


Abstract
Objectives: To study age specific rates of hepatitis B virus (HBV) carriage in the eastern region of Saudi Arabia following a 24 year immunization program.
Methods: Hepatitis B surveillance data between January 2004 and December 2013 were analyzed in a retrospective study, which included 24,504,914 patients. Seropositive cases of hepatitis B were reported by laboratory personnel as part of various investigations. Hepatitis B cases including acute and chronic carriers were identified upon serological positivity of hepatitis B surface antigen (HBsAg).
Results: The study shows that the overall prevalence rate decreased from 18.8 to 9.9/100,000 population between 2004 and 2013 (p=0.01). It was also found that the prevalence rate increased with age. For instance, the highest prevalence of hepatitis B was seen among patients >15 years of age and the lowest was seen among children <15 years of age. Over the period, the prevalence rate decreased in all age groups with the greatest decline among the age groups <4 years old. However, this was statistically insignificant (p>0.05). Another significant reduction in the prevalence rate occurred among age groups 5-14 years old (p=0.00). An insignificant decrease in the rate by 43% was also seen among older patients of 15-44 years old and 35% in >45 years old. The overall prevalence of hepatitis B is significantly higher in men than in women (p=0.00).
Conclusion: There is a particular decreased trend in the prevalence of HBV infection in different age groups over a decade of surveillance following more than 20 years of the universal HBV vaccination program.
Hepatitis B virus (HBV) is a public health concern world-wide and a major cause of chronic hepatitis, liver cirrhosis, and hepatocellular carcinoma. The burden of HBV infection varies geographically and depends on the different modes of transmission and the age at the infection, which determines the probability of progression to chronic infection.1,2 Several studies3-9 reported the prevalence of HBV in Saudi Arabia among the general public, school students, blood donors, health care workers, and pregnant women. Several studies have shown that HBV infection in Saudi Arabia is acquired mainly through horizontal and vertical transmission similar to what is observed in other endemic countries.10,11 It has been reported that 5-10% of the population were infected with HBV.12 However, despite a significant decline in the prevalence of HBV infection in Saudi Arabia, the disease continues to cause significant morbidity and mortality and imposes a great burden on the country’s health care system.12 Compared with other parts of Saudi Arabia, a higher prevalence of hepatitis B surface antigen (HBsAg) was found in the eastern region of the country.13 Since October 1989, the HBV vaccine has been integrated into the children’s extended program of immunization.13 Hepatitis B surveillance in Saudi Arabia was especially conducted to measure disease frequencies, direct prevention and control activities, and to evaluate the impact of these activities. Furthermore, a periodic and regular evaluation of surveillance data for quality, completeness, and timeliness was also implemented. This resulted in a marked decline in HBsAg seroprevalence, which was reported several times.14,15 Most of the previous reports16 on HBV infection in Saudi Arabia were based on prevalence studies, while very few were concerned with the actual disease risk in the community, or the effectiveness of immunization programs. Reports on the age specific prevalence of HBV especially in the eastern region of Saudi Arabia are very much lacking. Most of the previously mentioned studies have investigated the prevalence of HBV at country level. However, this study is the first one to assess the impact of a long term strict control measures on the rate of HBV carriage in the eastern region of Saudi Arabia, which was found to have the second highest prevalence in the country.17 The main objective of this study is to describe the trend in prevalence of HBV infection in 14 sectors affiliated to the eastern region of Saudi Arabia over a decade of surveillance (2004-2013) following the introduction of a vaccination program in 1989.
Methods
The primary goals of conducting surveillance for hepatitis B are to directly prevent and control activities for these diseases and to evaluate the impact of these activities.
The Eastern Province is the biggest province in Saudi Arabia. It borders the Arabian Gulf, Iraq, Kuwait, Oman, Qatar, the United Arab Emirates, and Yemen. In 2012 the population of the eastern region was 4,414,278, which includes 3,065,883 Saudi nationals and 1,348,395 expatriates mainly from other Arab and Asian countries with an annual growth rate of 3.19 between 2004 and 2010.18,19 Hepatitis B virus diagnostic reports were collected retrospectively in a cross-section study, which included 24,504,914 patients between 2004 and 2013 from 14 sectors in the eastern region involving participants visiting health facilities of the study area. All recorded cases indicated the unique medical record number of the patients to avoid duplication. Seropositive cases of hepatitis B were reported by a laboratory personnel as part of the investigations, which included medical care of clinically compatible illness, routine screening of blood donors, antenatal care, prenuptial tests, HBV-infected patients’ contacts, prisoners, intravenous drug users, patients with other sexually transmitted infections, and expatriates doing pre-employment tests.
Furthermore, HBV cases, including acute and chronic carriers, were identified upon serological positivity of HBsAg. The HBV markers were detected by standard enzyme immunosorbent assay (ELISA) using commercial kits for HBsAg according to manufacturers’ instructions. Any subject with positive HBsAg confirmed by a neutralization test was considered to be HBV-infected. However, ethical approval for the study was obtained from the Ethics Committee of Prince Sultan Military College of Health Sciences, Dhahran, Saudi Arabia. All subjects were assured of confidentiality of personal data.
According to the Ministry of Health Annual statistical books 2004-2013,18 the annual population of the eastern region during the surveillance period ranged from 2,113,533 in 2004 to 2,941,236 in 2011. The distribution of the population by age groups was calculated according to the age structure of the population reported by the 2007 census of Saudi Arabia. This was estimated as 2.3% for <1, 8.2% for 1-4, 20.4% for 5-14, 55.9% for 15-44, and 13.2% for and >45 years.18 Gender distributions was estimated according to the 2009 population census of Saudi Arabia, which reported a male to female ratio of 1.25: 1.19
Statistical analysis
For the purpose of this report, hepatitis B surveillance data between January 2004 and December 2013 were analyzed. Prevalence trends refer to rates over time of diagnosed seropositive cases of hepatitis B. The carriage rate for a certain yea, or demographic group (gender, age group) was calculated by dividing the number of reported seropositive cases for hepatitis B for that year, or demographic group by the corresponding estimated population for that year, or demographic group, then multiplied to give the rate per 100,000. All data were analyzed using the Statistical Package for Social Sciences version 20.0 (SPSS Inc., Chicago, IL, USA) to calculate the odds ratios (OR) and the respective 95% confidence interval (CI) for the decline in hepatitis B prevalence between 2004 and 2013. We used the 2004 prevalence for reference to calculate the OR and p-values compared with this year. Data were analyzed using univariate analysis. We used 5% (p<0.05) as a level of significance.
Results
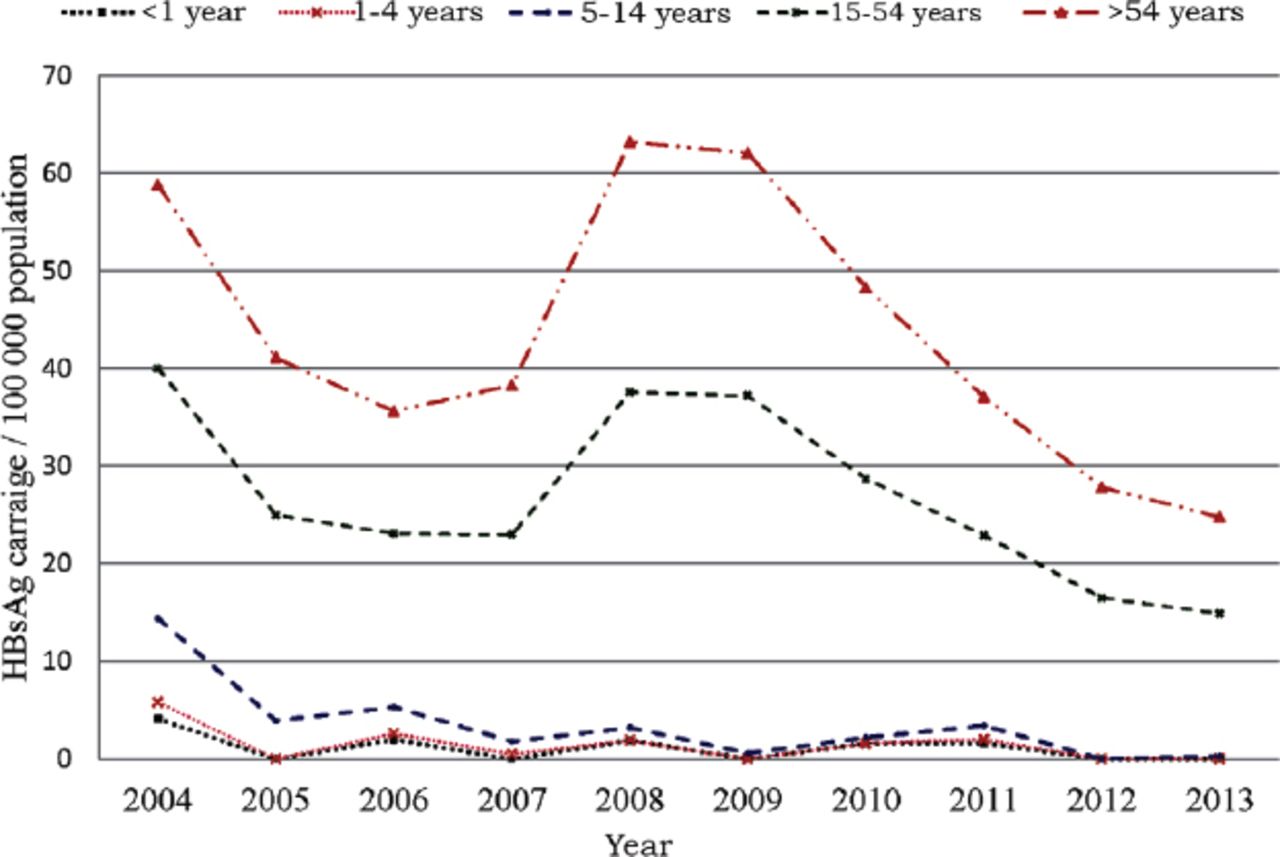
The estimated number of 4053 HBV infections by age groups and population at risk in the eastern region of Saudi Arabia during 2004-2013 are shown in Table 1. Tables 2 & 3 summarize the prevalence rate per 100 000 population (R/105) and the OR with the 95% CI, and the p-value among younger and older age groups. The highest prevalence of hepatitis B was seen among persons >44 years of age and the lowest among children <15 years of age. The overall prevalence has decreased from 18.8 in 2004 to 9.9% in 2013 (Table 3). During the surveillance period, the prevalence decreased in all age groups with the greatest decline of almost 100% at the age groups <1 and 1-4 years, although statistically insignificant. A significant reduction of 96.5% of the prevalence occurred among age groups 5-14 years. A less dramatic, statistically insignificant (p>0.05) decrease in the prevalence of 43% was seen among older persons of 15-44 and 35% in >45 years old. The average prevalence of HBV infection in the eastern region during the 10 year surveillance period ranged from 0.3 cases per 100 000 population for the age group 1-4 years to 25 cases per 100 000 population for the age group >45 years. The total number of HBV infections among patients <14 years old was 106 cases compared with 3947 cases detected among those >24 years old. There was a clear decline in the prevalence among all 3 pediatric age groups, namely infants <1 year of age, children 1-4 years of age, and children 5-14 years of age, although there was no noticeable decline in the overall prevalence (Figure 1). From 2004 to 2013, 4053 cases of HBV infection (HBsAg-positive) were estimated according to the data collected from 14 sectors affiliated to the eastern region of Saudi Arabia, of whom 2665 (65.7%) cases were males and 1388 (34.2%) were females. Prevalence rates among males were 10.6 per 100 000 and females were 6.0 per 100 000 (Table 4).
Hepatitis B surface antigen virus cases by age groups in the Eastern Province of Saudi Arabia during 2004-2013 and the population at risk between parentheses.
Hepatitis B surface antigen virus rate per 100 000 (R/105) and the odds ratio (OR) with the 95% confidence interval (CI) and P-value among younger age groups.
Hepatitis B surface antigen virus rate per 100 000 (R/105) and the odds ratio (OR) with the 95% confidence interval (CI) and P-value among older age groups.

Yearly hepatitis B surface antigen (HBsAg) virus rate/100 000 of hepatitis B among all age groups.
Hepatitis B surface antigen virus of hepatitis B virus per 100 000 population and number of infections by gender and the odds ratio and the 95% confidence interval (CI) at the different age groups.
In the <1 year age group, the prevalence among females is insignificantly higher than males (p=0.59). In the 1-4 years old age group, although slightly higher, it was not statistically significant (p=0.78). At 5-14 years, the prevalence was higher in males and statistically significant (p=0.00). For the older age groups >15 years old, the prevalence among males was noticeably higher than females and statistically significant (p=0.00).
Discussion
The current study showed the trend in prevalence of HBV infection in different age groups over a decade of surveillance following 24 years of the universal HBV vaccination program. The age group that included children and adolescents <15 years showed the greatest HBV prevalence decline, mainly due to the universal infant/child immunization program started in 1989 in Saudi Arabia.
The average prevalence of HBV infection during 2004-2013 among children was 1.1, 0.3, and 2.1/100 000 population, for the age groups of <1, 1-4, and 5-14. The relatively higher prevalence among children <1 year than the subsequent age group of 1-4 year may indicate that a sporadic vertical transmission is taking place. The study also indicated that horizontal childhood HBV transmission is very low in children, and suggested that schools may not form any risk of horizontal transmission of HBV. Similar findings were detected in very low-prevalence countries.20 The prevalence of HBV was more than 20-fold higher in those who were aged >15 years compared with those who were <15 years old (annual average prevalence of 24.2 and 1.2 per 100, 000 population).
Prior to the introduction of vaccinations in 1989, the overall prevalence of HBsAg of 6.7% was steady in all age groups, and the highest prevalence was seen in children between 1-3 years in the study area.21 The overall prevalence of hepatitis B in the eastern region declined by 47.34% from 18.8 to 9.9 per 100,000 population between 2004 and 2013.
The total number of cases detected between 1990-1999, a decade prior to our analysis, was 6101 hepatitis B cases compared with 4053 detected between 2004 and 2013, namely, a 33.57% reduction.13 The highest annual prevalence of 25.6/100,000 population reported in 2008 and 24.9/100,000 in 2009 was less than the estimated average annual prevalence of 46.0 and 53.2/100,000 population for HBV during the same period, possibly due to a population size estimate of those studies.16 The reduction in HBV prevalence in Saudi Arabia may be attributed to several measures implemented since 1989.13 However, the foremost of these measures is the vaccination of infants beginning at birth. Vaccination coverage as reported monthly by the Ministry of Health was >95.5% since its commencement.18 Other preventive measures include routine screening of all pregnant women for HBsAg for preventing perinatal infection, provision of immunoprophylaxis to infants born to HBsAg positive women, and routine vaccination of previously unvaccinated children and adolescents, although evidence for the declining protective effect of the vaccine in late adolescence has been proved.10,11,13 The vaccination of previously unvaccinated adults at increased risk for infection such as healthcare workers, dialysis patients, household contacts, and gender partners of persons with chronic HBV infection and others have also contributed to the incidence reduction. In addition, health education, routine screening of blood and organ donors for HBsAg, proper sterilization of surgical and dental equipment, and routine screening of high-risk subjects were implemented in HBV prevention strategy.22 Consequently, awareness for the public to practice good hygiene in barbers shops and traditional therapy settings is also important in Saudi Arabia. Routine pre-employment screening for HBV infection of expatriates who wish to be employed in Saudi Arabia was also implemented. The higher prevalence of HBV seroprevalence among adults in the current study, which accounts for 97.4% of the total cases between 2004-2013 may partly be due to intensive observations during prenuptial screening, blood donors, and the recruitment of new military or civilian employees. It is estimated that 50% of the Saudi population is less than 24 years of age.19 Accordingly, it could be assumed, therefore, that at least 50% of the Saudi population has been vaccinated for HBV either at birth or as an entry requirement for primary school. As such, this particular group would have an insignificant prevalence of infection as indicated in this study.
In general, the overall prevalence of hepatitis B is significantly higher in men than in women. In the age group <1 year, the prevalence among females is insignificantly higher than males (p=0.59). At the age of 1-4 years, although slightly higher, it was not statistically significant (p=0.79). At 5-14 years, the prevalence was higher in males but again statistically insignificant. For the older age groups, above 15 years, the prevalence among males was markedly higher than females, which is statistically very significant (p=0.00). The OR of female to male in this study was 1:2.40, and statistically insignificant. In a previous report, the prevalence of HBV seropositivity stratified by gender showed a higher prevalence of 123.0 cases per 100,000 population in males compared with 85.5 per 100,000 population in females.16 Nevertheless, the impact of gender on hepatitis B has been reported also in China.22
Long time implementation of universal infant vaccination against HBV in other endemic areas has resulted not only in decreasing the disease prevalence, but also in the reduction of liver cancer.23 Evidence of the decrease in the prevalence of HBV-associated HCC in Saudi Arabia has been previously demonstrated.24
In conclusion, the prevalence of HBV infection in Saudi Arabia has markedly decreased among children as a result of the universal childhood HBV vaccination program that was implemented in 1989. It is expected that the prevalence of HBV infection and its complications (cirrhosis and hepatocellular carcinoma) will also greatly decrease among adults in the near future as the vaccinated individuals grow older.25 Although the occurrence of hepatitis B among children below one year of age indicates an incidence of new cases, a prospective study is required in order to determine the actual incidence of hepatitis B in the area. Another limitation of this study is that it is a hospital based surveillance that may not reflect the real population incidence.
Ethical Consent
All manuscripts reporting the results of experimental investigations involving human subjects should include a statement confirming that informed consent was obtained from each subject or subject’s guardian, after receiving approval of the experimental protocol by a local human ethics committee, or institutional review board. When reporting experiments on animals, authors should indicate whether the institutional and national guide for the care and use of laboratory animals was followed.
Acknowledgment
This work is fully supported by the Prince Sultan Military College of Health Sciences, Dhahran, Saudi Arabia. The data presented in this manuscript were generously provided by the Eastern Region Health Affairs Directorate to whom we are greatly indebted. We wish to thank Mr. Abdul T. Baker and Mr. Charles Janicki, of the English Department for assisting in the proof-reading of the manuscript.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 17, 2016.
- Accepted June 6, 2016.
- Copyright: © Hellenic Society of Gastroenterology
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.