


Abstract
Objectives: To evaluate early performance indicators for breast cancer screening at the King Abdulaziz University Hospital in Saudi Arabia.
Methods: This study retrospectively evaluated data from women who underwent their first breast cancer screening program in Jeddah, Saudi Arabia between 2012 and 2019. Data on screening results were used to estimate performance indicators and generate descriptive statistics.
Results: Of the 16000 women invited from 2012 to 2019, a total of 1911 (11.9%) participated. The majority of women (68.8%) were between 40 and 55 years old. Based on the screening process results, 26.6%, 40.1%, 9.7%, 1.3%, 0.7%, and 5.2% of women had BI-RADS scores of R1, R2, R3, R4, R5, and R0 respectively. The remaining 16.3% did not have mammogram records. The recall rate, or the percentage of women who underwent further evaluation, was 19.9%; 18.9% underwent a biopsy procedure. In addition, 1.6% of women had cancer screen-detected, although only 0.7% were diagnosed with breast cancer.
Conclusion: In light of the low participation and high recall rates, it is essential that the screening program utilizes performance indicators to optimize resource utilization and ensure the quality of the service provided. Additionally, a national framework and standardized performance indicators could mitigate this problem for other cancer screening programs.
Breast cancer is a leading cause of death worldwide and a serious public health issue that affects many people.1 Breast cancer is the most common form of cancer in Saudi Arabia, according to a recent systematic review.1 In 2020, 14.2% of new cancer diagnoses in Saudi Arabia were breast cancer, and the breast cancer mortality rate was 8.4%.2 Early detection of breast cancer results in a 98.8% increase in cure probability and a nearly 40% reduction in mortality.3-5 However, more than half of breast cancers in Saudi Arabia are detected at an advanced stage, compared to 20% in more advanced countries.6
Early detection of breast cancer involves 3 processes: mammography, breast self-examination, and clinical breast examination.6,7 According to a large meta-analysis, mammography screening programs reduce breast cancer mortality by 33%.8 Additionally, mammography programs can minimize late-stage cases, as seen in many industrialized countries.7,9,10 Therefore, many countries have developed breast cancer screening mammography programs.8 Although mammography can be part of an effective screening program in Saudi Arabia, the culture’s traditional values still limit its efficacy.11-13
As part of its commitment to achieving Vision 2030, Saudi Arabia launched the National Transformation Program in 2016. The new Transformation and Health Care Model consists of actions targeted toward preventing disease, including breast cancer.14 This notion requires the availability of data regarding the performance of breast cancer screening programs in the country. Moreover, monitoring early indicators of breast cancer screening can help optimize resource utilization and improve the quality of service.6,15,16
The purpose of this study is to examine early performance indicators for the cancer screening program at King Abdulaziz University Hospital in Saudi Arabia.
Methods
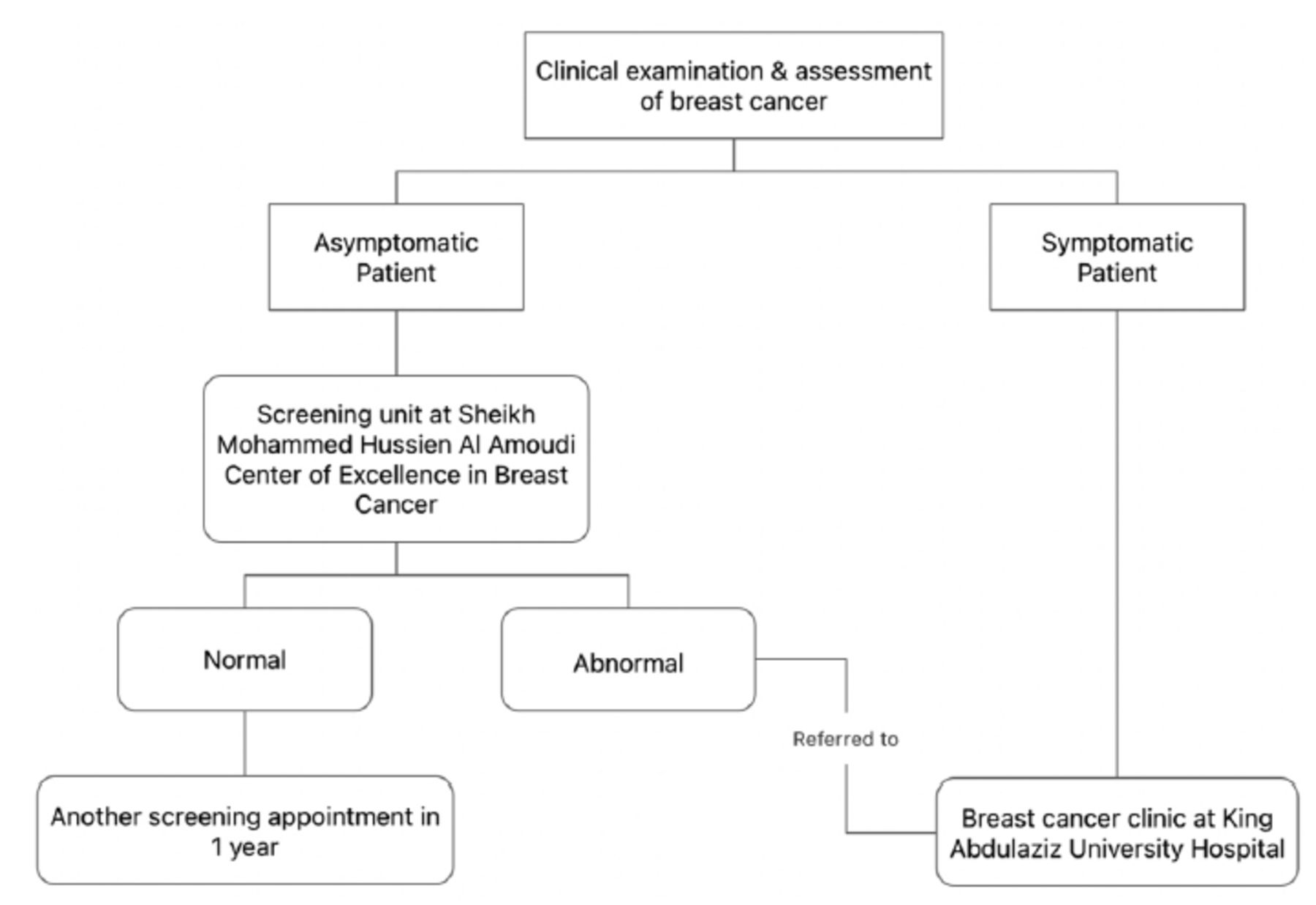
A retrospective analysis of cancer screening data from 2012 to 2019 was carried out in Jeddah, Saudi Arabia. The Breast Cancer Screening Center of Excellence was established at King Abdulaziz University Hospital in Jeddah in 2010; an overview of the screening process can be found in Figure 1. The program aimed to reach women 35-60 years old with a family history of breast cancer residing in Jeddah. The analysis included all participants whose screening records had been completed. Study approval was obtained from the Research Committee and the Institutional Review Board of the King Abdulaziz University) protocol code 54420 and approval date of November 2020), ensuring conformity with the Declaration of Helsinki.
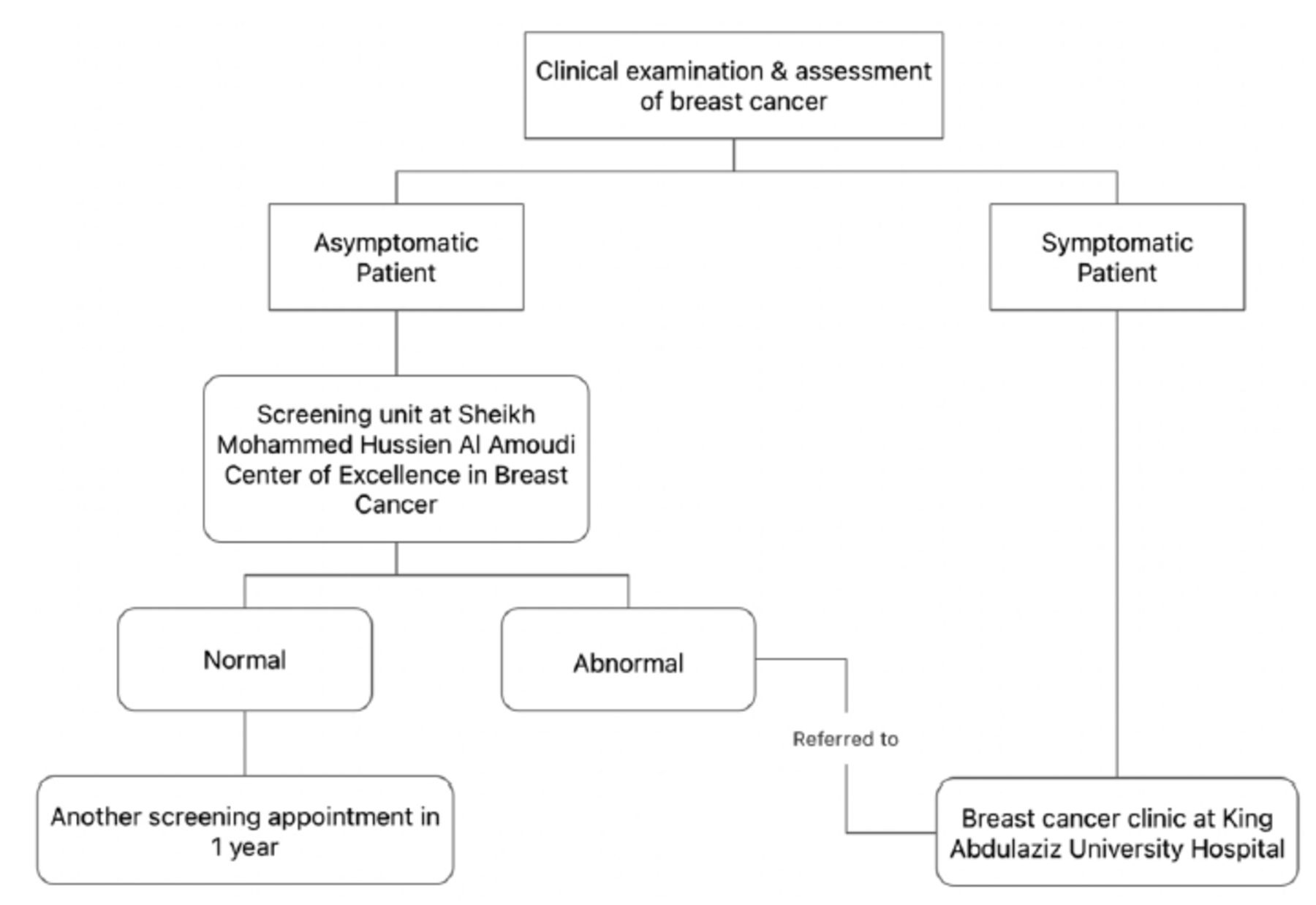
- The flowchart shows the breast cancer screening process at Sheikh Mohammed Hussien Al Amoudi Center of Excellence in the Breast Cancer Screening Unit at King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia.
The data were collected based on the information provided by the cancer screening center. There were 3 main categories of data. The first included information on demographics and risk factors, such as age, marital status, education, menopausal status, late parity, hormone replacement therapy, previous breast cancer history, and a family history of breast cancer. The second included detailed information regarding mammography examination readings taken by 2 oncologists. The Breast Imaging-Reporting and Data System (BI-RADS) of the American College of Radiology was used to score mammograms. The third included information on the mammogram results, including whether further procedures or imaging were required.
Statistical analysis
Performance indicators were estimated based on the screening data. Indicators were chosen based on extensive discussions with the center’s oncologists, data availability, and literature review.17 Performance indicators included participation rate, recall rate, diagnostic workup rate, biopsy rate, detection rate, episode sensitivity, and percentage of confirmed cases. Each of these performance indicators is defined in Table 1. The descriptive statistics were calculated using SAS statistical software (SAS Institute, Inc., Cary, NC, USA).
- Definition of performance indicators of the breast cancer screening program.
Results
There were 1911 women enrolled in the screening program between 2012 and 2019. The demographics of the screening program participants are presented in Table 2. Most of the women (68.8%) were between the ages of 40 and 55 years. Approximately half of the women received hormonal replacement therapy. In addition, 19.8% had a family history of breast cancer. Only 6 women reported a history of breast cancer, and 55 reported a history of benign breast tumors. Eighty-nine women (4.7%) reported having undergone breast surgery (Table 3).
- Characteristics of women enrolled in the program.
- Risk factors and history of surgery of breast cancer
The following distribution of BI-RADS scores was observed among the enrolled women: 26.6% had a score of R1, 40.1% had a score of R2, 9.7% had a score of R3, 1.3% had a score of R4, 0.7% had a score of R5, 5.2% had a score of R0, and 16.3% did not have mammogram records. We further classified patients into 3 categories based on the BI-RADS score. Scores of R1 and R2 indicated no further assessment or imaging was necessary. Scores of R3 and R0 indicated further assessment or imaging was necessary. Scores of R4 and R5 indicated suspected malignancy requiring additional imaging. Among the 1,275 women in the BI-RADS R1 and R2 groups, 9.5% had follow-up imaging, and only 0.2% had follow-up procedures. Of the 286 women in the BI-RADS R3 and R0 groups, 72.7% had follow-up imaging, and only 1.4% had follow-up procedures. A small proportion of women in the program were in the BI-RADS R4 and R5 groups (n=38); 55.3% received follow-up imaging, and 50% underwent follow-up procedures.
With regard to the performance indicators of the screening program, 11.9% of the 16,000 invited women participated between 2012 and 2019. The recall rate, or the proportion of women who underwent further assessment, was 19.9%; 18.9% underwent a biopsy procedure. Of the participants, 1.6% were cancer screen-detected, but only 0.7% were diagnosed with breast cancer. The episode sensitivity, which was defined as the number of women who were screen-detected for cancer divided by the number of confirmed cancers, was 2.4% (Table 4).
- Performance indicators of the breast cancer screening program.
Discussion
This study aimed to evaluate a breast cancer screening program and its performance indicators. Sixteen thousand women were invited between 2012 and 2019. The participation rate was 11.9%, higher than the 7.8% participation rate reported in Kuwait.18 In contrast, this participation rate was much lower than those in developed countries such as Denmark (83.5%) and Germany (56.3%).19 The low participation rate may be explained by a lack of knowledge and sociocultural factors.12,20 For example, a previous study in Saudi Arabia found that women had sufficient knowledge regarding breast cancer risk factors and symptoms, but little information on proper screening methods was available.20
We observed a recall rate of 19.9%, which is higher than the recall rate of 8.8% reported in a large systematic review.21 Furthermore, the recall rates range from 2.6% to 4.6% in Denmark and Germany.19 We also found that 18.9% of the women had undergone a biopsy, which was higher than the 3.9% rate previously reported.21 For screening mammography, the Agency for Healthcare Research and Quality recommends a recall rate of 10%, as evidence suggests that a high recall rate results in fewer cancer diagnoses and more false positives.18,22,23 The annual reading volume and radiologists’ experience may have been related to the screening’s high recall rate.24 A system that targets radiologist factors (for example, screening volumes and second reviews of potential recalls) may reduce unwarranted high screening recalls.25
Study limitations
There were several limitations to this study, including the fact that we had to rely on only one program, which limited the generalizability of the results. Additionally, the current study evaluated the recorded data of the program participants; the researchers had no control over the quality of the data collection. Several cases contained missing data, although this did not affect the study’s findings. Using a prospective method for collecting data will allow future studies to address this issue.
In conclusion, in view of the low participation and high recall rates, it is crucial that breast cancer screening programs be based on performance indicators to optimize resource utilization and ensure the quality of the services provided. Moreover, a national framework and standardized performance indicators would mitigate this problem for other national programs that offer cancer screenings.
Acknowledgment
The authors gratefully acknowledge Editage (www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received June 28, 2022.
- Accepted September 25, 2022.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.