


Abstract
Objectives: To determine whether 12-month, 2000IU/day vitamin D supplementation cardiometabolically improves treatment naïve type 2 diabetes mellitus (T2DM) Saudi patients with vitamin D deficiency.
Methods: This 12-month interventional study was conducted at primary health centers in 5 different residential areas in Riyadh, Saudi Arabia between January 2013 and January 2014. Forty-five Saudi T2DM patients were enrolled. Baseline anthropometrics, glycemic, and lipid profiles were measured and repeated after 6 and 12 months. All subjects were provided with 2000IU vitamin D supplements for one year.
Results: Vitamin D deficiency at baseline was 46.7%, 31.8% after 6 months, and 35.6% after 12 months, indicating an overall improvement in the vitamin D status in the entire cohort. Insulin and homeostatic model assessment-insulin resistance (HOMA-IR) after 12 months were significantly lower than a 6 months (p<0.05), but comparable to baseline values. Mean levels of triglycerides increased overtime from baseline (1.9±0.01 mmol/l) to 12 months (2.1±0.2 mmol). This modest increase in serum triglycerides was parallel to the insignificant decrease in circulating high-density lipoprotein -cholesterol levels.
Conclusion: Twelve-month vitamin D supplementation of 2000IU per day in a cohort of treatment naïve Saudi patients with T2DM resulted in improvement of several cardiometabolic parameters including systolic blood pressure, insulin, and HOMA-IR. Further studies that include a placebo group are suggested to reinforce findings.
Diabetes mellitus (DM) is a major public health problem worldwide. The population of people with DM is on the rise secondary to an aging and urbanized population as well as an increasing prevalence of risk factors such as obesity and physical inactivity.1 In the Kingdom of Saudi Arabia (KSA) alone, the most-recent age-adjusted prevalence of type 2 diabetes mellitus (T2DM) was reported to be 31.6% in adults, considered among the highest in the Gulf region.2 Type 2 diabetes mellitus among Saudis results from the interaction between a genetic predisposition, behavioral, and environmental risk factors, which can manifest as early as pre-teens.3 This is alarming since the long-term cost of diabetes can be crippling to any health care system as there are many associated health problems, including: increased risk of coronary heart disease, eye problems, nerve damage, foot, and kidney problems.4 Vitamin D insufficiency, defined as serum 25-hydroxyvitamin D levels <50 nmol/l (25-OH-D), is also common in patients with T2DM.5 Using this arbitrary definition, it has been estimated that one billion people worldwide have either vitamin D deficiency or insufficiency.6 In KSA, there is an abundance of local literature pointing to an increased prevalence of vitamin D deficiency.7,8 Taken together, current evidence suggests a link between vitamin D deficiency and progression of T2DM, but results are not consistent and therefore the beneficial effects of vitamin D correction among T2DM patients with vitamin D deficiency remains controversial.9,10 Given that patients with T2DM are at higher risk for cardiometabolic complications, this study aims to determine whether vitamin D status improvement through dietary means improves the cardiometabolic profile of treatment naïve T2DM Saudi patients with vitamin D deficiency.
Methods
Site and duration of study
This is 12-month interventional study was conducted at the primary health centers in 5 different residential areas in Riyadh, KSA between January 2013 and January 2014. The present study is a small sub-cohort of several interventional studies carried out previously11,12 by the present study.
Subjects
A total of 45 adult Saudi patients (males and females) aged 21 years and above, diagnosed with T2DM with glycated hemoglobin (HbA1c) not exceeding 12% and hypovitaminosis D (25-OH-D<30 nmol/l). There were no dropouts in the study. A T2DM subject is considered “naïve” if he or she has not been introduced to any hypoglycemic agents. Each patient was educated on dietary vitamin D and these dietary supplementations (2000IU vitamin D/capsule) were taken for 12 months, with follow-up every 6 months. Patients were asked to return unused capsules at every follow-up visit before giving another set of supplements to determine compliance. All subjects were instructed to answer a general questionnaire that included questions on their past and present medical history. Ethical approval was obtained from the College of Science Ethics Committee, King Saud University, Riyadh, Saudi Arabia, following the guidelines set for the use of human subjects under the Helsinki Declaration. All participants underwent thorough physical examination and were required to submit signed written informed consent forms prior to the study.
Exclusion criteria
Patients who were impaired physically or mentally, pregnant women, and those with a creatinine clearance of <60 ml/min, hypersensitivity to vitamin D, hypercalcemia, and/or hyperphosphatemia, active liver disease, malabsorption syndrome, gallbladder disease, taking anti-seizure medications, taking steroids, and cancer treatment patients were excluded from the study. Furthermore, T2DM subjects who had already started oral hypoglycemic were excluded.
Anthropometric measurements
Various anthropometric parameters relevant to the study were assessed with the subject standing barefoot. Hip and waist measurements were carried out using a standardized non-stretchable fiber measuring tape. The hip measurement was measured at the level of greater trochanters (the widest circumference of the hip) on both sides. The waist girth were measured as the smallest horizontal girth between the costal margins and the iliac crests at minimal respiration. The waist-to-hip ratio was calculated by dividing the measurement of the waist (cm) by that of the hips (cm). Both height (cm) and weight (kg) were assessed using conventional and standardized methods. Body mass index was calculated using the formula weight (kg) divided by height in squared meters. A standardized mercurial sphygmomanometer was used to take the blood pressure of each participant 30 minutes after complete rest.
Laboratory parameters
All subjects were required to submit overnight fasting blood samples to analyze the different metabolic parameters at baseline, 6 months, and after 12 months. Fasting plasma glucose, lipid profile, insulin, and creatinine were determined using routine laboratory procedures. Diabetes mellitus is confirmed for fasting plasma glucose >7.0 mmol/l as recommended by the World Health Organization. Serum 25-OH-D was measured using COBAS e-411 automated analyzer (Roche Diagnostics, Indianapolis, IN, USA) in a DEQAS-certified laboratory (PMCO). For serum 25-OH-D assay, the inter-assay coefficient of variation (CV) was 8%, and the intra-assay was 5.6%, with a lower detection limit (LOD) of <4 ng/ml. Vitamin D cut-offs used were the following: deficient (<25 nmol/L), insufficient (25-50 nmol/L), sufficient (50-75 nmol/L), and desirable (>75 nmol/L). Homeostasis model assessment for insulin resistance (HOMA-IR) was computed as insulin (IU) x glucose (mmol/L)/22.5.13
Statistical analysis
Statistical analysis was performed using the IBM SPSS Statistics for Windows version 21.0 (IBMCorp, Armonk, NY, USA). Frequencies were presented as percentages (%) and continuous variables were presented as mean ± standard deviation for normally distributed, and mean ± standard error for non-normally distributed variables. All non-normal variables were log-transformed prior to analysis. A general linear model was used (repeated measures) to compare differences in mean values according to follow-up visits and using season as a covariate. Spearman’s correlation coefficient was used to determine associations between 25-OH-D and the different variables. Significance was set at p-value <0.05.
G*Power version 3.0.10 was used to calculate the sample size (paired observation, 2-tailed). Given a=0.05, ß=0.95 from the mean and standard deviation values of 25-OH-D at baseline and 6 months (sample size of n=44 per group has a power of 0.90, and the actual sample size of n=45 has a power of 0.92).
Literature search
References relevant to the study were searched using the following databases during the writing of the manuscript: PubMed and Web of Science. These references were extracted using the key words “vitamin D”, “interventional studies”, “Saudi Arabia” and “trials”.
Results
A total of 45 subjects were included in the interventional study, with more female participants (n=24) than males (n=21). Table 1 summarize the demographic characteristics of subjects. Most of the patients enrolled were illiterate, 17.8% were able to read and write and more than half were able to attend school, with only 8.9% reach with a higher academic level. Despite the high illiteracy rate in the cohort, almost 70% of the subjects earned within the range of SAR3000-10000. Most of the subjects were from the central region, followed by the southern region with the least participants coming from the west (Table 1).
Demographic characteristics of treatment naïve and vitamin D deficient Saudi type 2 diabetic patients (n=45).
Table 2 describes the anthropometric and metabolic characteristics of all subjects overtime. The mean age group of the cohort was 51.4±8.8 years. Baseline BMI of the subjects was 32.2±5.0 and fell into the obese category. Over the 12 month intervention, most of the metabolic parameters (diastolic blood pressure, glucose, triglycerides, high-density lipoprotein, and total cholesterol, albumin, corrected calcium, and phosphate remained insignificantly different from one another with the exception of systolic blood pressure, which showed significant improvement in 6 months and 12 months as compared with the baseline (p<0.05) and circulating levels of 25-OH-D, which significantly increased at 6 months and 12 months as compared with the baseline (p<0.05). Within one time points, insulin and HOMA-IR at the 12-month follow-up were significantly lower than the 6 month follow-up (p<0.05) (Table 2).
General characteristics of treatment naïve and vitamin D deficient Saudi type 2 diabetic patients according to follow-up (N=45).
Table 3 shows the bivariate associations of serum 25-OH-D to the different anthropometric parameters over time. Most anthropometric parameters were inversely associated with 25-OH-D (BMI at baseline and 6 months; hip circumference at baseline, 6, and 12 months; systolic blood pressure at baseline), but only diastolic blood pressure was found to be significant at baseline (p<0.05). In clinical parameters, corrected calcium was positively associated with vitamin D (p=0.007). At 6 months follow-up, serum 25(OH) vitamin D was found to be inversely and significantly associated with waist circumference (p=0.049), and positively associated with systolic blood pressure (p=0.0003). At 12 months intervention, serum 25(OH) vitamin D was positively associated with insulin (p=0.044), borderline significance with HOMA-IR (p=0.052), and positively associated with HDL-cholesterol (p=0.04). Stratification according to gender was not carried out due to small sample size. The rest of the associations were unremarkable.
Bivariate associations of 25-hydroxyvitamin D levels <50 nmol/l in treatment naïve and vitamin D deficient Saudi type 2 diabetic patients according to follow-up (N=45).
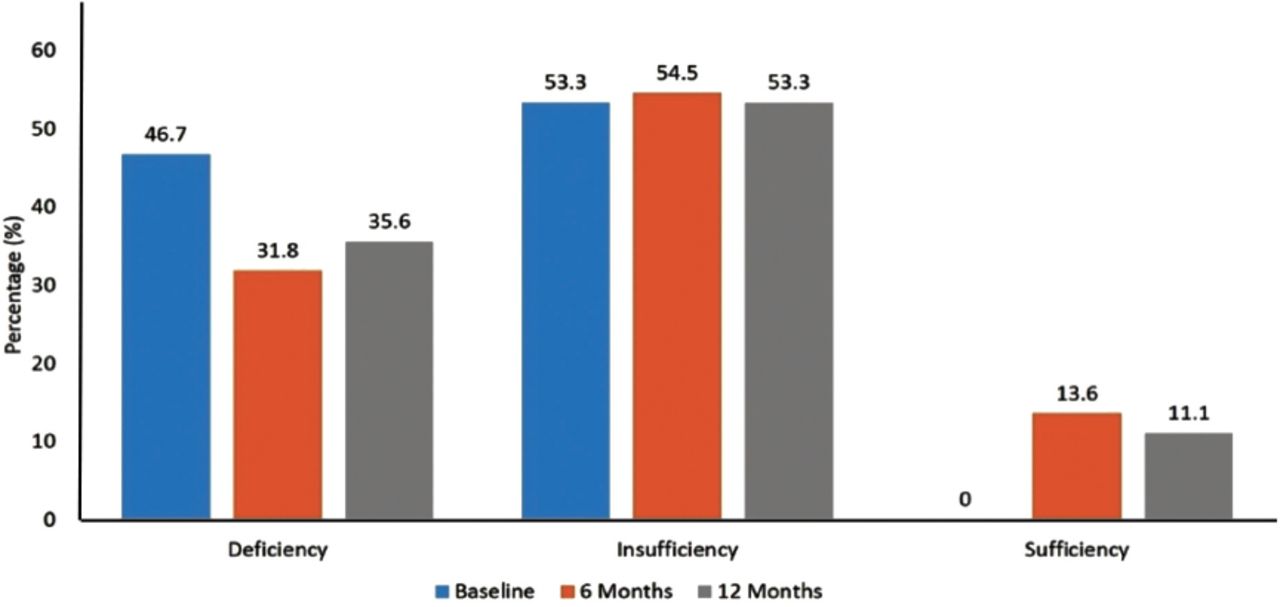
Figure 1 shows the vitamin D status of the entire cohort overtime and revealed that vitamin D deficiency at baseline was 46.7%, 31.8% after 6 months, and 35.6% after 12 months, indicating an overall improvement in the vitamin D status in the entire cohort. Consequently, vitamin D sufficiency was achieved only after 6 months by 13.6% of the entire cohort and modestly dropping to 11.1% after 12 months. Throughout the study, more than half of the entire cohort was vitamin D insufficient (Figure 1).

Prevalence of vitamin D Status in treatment naïve and vitamin D deficient Saudi type 2 diabetic patients according to follow-up.
Discussion
In the present study, we focused on the metabolic effects of vitamin D correction through supplementation among 45 Saudi patients with T2DM who are exclusively on dietary management and without any T2DM medications. It was evident that the mean levels of vitamin D throughout the intervention study did not reach the “sufficient level,” which is >50 nmol/l. The findings of not reaching optimum vitamin D levels despite vitamin D supplementation are in accordance to the observations of Al-Daghri et al11 and Alkharfy et al12 who carried out several interventional studies on vitamin D correction in a similar cohort. Worthy to note is that in the study of Alkharfy et al,12 there were only 15 T2DM subjects out of 499 who were on dietary management, hence no significant changes were observed. In contrast, we were able to elicit significant improvement in the levels of 25(OH) vitamin D. The failure to reach the desired vitamin D levels also confirms other recent studies using a 2000IU supplemental dose in a different ethnic cohort.14 In all studies including the present one, higher vitamin D doses have been recommended.
The inverse relationship between vitamin D and blood pressure has been documented in other studies.15-17 The cardioprotective effect of vitamin D involves inhibition of the renin-angiotensin system and parathyroid hormone levels aside from its renoprotective, anti-inflammatory, and vasculoprotective properties.18 However, the significant improvement in systolic blood pressure as observed in our study is not supported by clinical trials and meta-analyses that do not recommend vitamin D supplementation as an adjuvant anti-hypertensive medication.18,19 However, a similar study carried out by Al-Zahrani et al20 demonstrated the efficacy of vitamin D supplementation in marginally improving blood pressure in Saudi patients with T2DM. Another study by Al-Daghri et al21 found that the prevalence of hypertension in Saudi patients with metabolic syndrome reduced from 28% to 11.1% in a span of 12 months, and this improvement is secondary to non-pharmacologic means of vitamin D correction (increased sunlight exposure and dietary vitamin D intake).
The significant decrease in insulin and HOMA-IR secondary to vitamin D improvement confirm the previous observations of several recent local and international studies on patients with T2DM.22-24 It has been established that the pancreas harbors several vitamin D receptors (VDRs); hence, its ability to convert serum levels of 25(OH)vitamin D to its active form (1,25(OH)vitamin D).25 These VDRs are found in several cell types known to influence metabolism (myocytes, adipocytes and hepatocytes), confirming the substantial role of vitamin D in several key cellular processes.26 Several observational studies carried out in different ethnic backgrounds also attest to the inverse association of circulating vitamin D levels and insulin resistance.27-29 Vitamin D supplementation is still not recommended as an adjuvant therapy in patients with T2DM and further studies, such as the present one, are needed to revisit current recommendations.30
Previous studies11,12,22,31,32 highlighted that during vitamin D correction, the first to clinically improve are the lipids. Vitamin D depletion primarily improves lipid profile through VDRs, which down regulate the small heterodimer partner (SHP) and which concomitantly increases CYP7A1, a major inhibitor of cholesterol levels.33 Higher levels of serum 25(OH)vitamin D promotes the release of apolipoprotein A, the major protein component of HDL-cholesterol.34
Study limitations
The high prevalence of vitamin D deficiency in the cohort used does not apply for the general population since the subjects were all T2DM, and more importantly, monitoring of the vitamin D supplements was not strict, which may explain the persistence of high, but improved prevalence of vitamin D deficiency as well as the inconsistency of significant associations observed at different time points. Important measures such as HBA1c was not included and could have been a good indicator of glycemic status after vitamin D status improvement. Nevertheless, the clinical findings are particularly important in the Saudi T2DM population whose main diabetes management is limited to diet. Other T2DM and vitamin D interventional studies carried out in Saudi Arabia did not take into consideration, important variables such as season and sun exposure time, and these were all included in the present study.
In conclusion, 12-month vitamin D supplementation of 2000IU per day in a cohort of treatment naïve Saudi patients with T2DM resulted in improvement of several key cardiometabolic parameters including systolic blood pressure, insulin, and HOMA-IR. Serum vitamin D was positively associated with HDL-cholesterol and inversely associated with systolic blood pressure, waist circumference, insulin, and HOMA-IR. The present study recommends further investigations on vitamin D supplementation using the same T2DM cohort on a larger scale with a placebo group, higher vitamin D dose, and more stringent selection to include mostly vitamin D deficient subjects’ to reinforce present findings.
Related Articles
Sadat-Ali M, Al-Elq AH, Al-Shaikh IH, Al-Turki HA, Al-Ali AK, Al-Othman AA. Assessment of low vitamin D among Saudi Arabians. Did we overshoot the runway? Saudi Med J 2014; 35: 1243-1249.
AlFaleh KM, Al-Manie AM, Al-Mahmoud HF, Al-Razqan HM, Al-Mutlaq AB, Al-Rumaih SA, et al. Prevalence of vitamin D deficiency in Saudi newborns at a tertiary care center. Saudi Med J 2014; 35: 178-182.
Alramdhan AM, El-Zubair AG. Poor vitamin D supplementation in infants. Cross-sectional study of maternal practices and awareness of vitamin D supplementation in infants in Al-Ahsa, Eastern Saudi Arabia. Saudi Med J 2014; 35: 67-71.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. This study was funded by King Abdulaziz City for Science and Technology (KACST) (Grant No: 11-0536) as well as King Saud University, Deanship of Scientific Research, Prince Mutaib Bin Abdullah Chair for Biomarkers of Osteoporosis, Riyadh, Kingdom of Saudi Arabia.
- Received July 13, 2015.
- Accepted October 24, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.