


Abstract
Objectives: To assess knowledge and attitudes about do not resuscitate (DNR) among patients and their relatives visiting outpatient clinics at King Abdulaziz University Hospital (KAUH), Jeddah, Kingdom of Saudi Arabia.
Methods: A cross-sectional study conducted between March and April 2018 with a self-administered questionnaire among patients and their relatives visiting outpatient clinics at KAUH. A systematic random selection of individuals every other day.
Results: The questionnaire was filled by 400 participants. Fifty-four percent were patients’ relatives, and approximately 60% were female. Out of 105 (26.3%) who were familiar with the DNR term, 44.8% chose the correct definition, 5.2% had previous experience with the DNR term, and 34.3% of them had DNR-related knowledge from social media. Out of the 400 participants, 169 (42.3%) disagreed with DNR. The majority of responders did not know if there is DNR policy or fatwa (a legal opinion on the point of Islamic law).
Conclusion: There is a lack of knowledge regarding DNR among participants.
Allowing natural death is the most recent term of the do-not-resuscitate (DNR) order, although most hospitals still use the traditional DNR term.1 Do-not-resuscitate is a clinical order written by a doctor indicates that cardiopulmonary resuscitation (CPR) should not be initiated if a patient is found in cardiac or respiratory arrest. Do-not-resuscitate orders do not provide instructions for treatment.2 Do-not-resuscitate is a common practice, a crucial medico-legal aspect, and a broad area of debates. Since the 1980’s in the United States of America (USA), the DNR policies and guidelines have been perceived as patient autonomy.3 Thus, before writing the DNR order, the physicians should discuss it with the patient or his/her surrogate and respect his/her decision, whether it is acceptance or refusal.3 The DNR policies and guidelines in the Kingdom of Saudi Arabia (KSA) differ from those in the United States of America due to the fact that Saudi policies depend on many religious factors. Fatwas (a legal opinion on the point of Islamic law) are a unique term for the Islamic countries and are considered an approved source for policies and law. The Permanent Committee for Scholarly Research and Ifta’ published a Fatwa in 1988/1409 AH number 12086 about the basis of DNR policy. This policy clearly states: “If 3 knowledgeable and trustworthy consultants decide that resuscitation will be futile, DNR order will be established regardless of the patient and family wishes”.4 For our regional guidelines, the DNR was established with the aim of giving the DNR patient all treatments and interventions, in addition to comfort and dignity without providing CPR.4 In KSA, the Ministry of Health (MOH) started an on-going project aims for establishing a national policy for DNR to be applied in all hospitals.5 Few studied were carried out focusing on knowledge and attitude toward DNR that showed lack of knowledge with minimal empowerment of patients in DNR decision making.6,7
Patients and their families have the right to know everything they might undergo, including DNR orders. During daily practice, the researchers noticed a lack of knowledge regarding DNR along with insufficient data on DNR in KSA. We believe it is an important issue needs to be studied. We aimed to assess the knowledge and attitude about DNR among patients and their relatives visiting the outpatient clinics at KAUH, Jeddah, KSA.
Methods
A cross-sectional study was conducted in KAUH between March and April 2018 with a self-administered questionnaire among patients and their relatives who were visiting outpatient clinics at KAUH including the following clinics: internal medicine; family medicine; hematology; pediatrics; obstetrics and gynecology; general surgery; otorhinolaryngology; orthopedics; anesthesia; ophthalmology; and psychiatry. The study was approved by the Ethical Committee at KAUH, Jeddah, KSA, and a written consent was taken from all participants. A sample size of 385 was calculated using the equation:
with a confidence interval (CI) 95%, absolute error (d) of 0.05, and z-score of 1.96. The expected proportion in the population based on the previous study conducted in Riyadh7 (p) was 50%.
The inclusion criteria were all outpatient visitors at KAUH, Jeddah, KSA, and exclusion criteria were individuals aged less than 18 years old and above 70 years old and handicap. After analysis of the data, all samples have been included, and non were excluded.
Data collected by the co-authors using a systematic random selection of individuals chosen every other day (Sunday, Tuesday, Thursday) and distribution of the questionnaire for every other patient from outpatient clinics.
The questionnaire was taken from previously validated questionnaires based on a study carried out in Jeddah, KSA, among interns and residents and in Canada in outpatient clinics.6,8 Three expert consultants in the field reviewed the questionnaire to assess its validity. Back and forth translation was used to translate it from the English to the Arabic language at an authoritative translation office.
The questionnaire was composed of 4 parts: the first part consisted of demographic data; the second part has 2 sections A and B. Section A was answered only by individuals who had heard about DNR; it assessed their ability to define DNR correctly, from where/whom they had heard the term and their previous experience with the DNR term. Section B started with a statement of the correct definition of DNR (DNR is an order made by the physician and reported to all healthcare providers that if a patient’s heart or breathing stops not to perform CPR because it is futile, regardless of the age of the patient), followed by 6 questions aimed to evaluate a subject’s viewpoint toward DNR orders and decision making along with determining the subject’s knowledge regarding the presence of DNR policy and fatwa in KSA; the third part, factors to be considered in decision making, such as limited intensive care unit (ICU) state, the risk of vegetative state, religious concerns, legal concerns, patient dignity, efficient use of medical resources and cost reduction; the fourth part was the degree of agreement based on a 5-point scale for the following statements: a) assessed conservative management for DNR labeled patients, b) withdrawal of life-sustaining machines, c) organ donation, and d) whether they find it stressful to discuss DNR orders.6,8
The Statistical Package for Social Sciences (SPSS) version 21 (IBM Corp., Armonk, NY, USA) was used to analyze the data. Demographic characteristics were summarized using frequency tables. All comparisons were made using the Chi-squared test and crosstab. A p<0.05 was considered statistically significant.
Results
Five-hundred questionnaire were distributed, 400 participants completed the questionnaire with response rate of 80%. Fifty-four percent of them were patients’ relatives, and approximately 60% were female (Table 1). As the main objective of our research was assessing participants’ knowledge and attitude (Table 2).
Demographic data of participants (N=400).
Knowledge and attitude.
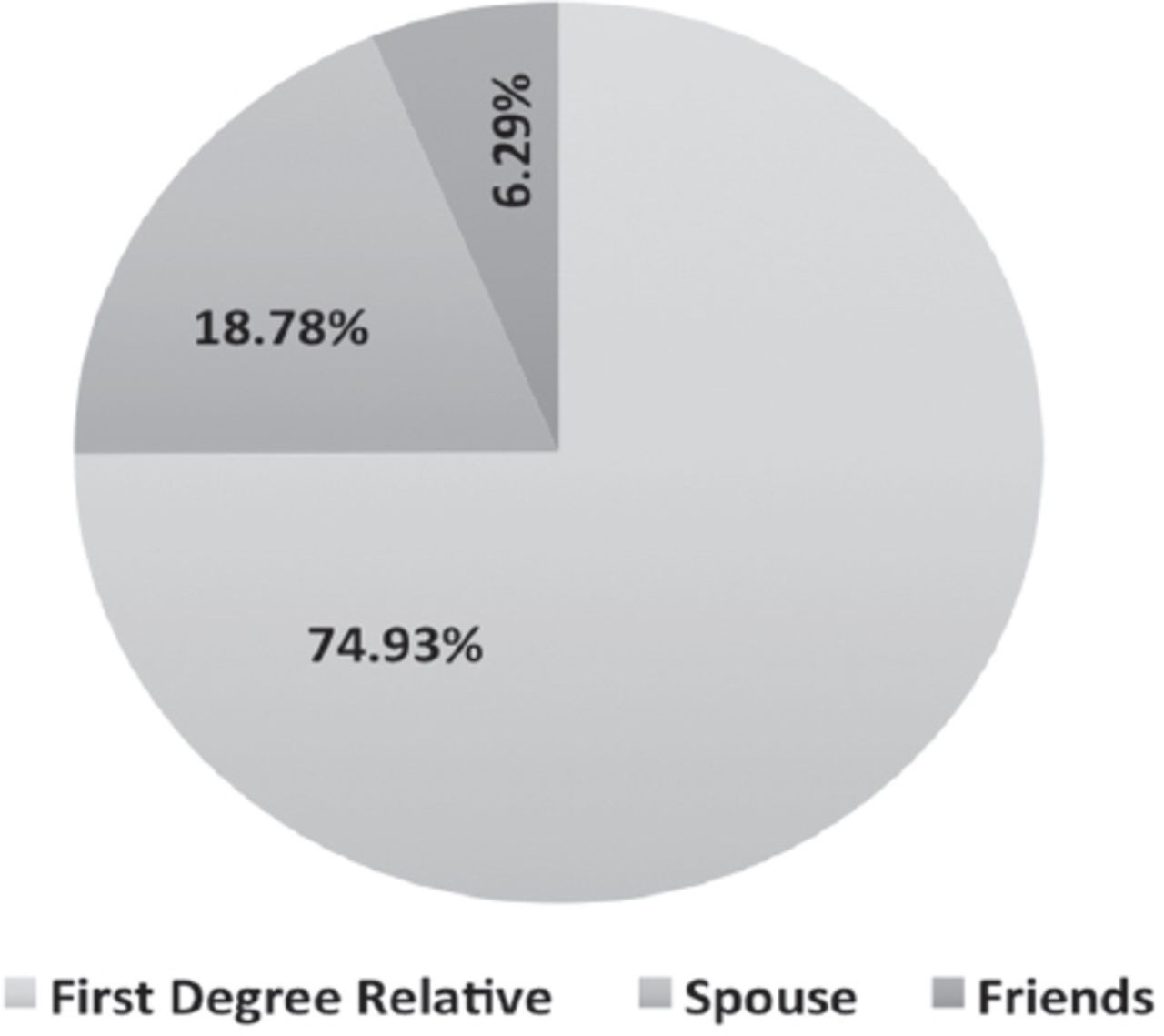
Out of 400 participants, only 105 (26.2%) were familiar with the DNR term. Participants with higher educational levels were more familiar with DNR term (p=0.05). However, there were no significant differences among age (p=0.54), gender (p=0.38), and responder status (p=0.49) (whether patient or relative). We assessed the knowledge of our responders about DNR definition. Out of the 105 who heard about the DNR term, only 47 (44.7%), were able to choose the correct one. Regarding their source of DNR-related knowledge, 34.3% gained it from social media (Figure 1). Regarding the experience of DNR, 16 (15.2%) out of 105 had a previous experience. The representation of with whom the experience had occurred is shown in Figure 2.
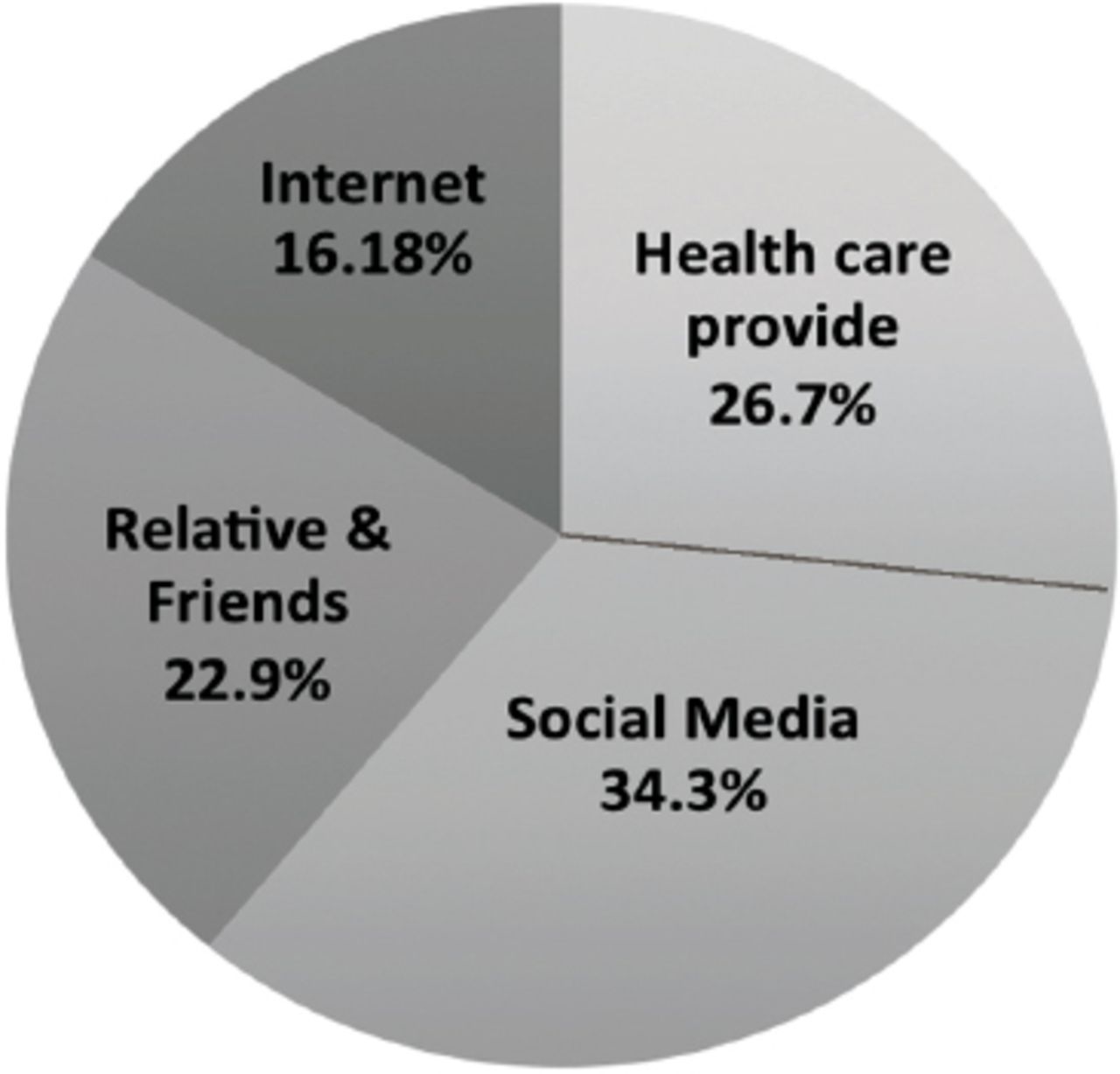
Source of knowledge about do no resuscitate (DNR) (n=105).

Do no resuscitate (DNR) experience case distribution (n=105).
As for the degree of agreement with DNR, we excluded the illiterate group due to its very small number and to avoid insignificant statistical results. Less than half (41.5%) of our sample disagreed with the DNR with a statistically significant association with educational level; p=0.02 (Table 3). On the other hand, there was no association with age (p=0.19), gender (p=0.06), occupation (p=0.22), and responders (p=0.75).
Relationship between agreement with do-not-resuscitate and educational level.
The majority of responders chose physicians as the one responsible for DNR decision making. There’s a significant difference among the age group. No significant differences were observed with responders (p=0.91) (patient, relative) and gender (p=0.38) (Table 4).
Do-not-resuscitate decision involvement among the age group.
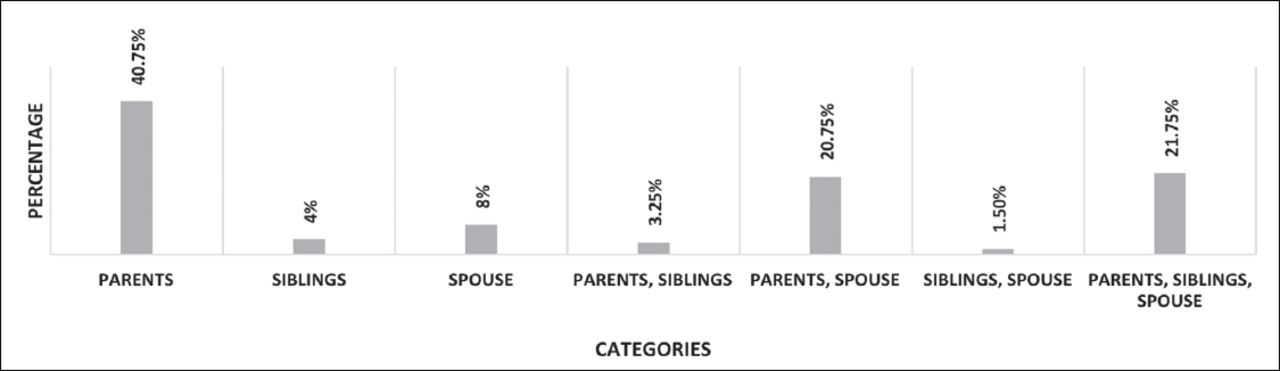
Figure 3 represents the responders’ view of the point concerning “who has the right to know about DNR decision?”. One-hundred and sixty-three (40.7%) of the responders chose their parents as the person who should be informed about their DNR status. Regarding the patient’s right whether to reject or accept the DNR order, no significant association was found with responder status (p=0.43) (patient, relative), gender (p=0.61), and age (p=0.86). Participants were asked about their knowledge concerning the presence of a clear policy and fatwa about DNR in KSA. The majority of responders did not know if there was a policy (69.5%) or a fatwa (89.8%) regarding DNR.

Having the right to know do not resuscitate (DNR) descision (N=400).
We assessed the contributors’ point of view regarding 6 different factors that should be considered while making the DNR decision. The most important factors were religious concerns (81%), followed by the risk of vegetative state (Table 5).
Do-not-resuscitate decision making related factors.
The responders were asked about their opinion in 5 different statements about DNR patients. Surprisingly, around half of the participants agreed on keeping the patient unaware of their DNR status (Table 6).
Participants attitude toward do-not-resuscitate (DNR).
Discussion
In this study, we aimed to assess knowledge and attitudes toward DNR among patients and their relatives visiting the outpatient clinics at KAUH, Jeddah, KSA. Our study found a small proportion of the participants (26.3%) were familiar with the DNR term in contrast to the findings of previous studies in which most of the responders (80%, 75%) had heard about the term.6,7 This difference may be related to their previous experience with DNR decisions (38%) in a study that was carried out in Canada in comparison to our sample in which only 15.2% had been previously involved in DNR decisions or knew about its relationship to their healthcare system that encourages discussion about the DNR term.6 In addition, the majority of responders (62%) in Riyadh, KSA, study were with higher educational levels. Furthermore, this discrepancy in findings may indicate a true lack of knowledge about the importance of the topic in our community.
Only 44.8% of our participants were capable of choosing the correct definition. This finding was similar to Riyadh, KSA, study (50.4%).7 When it comes to the source of DNR knowledge, 34.3% of participants had heard the term DNR from social media (the highest percentage) followed by healthcare providers (26.7%). In regard to the rule of social media, Bahkali et al,9 supports the effect of social media on education where they studied the level of awareness among Twitter’s female followers concerning their health, and their results demonstrated a noticeable improvement in the females’ level of awareness. Healthcare providers should be the primary source of knowledge for DNR. However, many researchers had studied the barriers of discussing DNR with patients or their families and found that inadequate training and lack of time were the commonest, along with other causes.5,10,11 Unfortunately, 28.8% of our participants agreed on the DNR concept, while 42.3% disagreed. This finding is maybe due to the complexity of the topic and its relation to several legal and religious concerns. Out of the 42.3% who disagreed group, around half of them were graduate and postgraduate, this could be due to emotion rather than scientific disagreement. The majority of our sample (72%) preferred to involve their physician in decision making because they may believe that the physician knows the best for the patient. This finding was similar to Canada research, where 86% chose their physician, while in our study involving of family members in decision making was only 21.8% compared to 72% in Canada.6 This may be due to the fact that in Canada research the participants could choose more than one choice. Forty percent of our participants tend to inform their parents of their decision in agreement with Al Sheef et al,7 (51.7%) but unlike Robinson et al,6 who showed that spouses (34%) and other family members (30%) were the most common ones to be notified. This was possibly related to religious and cultural differences. Most of our participants did not know about the existence of a clear policy (69.5%) or a fatwa (89.8%) regarding the DNR. The result is not surprising as only around half of interns and residents knew about the presence of a DNR policy or the fatwa.8 Regarding the factors to be considered in decision making, religious concerns (81%), risk of vegetative status (78%), and patient dignity (75%). These findings are consistent with 2 studies carried out among interns and residents in Jeddah, KSA, and a multicenter survey was carried out among physicians in KSA.8,12 Our participants showed positive attitudes toward organ donation and conservative approach with DNR patients; which reflects embedded Islamic and cultural values. On the other hand, participants showed unfavorable attitude toward patient autonomy as only 36.3% of them disagreed upon keeping the patient ignorant of their DNR status. Additionally, 66.6% of participants considered DNR decision as a stressful topic, which was an incompatible result with the study carried out in Canada (16%).6 Religious concerns and lack of knowledge might be the causes of the variations between the 2 samples.
Study limitations
Do-not-resuscitate was poorly understood by the responders as it involves a religious and cultural aspects that may affect their perspective. There are only a few studies regarding DNR; therefore, there was limited number of studies to compare our results. As for our findings in this research, we found significant lack of knowledge about DNR in our society; especially among lower educational levels. Those who knew about it, had their knowledge from social media.
In conclusion, our study can be utilized for paying more attention to DNR and its related issues. Our research can be considered as the beginning of more DNR related researches, where the focus could be directed to the patients, their families, and health care providers who are dealing mostly with DNR; and a significant effort should be directed to those of lower educational levels. We also recommend the implication of these researches into actions that could potentially lead to raising the awareness and knowledge. Nowadays, social media is one of the most important methods of spreading awareness about different topics in our society, including DNR.
Acknowledgment
The authors gratefully acknowledge American Manuscript Editors (https://americanmanuscripteditors.com/) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received July 11, 2019.
- Accepted November 22, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.