of a small antegrade perfusion catheter into the superficial femoral artery to perfuse the leg distal to the primary cannula.31 Limb ischaemia can develop following arterial cannula removal due to displacement of clot developing around the cannulae.
Increased afterload
The continuous retrograde flow of blood within the ascending aorta can lead to increased afterload preventing the left ventricle from ejecting. In this situation, left ventricular distension can occur which can lead to development of pulmonary oedema and even development of intracardiac thrombus if there is no aortic valve opening.
Management of ECMO support in the context of cardiac support
Patients supported with ECMO should be managed by multidisciplinary specialists including some experienced in monitoring circuit function33–35 and others in heart failure management (table 1). The level of support provided by the ECMO system should be titrated to achieving adequate tissue perfusion—as judged by end organ function and lactate level.25
Multidisciplinary specialists involved in the management of patients on extracorporeal membrane oxygenation (ECMO)
Patients on VA-ECMO do not necessarily require sedation. Out-of-bed mobilisation is difficult for patients with a return cannula in the femoral artery but can be easily achieved for patients on all other modes of ECMO support.
Pharmacological management of the patient on VA-ECMO can be challenging, particularly initially. There will usually be a reduction in the inotropic and vasopressor requirement as gas exchange improves and intrathoracic pressures are reduced. Typically, patients will be volume overloaded with fluid accumulation within the extracellular space due to sepsis, inflammation and cardiac failure. This can be managed with diuretic therapy and fluid restriction, and haemofiltration can be a useful adjunct to ECMO.
In cases of severely impaired left ventricular function, the blood flow and associated pressure generated by VA-ECMO will increase afterload and lead to an overdistension of the left ventricle and left atrium, worsening pulmonary oedema by increasing afterload and reducing left ventricular ejection.36 This may cause myocardial injury. There is an increased risk of intraventricular thrombosis due to blood stagnating. Serial echocardiography should be performed to monitor for this complication. If identified, several strategies have been described to facilitate decompression including addition of a left ventricular vent cannula or alternative support modalities can be used such as a percutaneous ventricular assist device.37
Anticoagulation
The circuit tubing is made of a plastic which therefore necessitates therapeutic anticoagulation to prevent activation of the clotting cascade and thrombosis of the circuit, although this must be balanced with the patient’s risk of bleeding. Anticoagulant-bonding of the material aims to reduce this activation. Most commonly anticoagulation is with unfractionated heparin.24 38 It is possible to run ECMO without anticoagulation but this significantly increases the risk of thrombosis, particularly in the context of arterial cannulations used in VA ECMO. However, this may be necessary temporarily in the context of bleeding complications. To reduce the risk of bleeding, a centre in Germany reported 61 patients on VV-ECMO that were successfully managed with only prophylactic low molecular weight heparin.39
Thrombocytopaenia is a common problem for patients on ECMO due to destruction within the circuit, and regular platelet transfusions may be necessary to reduce the risk of bleeding.24 Heparin-induced thrombocytopaenia is a potential complication, requiring expert haematological input to guide management of anticoagulation.
Complications
The morbidity associated with ECMO is significant and it is this that warrants careful patient selection. The most common serious complications are thrombosis and haemorrhage.24 There are multiple factors that contribute to development of thrombosis: blood contact with foreign surfaces, blood stasis in cardiac chambers and disseminated intravascular coagulation. Consequently, patients must be therapeutically anticoagulated to prevent development of thrombosis within the circuit which can affect function of the circuit and/or embolise to the systemic circulation (in VA-ECMO). This requirement for anticoagulation—in addition to the consumption of coagulation factors and platelets—leads to the risk of haemorrhage which can occur in any organ. Bleeding often occurs at the cannulation sites.
Infective complications are important, often related to the cannulation sites and strict aseptic technique is required when handling the lines. Mechanical equipment failure is now very uncommon with modern systems but can be catastrophic.
A recent meta-analysis summarised the incidence of complications observed in patients on VA-ECMO support from 20 studies reporting on outcomes in 1866 patients (table 2).40
Complication rates of cardiac extracorporeal membrane oxygenation (modified from Cheng et al 40)
For survivors of ECMO there has been the suggestion that there is an increase in neurological deficits and respiratory morbidities. It is not known the neurodevelopmental deficits and behavioural problems observed in the paediatric population28 applies to adults but RCTs in adults have observed no between-group differences for these outcomes.6 41 As most patients recovering from severe critical illness, patients will require rehabilitation and multidisciplinary follow-up after discharge from hospital.
Outcomes
There is little doubt in the mind of clinicians that supporting with ECMO has had a significant impact on outcomes for patients with reversible respiratory and cardiac failure. However, there are no randomised controlled data demonstrating the absolute benefit of ECMO. In the use of ECMO to support cardiac function, this may be explained by the challenge of designing trials of life support that are ethically acceptable.20 Much of the evidence supporting use of ECMO therefore comes from case series, cohort studies and registry data and there remains the challenge of quantifying the number of deaths actually averted using ECMO.42 What is becoming increasingly appreciated is the importance of patient selection and timing of initiating ECMO support.
Extracorporeal Life Support Organization registry
ELSO was founded in 1989. This organisation maintains an international registry of patients who have been treated with all types of extracorporeal life support. The results of the ELSO registry are published regularly. As of July 2018, a total of 100 905 patients (including neonatal, paediatric and adult) are included in the registry.13 Overall, 68% of patients survived extracorporeal life support, with 56% surviving to hospital discharge. Outcomes for adults are summarised in table 3.
Summary of outcomes following extracorporeal membrane oxygenation (ECMO) in adults13
Patients are usually offered VA-ECMO support when at risk of imminent death and it is not surprising that the survival in this group is low. The chance of overall survival is determined by the diagnosis, state of end organ damage at the time of initiation of support and in the case of non-recovery the potential for transplantation or more permanent support (eg, ventricular assist devices). Patients supported postcardiotomy43 or as part of extended CPR44 have the worst survival.
ECMO outcome predictions scores
Data from the ELSO registry have been used to create outcome prediction scores to allow estimation of likelihood of survival in patients selected for ECMO in different settings.45 46
Conclusion
ECMO is an advanced form of cardiorespiratory support which has become commonplace in the ICU environment. A multidisciplinary team of specialists with experience managing patients on ECMO support is essential to achieving the excellent outcomes that are now achieved. The complications are significant, and careful patient selection is an important part of the current success of ECMO services. There is a lack of evidence demonstrating the clinical benefit of the use of ECMO and this should be the focus of future studies, helping to understand which patients are most likely to recover on ECMO support.
Key points
Extracorporeal membrane oxygenation (ECMO) is an advanced form of cardiorespiratory support based on cardiopulmonary bypass technology.
Veno-venous (VV) ECMO is used to support patients with acute respiratory failure with refractory hypoxaemia or hypercapnia despite optimal ventilation.
Veno-arterial (VA) ECMO is used to support patients with cardiogenic shock that is refractory to maximal therapy.
ECMO should be reserved for patients with reversible pathology, or who are potential transplant candidates.
Patients supported with ECMO should be managed by experienced multidisciplinary specialists.
Therapeutic anticoagulation is necessitated to minimise the risk of thrombosis, but predisposes to bleeding.
Patient outcomes are reported by the Extracorporeal Life Support Organization registry. In adults, survival to discharge for respiratory ECMO is 59% and for cardiac ECMO is 42%.
CME credits for Education in Heart
Education in Heart articles are accredited for CME by various providers. To answer the accompanying multiple choice questions (MCQs) and obtain your credits, click on the ‘Take the Test’ link on the online version of the article. The MCQs are hosted on BMJ Learning. All users must complete a one-time registration on BMJ Learning and subsequently log in on every visit using their username and password to access modules and their CME record. Accreditation is only valid for 2 years from the date of publication. Printable CME certificates are available to users that achieve the minimum pass mark.
References
Footnotes
Contributors The manuscript was written by JA and AV. Both authors reviewed and prepared the final manuscript for submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Patient consent for publication Not required.