


Abstract
Objectives: To compare carotid endarterectomy patch angioplasty (p-CEA) with eversion carotid endarterectomy (e-CEA) and associated risks of early cardio-cerebrovascular complications.
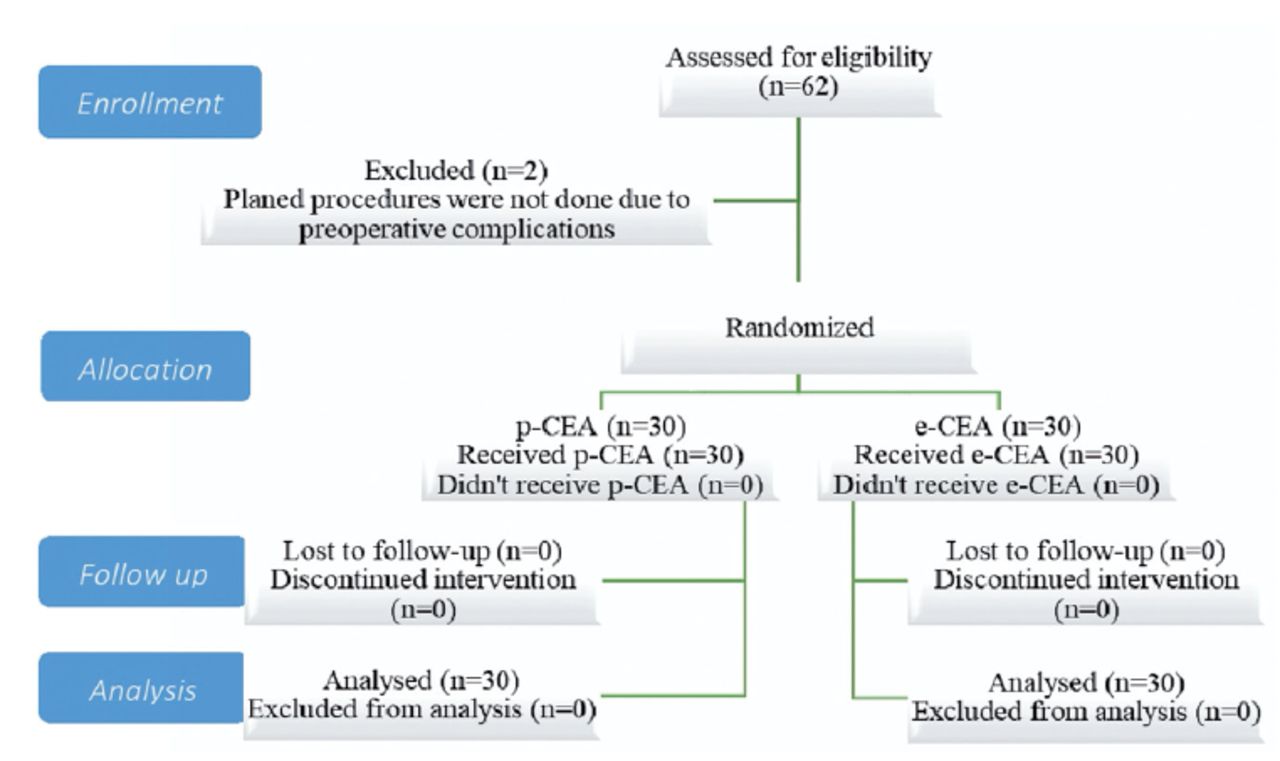
Methods: The study was a prospective randomized single-blind trial, monocentric, clinically applicable, descriptive analytical and comparative. From June 2021 to June 2023, 62 consecutive patients with symptomatic and asymptomatic stenosis of the internal carotid artery, admitted to our department and randomized into two groups: carotid endarterectomy with patch angioplasty and eversion carotid endarterectomy. Follow-up for 30 days after surgery.
Results: During surgery e-CEA, 70% patients had an arrhythmia, and 24 hours after 66.7%, seven days after 46.7% and month after 13.3%. During surgery p-CEA, 33.3% patients had an arrhythmia, 24 hours later 33.3%, 7 days after 13.3% and 30 days after 13.3% patients. Statistically significant difference observed during surgery (Fishers p=0.004). One day after the surgery rate of patients with arrhythmia that were treated e-CEA has decreased, but it was still higher than after p-CEA (Fishers p=0.010).
Conclusion: The frequency and categorization of postoperative cardiac arrhythmias after eversion carotid endarterectomy, the clinical implications of various postoperative heart rhythm disturbances and their long-term effects on patients need to be further investigate through sufficiently powered randomized controlled studies
Carotid endarterectomy (CEA) is a corner stone of primary and secondary prevention but it has many discrepancies, keys of the outcomes are in the details and based on clinical guidelines, randomized controlled trials (RCT), clinical and observational retrospective trials.1-5
Many variables can determine outcome of CEA such as local or regional anesthesia, routine or selective shunt, brain function monitoring, routine patch and completion radiological diagnostics. RCT shows that patch versus (vs) primary closure and eversion vs primary closure in patients undergoing standard CEA has better and more desired results, including early and late complications (stroke, restenosis).6-8
We should not ignore impact on carotid body (baroreceptor and chemoreceptor) sensitivity and possible early and late consequences.9 Results that show no influence in any way to function of carotid body has limitation due to study design (exclusion criteria etc) and we can only conclude that findings can be apply only to limited group of patients.10
The aim of this study was to compare patch angioplasty CEA (p-CEA) with eversion CEA (e-CEA) and the associated risks of early cardio-cerebrovascular complications including heart rhythm disorder. This prospective randomized controlled trial was a single blinded, monocentric, clinically applicable, descriptively analytical, and comparable study. Patients were divided into two randomized groups: one that received p-CEA and one that received e-CEA.
Methods
This prospective monocentric randomized controlled trial was approved by the Scientific Ethics Committee of Cantonal Hospital Zenica (IRB 00-03-35-247-3/21). We used findings on all available relevant medical databases to guide our research. Followed procedures were in accordance with the ethical standards of the responsible committee and with the Helsinki Declaration of 1975, as revised in 2013.
The study examined 62 consecutive patients admitted to Vascular Surgery Department, Cantonal Hospital Zenica, Bosnia and Herzegovina from June 2021 to June 2023 with symptomatic and asymptomatic internal carotid artery (ICA) stenosis. They were randomized based on even and odd numbers on dice thrown by medical technicians. The study was performed in one medical institution by one chief vascular surgeon (who assigned patients to surgery) and different assistants. The trial was paused in June 2023 due to technical reasons. Before and after surgery was conducted, all patients were examined by 2 neurologists. The inclusion criteria were asymptomatic stenosis of ICA ≥ 70% or symptomatic stenosis of the ICA ≥ 50% with cortical dysfunction, transient loss of vision, chronic ocular ischemic syndrome, weakness, sensory or motoric impairment of the face, arms, or legs (one or all areas may be affected) 5 and age >18 years. The exclusion criteria were hematological-oncological diseases, a condition after neck irradiation, congenital carotid artery hypoplasia unilaterally or bilaterally, complicated anatomy, spontaneous intracranial hemorrhage in the last 12 months, inability to understand and collaborate during the study, malignant arrhythmia, and pregnancy. We used recommendations for treatment of cerebrovascular diseases accepted by the Society for Vascular Surgery guidelines.11
The primary outcomes were blood pressure, heart rate, blood oxygen saturation, diuresis, neurological findings, arrhythmia, myocardial infarction, transient ischemic attack (TIA), cerebrovascular insult/stroke (ICV), hemorrhage (drainage in a vacuum drain), surgical re-interventions, cranial nerve injuries, and wound infection during hospital stay (before and after surgery). Computed tomography (CT) was performed after 24 hours if new clinical signs of stroke appeared. The secondary outcomes were measured at 7 and 30 days after surgery and comprised blood pressure, heart frequency, blood oxygen saturation, body temperature, neurological findings, arrhythmia, myocardial infarction, TIA, ICV, repeated surgical interventions, cranial nerve injuries, wound infection, and carotid color Doppler findings.
Patient management. All patients with previous stroke were examined by a neurologist to determine their neurological clinical status. Patients were on 75 mg of clopidogrel (Synetra®, Alkaloid, Skopje, North Macedonia; Zyllt®, Krka, Novo Mesto, Slovenia; Plavix®, Sanofi, Paris, France) continuously before admission to the hospital and after surgery, which was prescribed by a specialist of internal medicine, neurologists, cardiologists, and anesthesiologists. One hour before surgery, all patients received oral 100 mg of acetyl salicylic acid (Aspirin®, Bayer, Leverkusen, Germany), 40 mg of atorvastatin (Avasta®, Alkaloid, Skopje, North Macedonia), and 10 mg of diazepam (Apaurin®, Krka, Novo Mesto, Slovenia). Throughout the surgical procedure, vital signs were monitored by an invasive blood pressure monitor through arteries of the upper extremities (radial or brachial) opposite to the surgical field, as well as a 6-channel electrocardiogram (ECG) and a blood-saturation (finger sensor). Regional cervical anesthesia was established using 80-100 ml of 1% lidocaine-hydrochloride (Lidokainklorid®, Belupo, Koprivnica, Croatia).

- Consort statement on conscription and randomization of patients

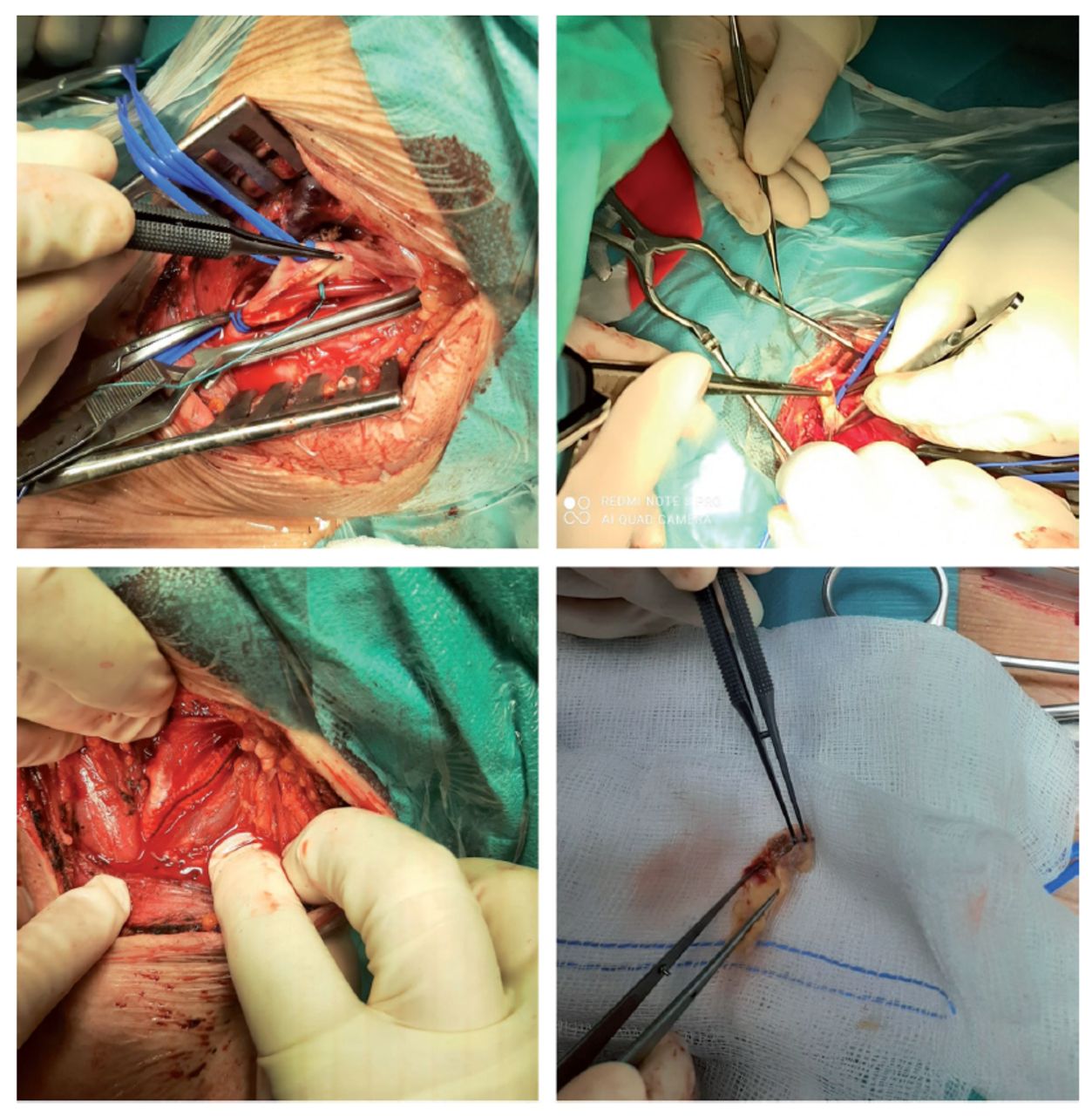
- Carotid surgery (carotid shunt, eversion carotid endarterectomy, carotid endarterectomy with patch angioplasty, plaque)
The surgical approach was from the projection of the front edge of the sternocleidomastoid muscle. We administered 100 IU/kg of unfractionated heparin through an intravenous (i.v.) route before clamp. The surgeon used an eversion or angioplasty technique with a collagen-coated knitted polyester vascular patch (Hemagard Carotid Patch ultrathin®, Getinge, Göteborg, Sweden), and a carotid shunt used once for p-CEA. Color doppler measurements were performed with a Versana Premier® (General Electrics, Boston, USA), and neurological examination was performed by 2 specialists in neurology for the identification of neurological clinical status, possible residual carotid stenosis, early carotid occlusion, carotid dissection, bleeding, and hematomas of the neck at 7 a 30 days after departure from the hospital.
Statistical analysis
Descriptive statistics were generated, and continuous measures were summarized as the median with interquartile range due to a nonparametric data distribution. Categorical traits were summarized using percentages. For statistical analyses, IBM SPSS Statistics v. 27.0.1 (IBMCorp, Armonk, NY, USA). The Mann–Whitney U test, independent-sample t-test, chi-squared test, and Fisher’s exact test were used to determine differences within groups for continuous and categorical variables, and p<0.05 was considered statistically significant.
Results
The following results were obtained from the 62 patients. Two patients were excluded due to cardiac complications before surgery. Thirty (50%) patients were females with an average age of 63.77±7.93 years, while the average age of males was 67.73±6.56 years. Male patients were significantly older (t=-2.112, p=0.039). Twelve (20%) patients had ipsilateral stenosis, and 4 (6.7%) patients had asymptomatic stenosis. Family history was positive for stroke among 51 (85%) patients. Stroke occurred at some point in life for 27 (45%) patients, and TIA was diagnosed in 29 (48.3%) cases.
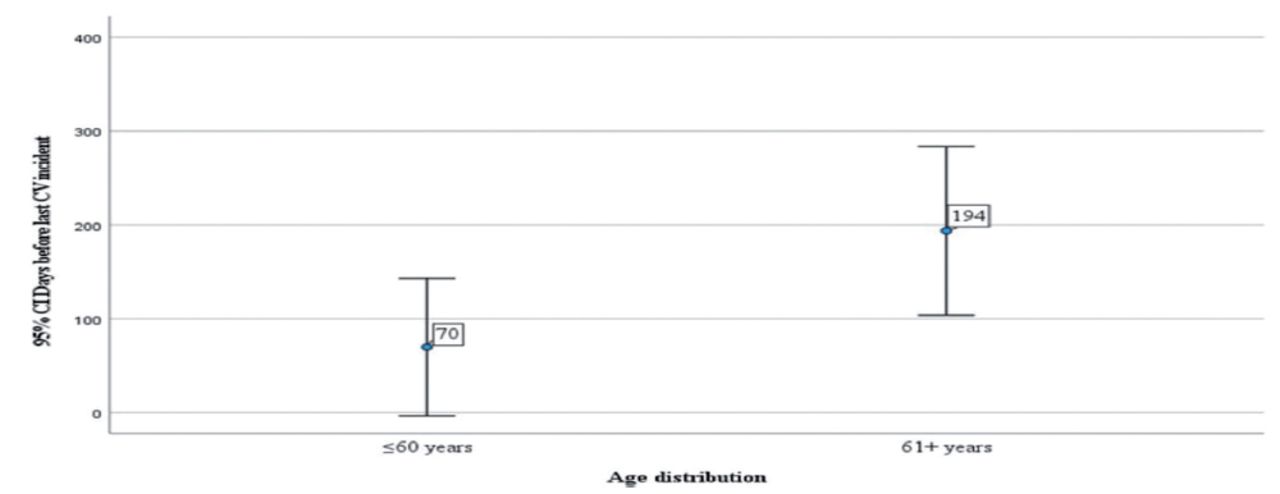
It is important to note that all patients had multiple comorbidities, and the average number was 8±1.8 comorbidities. The lowest number of comorbidities was 2, and the highest was 13 in one patient. A significant difference was observed in the occurrence of dyslipidemia among patients who later went on pCEA (p=0.006). The mean time from the first ICV or TIA was 159.30 days. The median was 26 days, the interquartile range (IQR) was 0 to 202 days, and the total range from 1 to 1200 days. Patients with symptomatic carotid stenosis had neurological symptoms on a daily or weekly basis
The patients’ social backgrounds and post-traumatic stress disorder (war traumas) challenged us to provide timely surgical intervention despite all the recommendations.5,6 We were not able to predict differences between groups regarding age, gender, degree of carotid stenosis, and comorbidities. Fisher’s exact test showed significant differences in the frequency of administration of clopidogrel 48 hours before surgery between the e-CEA 26 (83.9%) and p-CEA 23 (74.2%) groups (p=0.349). The median E-CEA clamp time was 24.0 minutes with an IQR of 21.0-27.0 minutes. The median p-CEA clamp time was 33 minutes with an IQR of 29.0-36.0 minutes. The difference was statistically significant (p<0.001).
A significant difference in arrhythmia occurrence during surgery between e-CEA versus p-CEA (70% vs 30.3%) was observed using Fisher’s exact test during surgery p=0.004 and 24 hours after surgery e-CEA vs p-CEA (66.7% vs 33.3%) p=0.010. No significant difference 7 days after surgery e-CEA vs p-CEA (46.7% vs 33.3%) p=0.292 and 30 days after e-CEA vs p-CEA (30% vs 13.3%) p=0.117. Atrial arrhythmias were significantly more common among patients with e-CEA during surgery (56.7% vs 20.7%) and 24 hours after (56.7% vs 23.3%) Fisher’s exact test, p=0.005.
Discussion
The main finding of our study was that postoperative arrhythmias were significantly more common after e-CEA compared to p-CEA. This was most likely a consequence of carotid body (CB) profound damage or, which was predominately during e-CEA.
From 1954 to today, many CEA techniques have changed, CEA remains an effective treatment Despite the increasing use of carotid artery stenting (CAS) around the world.12-17 Carotid endarterectomy has been the first choice over CAS for symptomatic carotid stenosis according to RCTs and a meta-analysis.18-20 During and after CEA, morbidity and mortality are associated with hemodynamic instability. Blockade of the CB with local anesthetics is not sufficient to protect cardiovascular complications, we did not apply local anesthetics to the CB.21-26
Carotid body is a bilateral organ (chemoreceptor, baroreceptor), located in the carotid bifurcation. Carotid body provide cardiorespiratory regulation in state of hypoxia, hypercapnia (acetylcholine, dopamine, catecholamine, and so on).

- Days before last verified major cerebrovascular incident( incident/age distribution).
- Occurrence of events at 24 hours, 7 days, and 30 days after surgery
- Peak systolic velocity, EDV, stenosis level, and plaque characteristics.
Various surgical procedures on carotid arteries are used to avoid most common complication – embolism, usage of unfractionated heparin (UFH) intravenously before or during clamping (we used 100 i.j.UFH/kg i.v.).27-29 Control of the unaltered (clean) distal ICA is important part of CEA surgical.27,30,31 Our technique of exposure and dissection is characterized by putting loop around the external carotid artery (ECA) and then around the CCA with a “non-touch” technique and no loop around the liberated ICA. The probe clamping had the following order: ICA, CCA, and ICE. A decision for shunt after 120 seconds was made, and reperfusion was not commonly performed. When we performed internal carotid resection, we cut through the root of the ICA and through the CB, after which we did reinsertion and sutured through CB.
A million cases of atrial fibrillation occurring in Germany alone.29 After acute myocardial infarction, the incidence of atrial fibrillation was found to be 7.8% among patients admitted to King Khaled University Hospital, Riyadh, Saudi Arabia.32 Subclinical asymptomatic episodes of paroxysmal atrial fibrillation are called silent atrial fibrillation and are often related to silent cerebral infarction (stroke without clinical signs).29,30
We did not notice any clinical signs or clinical consequences according to the patient state regarding arrhythmia except for patient agitation (not measured or qualified) and it was just subjective observation by the surgical team. One patient had a malignant hypertension crisis after p-CEA, and one patient received an emergency embolectomy with a Fogarty catheter. Damage of carotid body and belonging nerve fibers during e-CEA leads to increased sympathetic activity which can be trigger for cardiovascular incident (arrhythmia, HTA, MI, stroke etc).33 During a 12-year study, there was a statistically lower rate of reoperation, stroke, TIA, restenosis, and occlusion during the first postoperative year after p-CEA. Surgeons who performed more CEAs reported a linear increase in performed p-CEA from 50% to 90%, a reduction in restenosis from 9.0% to 1.2% (p<0.001), and a reduction in stroke or TIA from 4.9% to 1.9% (p< 0.001).34
- Peak
Study limitations
We did not use ultrasound guidance in applying regional anesthetics. We did not perform magnetic resonance imaging after surgery for all patients to identify silent strokes due to possible correlation with arrhythmia. We also did not perform CT angiograms or digital subtraction angiograms of carotid vessels after surgery. After 24 hours, patients were not continuously monitored and did not use a Holter monitor during hospitalization or after departure from the hospital, so we could not do a detailed analysis of cardiac rhythm or blood pressure. There was no intraoperative or postoperative cerebral monitoring. Surgical procedures were performed by single chief vascular surgeon. We could not observe patients’ compliance due to medical treatment before hospitalization and after discharge.
In conclusion, medical treatment, patient complexity (often affected by multiple comorbidities-not addressed in most RCTs), socio-cultural backgrounds, lifestyles, and different risk factors, life habits, and preferences had major influence in treatment outcomes. Although e-CEA and p-CEA are an effective and safe techniques for carotid artery stenosis, we suggest the need for further investigation on the incidence and categorization of possible postoperative cardiac arrhythmias following CEA. The clinical implications of various postoperative heart-rhythm disturbances and their long-term effects on patients also need to be examined. Thus, we propose a large multicenter RCT to provide more strong and solid evidence on this topic.
Acknowledgment
We would like to thank American Manuscript Editors (https://americanmanuscripteditors.com/) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 25, 2024.
- Accepted June 10, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.