


Abstract
Objectives: To assess the prevalence and metabolic characteristics of lean/non-obese (L/NO) nonalcoholic fatty liver disease (NAFLD) in China.
Methods: The databses, inlcuding PubMed, Web of Science, EMBASE, as well as Cochrane databases, were retrieved for eligible studies. The prevalence together with clinical features of L/NO-NAFLD in China were analyzed using a random/fixed effects model. Lean or nonobese participants were characterized by the cut-offs of body mass index used in original studies. Heterogeneity was identified using meta-regression and subgroup analyses.
Results: We included 25 studies for the final analysis comprising 229091 L/NO Chinese adults and 22641 diagnosed with NAFLD, with the NAFLD prevalence of 8.98% (95% confidence interval [CI]: [5.55-13.13] for L-NAFLD Chinese participants and 13.77% (95% CI: [11.13-16.63]) for NO-NAFLD Chinese participants. This prevalence gradually increased during the past few years. The community and health checkup populations presented similar prevalence (14.19% vs. 13.55%). Meanwhile, L/NO patients with NAFLD showed lower blood pressure (128.86/80.48 vs. 136.09/84.98 mmHg), waist circumference (80.63 vs. 92.73 cm), fasting blood glucose (5.53 vs. 5.69 mmol/L), uric acid (339.14 vs. 365.46 μmol/L), triglyceride levels (1.63 vs. 1.94 mmol/L), alanine transaminase (30.28 vs. 33.12 IU/L), and γ-glutamyl transferase (29.9 vs. 43.68 IU/L), but higher levels of high-density lipoprotein cholesterol (1.33 vs. 1.26 mmol/L) compared to overweight/obese (OW/O) patients with NAFLD.
Conclusion: Prevalence of NAFLD was slightly lower among the L/NO-NAFLD Chinese population than the global level but has obviously increased recently. In addition, the metabolic profile of L/NO-NAFLD patients was generally better compared to OW/O-NAFLD patients.
PROSPERO Reg. No.: CRD42022327240
Approximately 25% of global population suffer from nonalcoholic fatty liver disease (NAFLD), which was closely linked with metabolic disorders, including diabetes, obesity, dyslipidemia, and hypertension.1 Nonalcoholic fatty liver disease can result from central obesity or being overweight (OW), but many NAFLD patients are not obese and lean, called lean/non-obese (L/NO) NAFLD. Body mass index (BMI) is generally used to define L/NO. For the non-Asian NO is generally defined as BMI of <30 kg/m2 and BMI of <25 kg/m2 for Asian population; while lean is defined to be BMI of <25 kg/m2 for the non-Asian and BMI of <23 kg/m2 for Asian population.2-4 Many systematic reviews have reported the prevalence of L-NAFLD to be 4.1-5.1% globally, and for L/NO-NAFLD is 10.2-12.1%. Approximately 40% of NAFLD patients are not obese in the world’s population, nearly one-fifth are lean, and L/NO-NAFLD is more prevalent in Asian than in Western populations. Additionally, L/NO-NAFLD has many liver and non-liver complications over the long term.5-8
The metabolic syndrome characteristics in L/NO-NAFLD subjects are milder than in obese individuals. However, compared to healthy people, the prevalence of metabolic diseases, such as dyslipidemia, insulin resistance, hypertension, as well as diabetes, is still higher among L/NO NAFLD subjects. They are also more prone for severe liver diseases of nonalcoholic steatohepatitis or cirrhosis.9 Besides, some studies showed that a greater risk of severe liver disease and mortality was found in L/NO-NAFLD patients.10,11
Obesity and metabolic diseases have sharply increased with Chinese economic growth and improved living standards. According to a systematic review, the prevalence of NAFLD in China was reported to be 29.2%, exceeding the global prevalence (25%).12 However, there is currently a lack of nationwide epidemiological studies or systematic reviews addressing the prevalence of L/NO NAFLD in China. Therefore, the present meta-analysis reviewed the prevalence, clinical characteristics, and metabolic complications of L/NO-NAFLD in a Chinese population.
Methods
This study followed the evaluation and protocol description in The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 guidelines.
Search strategy
Published studies were retrieved from multiple databases including PubMed, Cochrane Library, Embase, as well as Web of Science with no language restrictions from inception to February 2022.
The following terms were included in the search: non-alcoholic fatty liver disease OR fatty liver OR nonalcoholic steatohepatitis OR nonalcoholic steatohepatitis OR NAFLD OR NASH AND Nonobese OR lean OR non-overweight OR normal weight OR body mass AND prevalence OR epidemiology OR incidence. The MeSH search terms were consisted by NAFLD, prevalence, epidemiology, as well as incidence. Lean, non-obese, non-overweight, body mass index, BMI, thin, thinness, normal weight, and combinations of these terms were free in the title/abstract. Only human studies were included. The references from all publications were manually screened to ensure completeness. Studies on Chinese population were selected by the population source described in the article.
Selection criteria
Original studies that declared their subjects as L/NO Chinese adults over 18 years were included. The inclusion criteria were: I) NAFLD diagnosed by any of the following methods, including ultrasound, magnetic resonance imaging (MRI), computed tomography (CT), as well as liver biopsy, and excluded other causes of liver disorders; and II) for adult Chinese individuals (≥18 years), NO-individuals were defined to be those with BMI of <25 kg/m2, whereas L-individuals was defined as those with BMI of <23 kg/m2. Exclusion criteria included: I) studies without stating the diagnosis methods of NAFLD; II) studies on HBV, HCV, and other liver diseases or excessive consumption of alcohol; III) duplicate studies on the same cohort carried out at the same time (in the case of duplicate papers, the more recent study or largest sample size was included); IV) studies without description of the prevalence of NAFLD or characteristics in genetics, metabolism, or histology of L/NO populations; V) other BMI cut-offs than those mentioned above; VI) obesity or overweight was determined only by waist circumference; VII) case reports, editorials, reviews, meta-analyses, as well as laboratory studies; VIII) participants in the study were selected specifically (namely, veterans, outpatients or inpatients, prisoners); IX) sample size of <50 subjects; and X) the study population was not from China.
Data extraction as well as quality assessment
Two independent investigators (J.Z. and X.H.) collected the data following the MOOSE guidelines13, and a third investigator would be decisive if there was any discrepancy. The following data were extracted: authors’ names, the year the study began, region, population source, NAFLD diagnosing methods, BMI cut-off value defining L/NO, sample size, characteristics of selected populations (namely, BMI, mean age, gender, laboratory parameters, and complications), number of L/NO participants, and NAFLD incidence. We also retrieved the clinical characteristics of L/NO-NAFLD patients, such as waist circumference, level of fasting blood glucose, level of uric acid, level of total cholesterol, level of triglycerides, high-density lipoprotein cholesterol (HDL) level, alanine aminotransferase (ALT) level, low-density lipoprotein cholesterol (LDL) level, as well as γ-glutamyl transferase (GGT) level.
Quality assessment
In the present meta-analysis, studies were accessed according to the Joanna Briggs Institute reviewer’s manual checklist.14 Appendix 1 shows detailed information on the quality assessment. Two authors (J.Z. and X.H.) completed the quality evaluation of studies.
Statistical analysis
Estimation of a pooled prevalence together with 95% confidence intervals (CIs) were adopted as a measurement of outcomes. Besides, the heterogeneity was examined using Cochrane Q test as well as I2 statistics. The value of I2 indicated the degree of heterogeneity (25%: low; 50%: moderate; 75%: high). Based on the degree of heterogeneity, A meta-analysis based on random-effect/fixed-effect models combined the prevalence using Freeman-Tukey double arcsine transformation.13,14 Assessment of publication bias in the analysis was carried out through two methods-Egger’s test as well as funnel plot asymmetry. Subgroup analyses together with multivariable random effect meta-regression were used to identify possible sources of heterogeneity: BMI cut-off values (23, 24, and 25 kg/m2), population type (community or health checkup-based), region (North and South China), study year (2005-2010, 2011-2015, and 2016-2021), sample size, and NAFLD diagnosing methods. The NAFLD prevalence was also calculated for L/NO men and women in China.
Merged NAFLD characteristics were compared between L/NO and overweight/obese (OW/O) patients. Bivariate variables were analyzed by calculating the odds ratio (OR). The standardized mean differences (SMDs) were calculated for continuous variable analysis. The p-value of the test was determined based on Z-value. A p-value of <0.05 was indicative of a statistical significance. R software was used to carry out all statistical analyses (version 4.1.2).15
Results
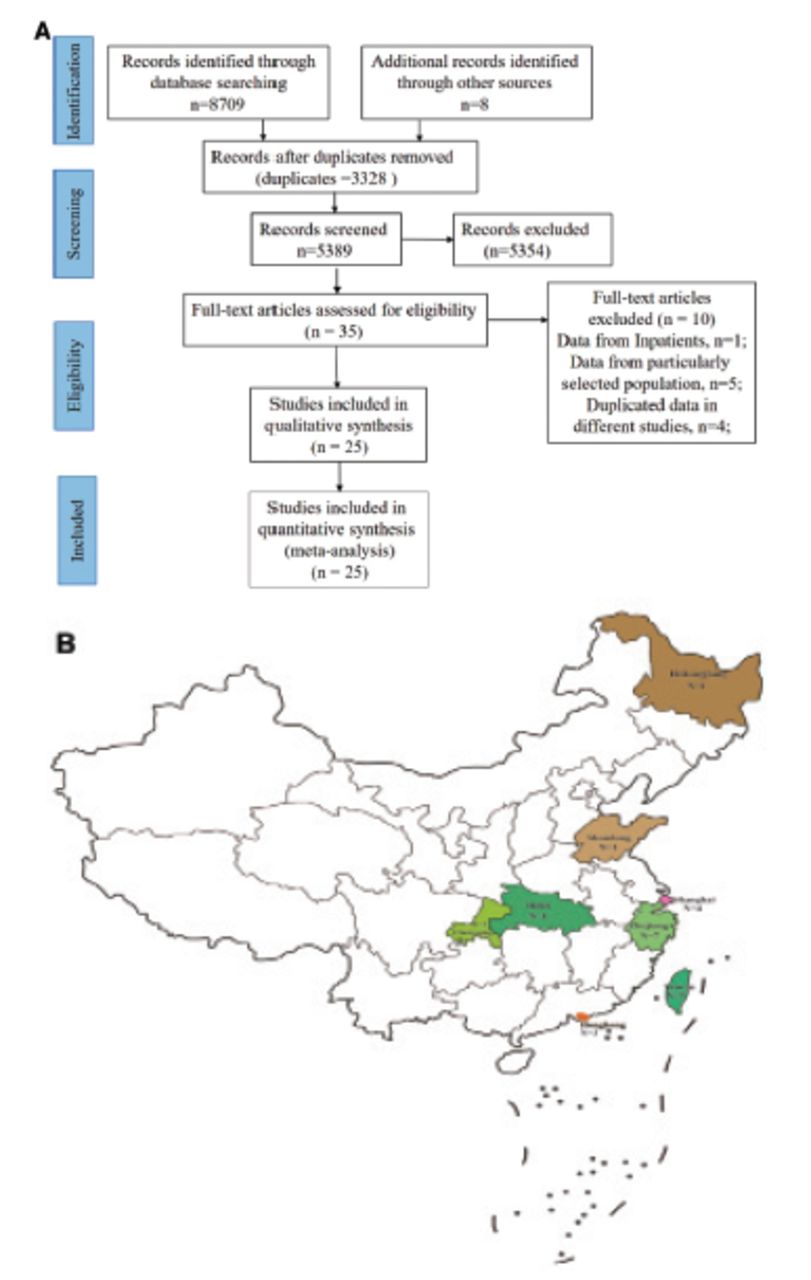
Figure 1A depicted the flowchart of literature selection. Preliminary search identified 8709 publications (Appendix 2), and 8 additional records were added after a manual search. During the title and abstract screening, 3328 duplicates and 5354 publications were excluded. Detailed evaluations were carried out on 35 records that complied with the inclusion criteria, and 10 were removed for various reasons (Figure 1A). This systematic review ultimately included 25 studies comprising 240,072 individuals.

- Flow diagram of the studies’ enrollment and geographical regions of China. A) Flow diagram of the studies’ enrollment by PRISMA. B) The geographical regions of China included in this meta-analysis.
Table 1 described the features of the 25 studies analyzed in the present meta-analysis. We collected studies on NAFLD prevalence in L/NO Chinese from 2006-2020. The study regions were distributed in 8 provinces and cities, and most studies were carried out in Southern China (n=23/25, Figure 1B). A total of 9 studies were community-based, and 16 used health examination data (Table 1).
- Summary of included studies.
The NAFLD prevalence survey was carried out among 240,072 Chinese adults, 229,091 were L/NO, and 22,641 were diagnosed with NAFLD. Besides, sample size varied between 565 and 95,924. A total of 8 studies composed of only L/NO subjects. The NAFLD diagnosing methods included ultrasonography (88%) and H-magnetic resonance spectroscopy (12%).
Quality assessment
Appendix 3 showed the detailed quality evaluations of studies included, which were of a high quality, accompanied by a low risk of bias (Appendix 1).
Assessment of publication bias
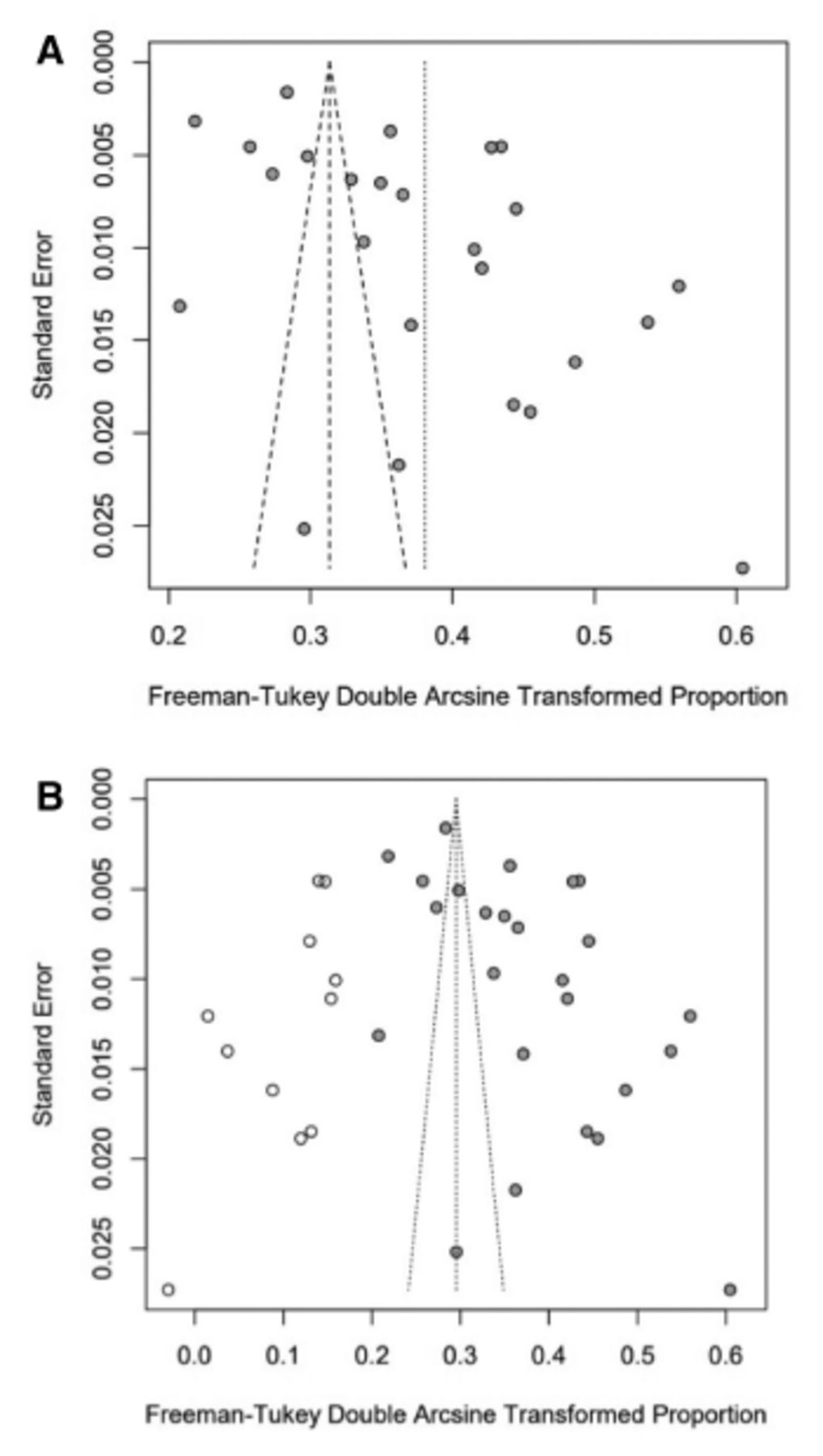
The funnel plot suggested that among the L/NO population, publication bias might exist in the analysis on the prevalence of NAFLD. Egger’s test confirmed publication bias with statistical significance (p=0.0052). Furthermore, the trim-and-fill analysis indicated an adjusted NAFLD prevalence of 8.43% (95% CI: [5.75-11.55]), suggesting that our study might overestimate the prevalence of L/NO-NAFLD in Chinese population (Appendix 3). However, regarding the metabolic characteristics of L/NO compared to obese NAFLD, no publication bias was observed from funnel plots/Egger’s tests, except for 2 subgroups (the prevalence of type 2 diabetes and GGT) from less than 3 studies (Appendix 4).
NAFLD prevalence in the L/NO Chinese population
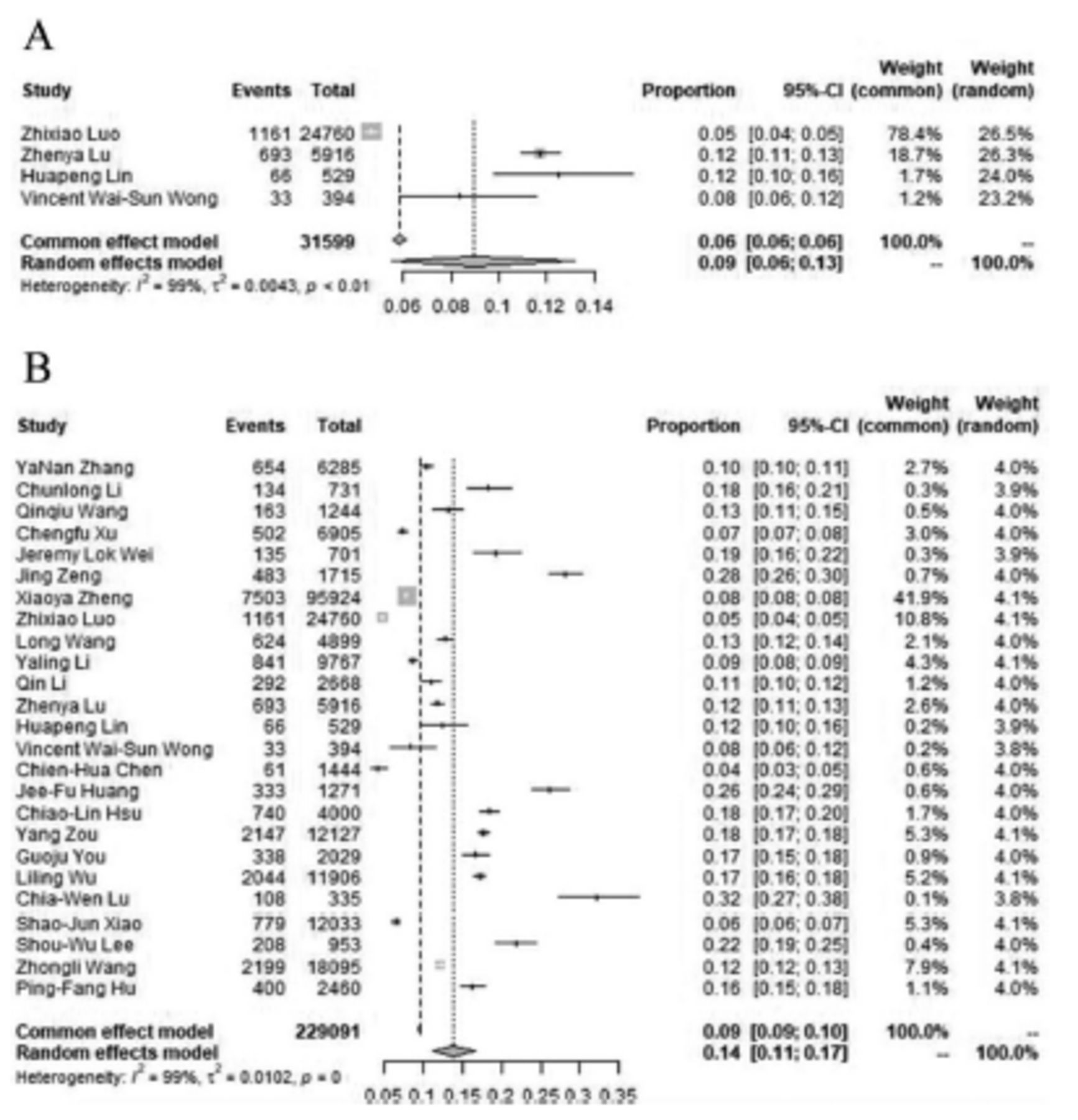
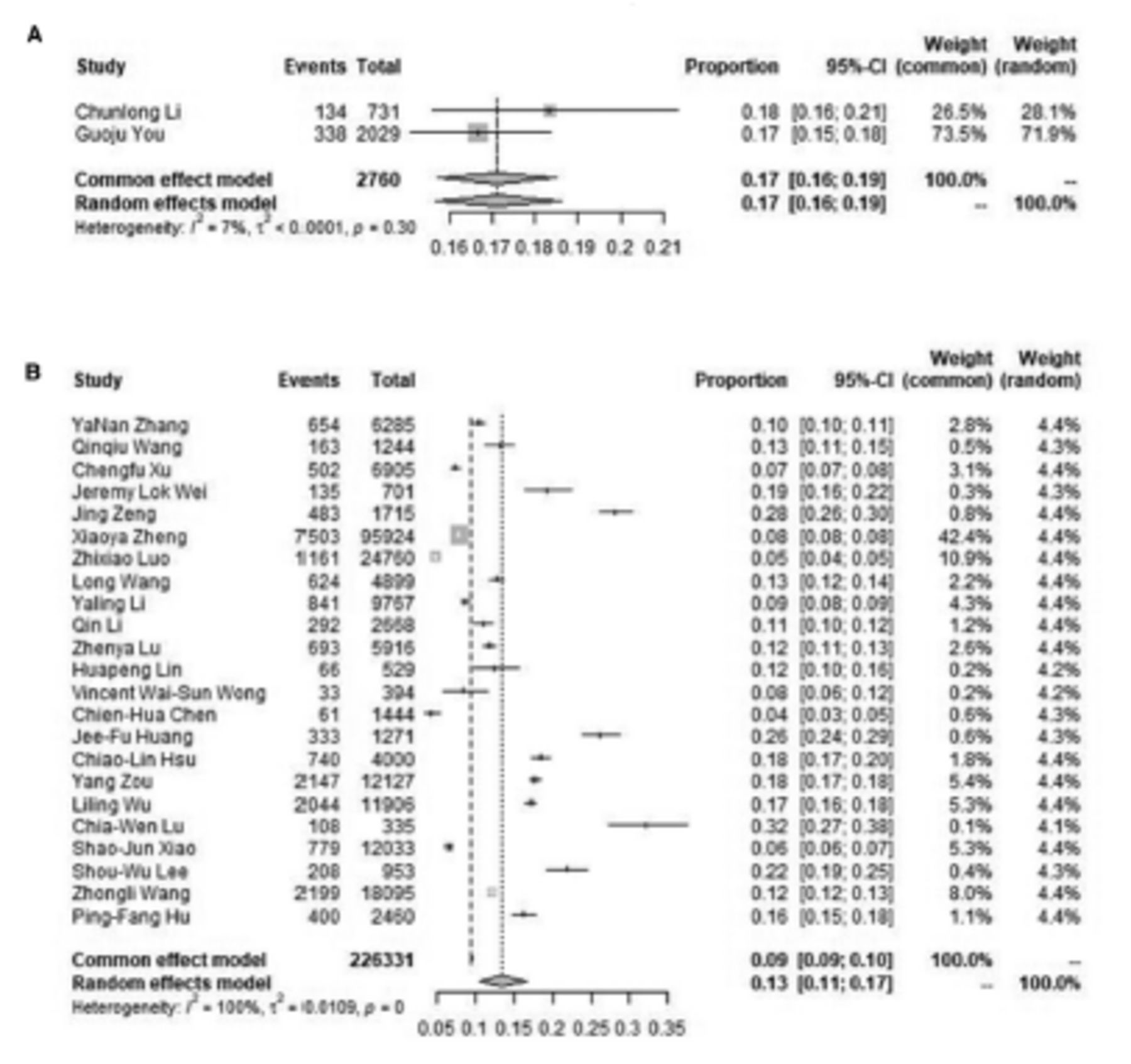
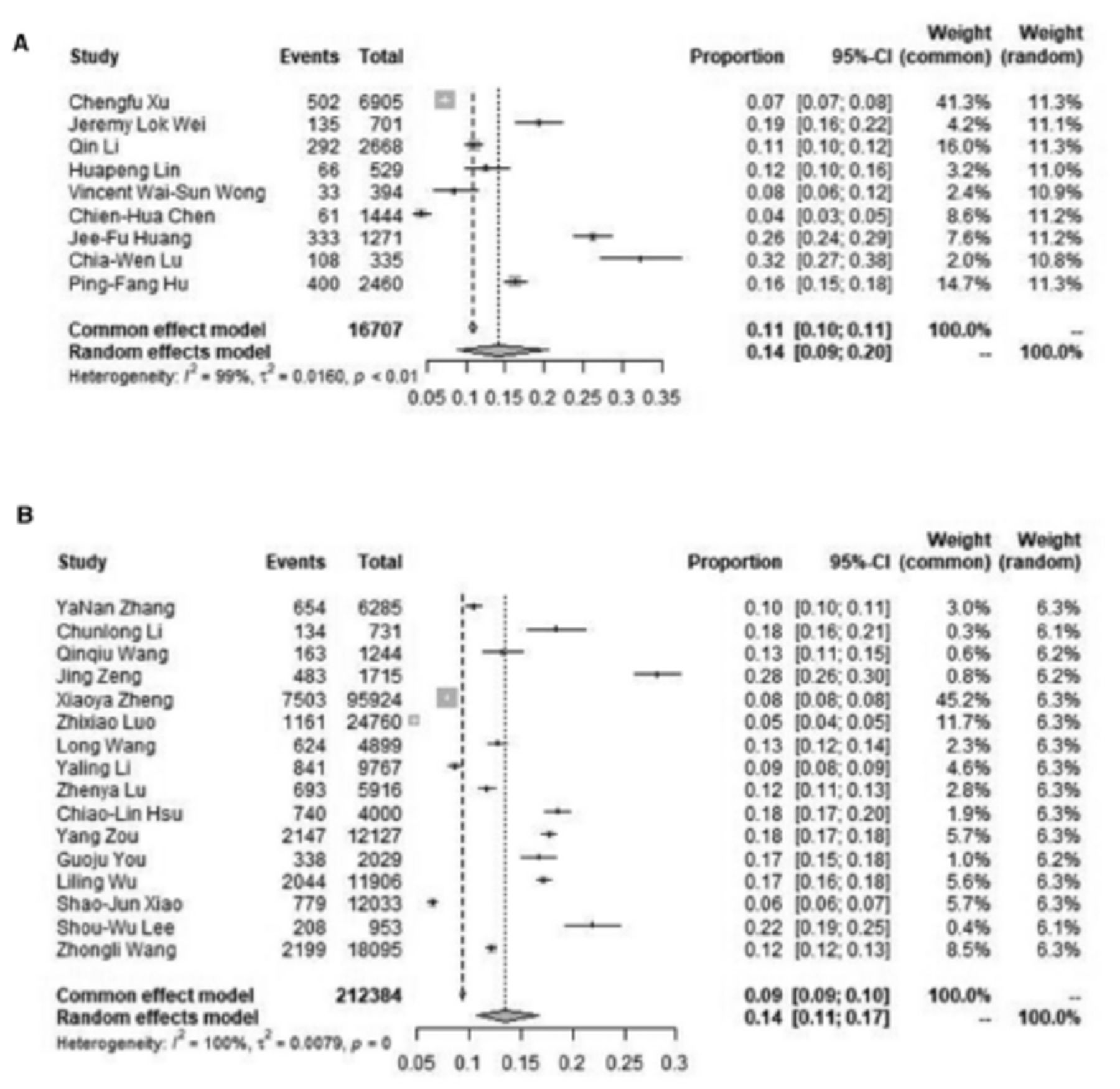
The NAFLD prevalence in lean Chinese was calculated based on 4 studies (n=31599), and the pooled prevalence was 8.98% (95% CI: [5.55-13.13]) with a significant heterogeneity degree (I2=99.2%). The forest plot shows the NAFLD prevalence in the lean Chinese population (Figure 2A). There were 25 studies included to evaluate the NO-NAFLD prevalence in Chinese population (n=229091). The pooled prevalence was 13.77% (95% CI: [11.13-16.63]), and the studies had significant heterogeneity (I2=99.5%). The forest plot of NO-NAFLD prevalence in the Chinese population was shown in Figure 2B. A higher NAFLD prevalence was found in NO-population compared to lean population. Lean/non-obese was defined by the authors of the original studies.

- Forest plot for the lean/nonobese NAFLD prevalence by meta-analysis. A) NAFLD prevalence in lean subjects of China. B) NAFLD prevalence in nonobese subjects of China.
Subgroup analysis for various cut-offs of BMI, regions, and sources of population
Figure 3A provided a subgroup analysis based on various BMI cut-offs, regions, as well as sources of population.

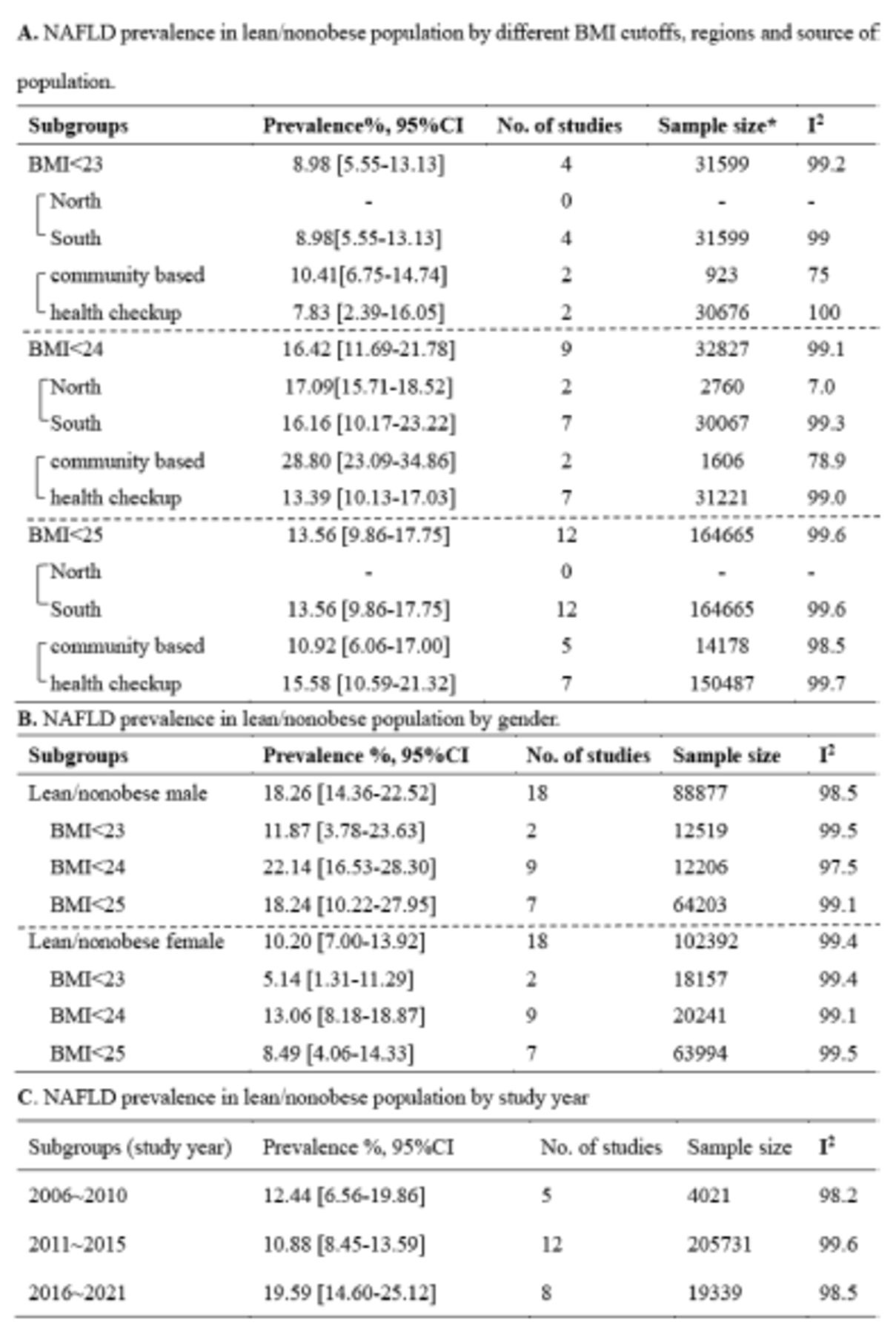
- Summary of subgroup analysis of NAFLD prevalence by different BMI cut-offs, regions, genders, study year, and population source. A) NAFLD prevalence in lean/nonobese population by different BMI cut-offs, regions, and population source. B) NAFLD prevalence in lean/nonobese population by study year. C) NAFLD prevalence in lean/nonobese men or women of China by different BMI cut-offs. *Sample size refers to the total number of lean/nonobese subjects in the study. BMI: body mass index, CI: confidence interval, NAFLD: nonalcoholic fatty liver disease
Among the 25 included studies, 4 (n=31599) used a BMI of 23 kg/m2 as the cut-off with NAFLD prevalence was 8.98% (95% CI [5.55-13.13]). A total of 9 studies (n=32827) used 24 kg/m2 as the BMI cut-off, with 16.42% of NAFLD (95% CI: [11.69-21.78]). In the remaining 12 studies, the BMI cut-off value was 25 kg/m2 (n=164665), presenting a pooled prevalence of NAFLD to be 13.56% (95% CI: [9.86-17.75]; Figure 3A).
Only 2 of the 25 included studies were from Northern China, and the remaining 23 were from Southern China. The BMI cut-off was 24 kg/m2 for both studies in the North, and the estimated NAFLD prevalence was 17.09% (95% CI: [15.71-18.52]), while in the South, the NO-NAFLD incidence was 13.47% (95% CI: [10.67-16.53]), lower than the North (Appendix 5). Further, the subgroup analysis with different BMI cut-offs in Southern China showed that the NAFLD prevalence for BMI of 23 kg/m2 (4 studies, n=31,599) was 8.98% (95% CI: [5.55-13.13]), and 16.16% (95% CI: [10.17-23.22]) for BMI of 24 kg/m2 (7 studies, n=30,067). Among the studies (12 studies, n=164,665) using BMI cut-off as 25 kg/m2, the prevalence of NAFLD was 13.56% (95% CI: [9.86-17.75]; Figure 3A).
As shown in Appendix 6, overall, community-based studies estimated a similar prevalence of L/NO-NAFLD (14.19%, 95% CI: [8.87-20.49]) to health checkup-based studies (13.55%, 95% CI: [10.69-16.68]). Figure 3A displays the subgroup analysis on the NAFLD prevalence for different BMI cut-offs in the community or health checkup-based studies. The prevalence of NAFLD for community-based studies was 10.41% (2 studies, n=923, 95% CI: [6.75-14.74]), and 7.83% for health checkup-based studies (2 studies, n=30,676, 95% CI: [2.39-16.05]) with the cut-off of BMI to be 23 kg/m2. The NAFLD prevalence was 28.80% (2 studies, n=1606, 95% CI: [23.09-34.86]) in the community-based population and 13.39% in the health checkup-based population (7 studies, n=31,221, 95% CI: [10.13-17.03]) using the BMI cut-off of 24 kg/m2. The prevalence of NAFLD was 10.92% (5 studies, n=14,178, 95% CI: [6.06-17.00]) in community-based studies and 15.58% (7 studies, n=150,487, 95% CI: [10.59-21.32]) in health checkup-based studies using a BMI cut-off of 25 kg/m2. These results indicated that the L/NO-NAFLD prevalence with different BMI cut-offs differed in the populations based on the community/health checkup.
NAFLD prevalence in L/NO male and female populations
The NAFLD prevalence of L/NO men and women was analyzed in 18 studies. The NAFLD prevalence in Chinese L/NO men was 18.26% (18 studies, n=88,877, 95% CI: [14.36-22.52]) and 10.20% (18 studies, n=102,392, 95% CI: [7.00-13.92]) in women (Figure 3B). Prevalence of NAFLD was 11.87% (2 studies, n=12,519, 95% CI: [3.78-3.63]) in men and 5.14% (2 studies, n=18,157, 95% CI: [1.31-11.29]) in women with the cut-off of BMI to be 23 kg/m2. Prevalence of NAFLD was 22.14% (9 studies, n=12,206, 95% CI: [16.53-28.30]) in men and 13.06% (9 studies, n=20,241, 95% CI: [8.18-18.87]) in women with a cut-off of BMI to be 24 kg/m2. Taking 25 kg/m2 as the cut-off of BMI, the overall NAFLD prevalence was 18.24% (7 studies, n=64,203, 95% CI: [10.22-27.95]) in men and 8.49% (7 studies, n=63,994, 95% CI: [4.06-14.33]) in women. Hence, a higher NAFLD prevalence was found in the NO Chinese male population (Figure 3B).
Study year (the time when the data collection began)
Recently, NAFLD prevalence has increased among the NO and general population. From 2005-2010, the NAFLD prevalence rate in the NO Chinese population was 13.44% (95% CI: [9.62-17.78]), 11.82% (95% CI: [7.39-17.10]) from 2011-2015, and 17.03% (95% CI: [10.83-24.29]) after 2016 (Figure 3C).
Meta-regression analysis
Since the included studies were significantly heterogeneous, a meta-regression analysis was carried out to clarify sources of heterogeneity that affected the prevalence of L/NO-NAFLD within the Chinese population. Results showed that study year (for the initiation of data collection) (p=0.0053), sample size (p=0.0346), and BMI cut-off (p=0.0013) significantly influenced the estimated NO-NAFLD prevalence (Table 2).
- Multivariable meta-regression of included studies to identify heterogeneous sources affecting the prevalence of nonobese nonalcoholic fatty liver disease in China.
Metabolic characteristics of L/NO vs. OW/O NAFLD
Moreover, we compared the clinical features of L/NO to OW/O NAFLD patients within studies. Overweight/obese NAFLD patients were predominantly males. In contrast, L/NO-NAFLD patients showed a lower incidence of hypertension (41.36 vs. 57.80%), lower levels of blood pressure (128.86/80.48 vs. 136.09/84.98 mmHg), fasting plasma glucose (5.53 vs. 5.69 mmol/L), uric acid (339.14 vs. 365.46 μmmol/L), as well as triglyceride (1.63 vs. 1.94 mmol/L), smaller waist circumference (80.63 vs. 92.73 cm), but higher levels of HDL (1.33 vs. 1.26 mmol/L). The incidence of diabetes (12.64 vs. 15.94%), age, total cholesterol (5.14 vs. 5.13 mmol/L), and LDL levels (3.07 vs. 3.12 mmol/L) did not differ between the 2 groups. Regarding liver function, L/NO-NAFLD patients presented lower ALT (30.28 vs. 33.12 IU/L) and GGT (29.9 vs. 43.68 IU/L) than OW/O NAFLD patients. In summary, the metabolic profiles of L/NO-NAFLD patients were better in contrast with OW/O NAFLD patients (Table 3).
- Comparison of characteristics between lean/nonobese and overweight/obese nonalcoholic fatty liver disease patients.
Discussion
Herein, we carried out a meta-analysis to examine the prevalence of NAFLD, followed by its associated clinical characteristics in L/NO individuals in China. Regarding of the NAFLD prevalence in the L/NO populations, publication bias was identified, which might be attributed to the following: our study was a meta-analysis of proportion studies without controlled data, and the original studies included in this part were cross-sectional studies that only provided the total number of people and percentage of NAFLD patients among them; no positive or negative results were reported in these studies, and only descriptive statistics on the outcome of the disease were carried out without comparing differences. Therefore, some statistical experts suggest that funnel plots were inaccurate method of assessing publication bias for meta-analyses of proportion studies.13,14,16
This updated systematic review and meta-analysis included 25 studies comprising 229,091 individuals from 8 Chinese provinces and cities. The total prevalence of L-NAFLD Chinese population was 8.98% and the total prevalence of NO-NAFLD Chinese population was 13.77%, indicating that NAFLD was relatively common in these populations.
Most of the 25 studies were distributed in Shanghai, Zhejiang, Hong Kong, and Taiwan, and only 2 were from Northern China, indicating that L/NO-NAFLD should receive more attention in this region.
Independent meta-analyses have shown that the global L-NAFLD prevalence was 9.7% and 10.2%, and the global NO-NAFLD prevalence was 15.7% and 14.8%.5-7 Zhou et al12 showed that NAFLD was prevalent in 10.8% of NO Chinese individuals. Our results suggest that the NAFLD prevalence among the L/NO Chinese population was slightly lower than the global level but higher than that of Zhou et al.12 The following results are notable: I) Our meta-analysis indicated a grown trend of L/NO-NAFLD prevalence among the Chinese population, consistent with other meta-analyses.5,7 Zhou et al12 included studies before 2018, and we included studies before 2021. The different study years of the included studies might account for the higher prevalence in our study; II) we also found that 23 of the 25 included studies were from Southern China, and only 2 were from Northern China. Based on the subgroup analysis, Northern China had a slightly higher NAFLD prevalence than southern China among NO people (17.09 vs. 16.16%). Due to the different diets and lifestyles between the North and South, few studies in the North might lead to a lower estimated NAFLD prevalence.
Two population types were included: community and health check-up-based. The subgroup analysis showed an obvious difference of the NAFLD prevalence among the community-based population in contrast to the health check-up-based one. The sample size in the health check-up-based studies was far larger than in the community-based studies. Therefore, the difference in NAFLD prevalence between the 2 groups might be primarily related to the difference in sample size.
Furthermore, we showed that the NAFLD prevalence in the overall population had increased yearly. However, in the L/NO populations, the prevalence of NAFLD fell between 2011 and 2015; after 2016, it began to rise again. This phenomenon was probably due to the substantial differences in sample sizes among the included studies. In the lean population, from 2006-2010, we included 2 studies for subgroup analysis with sample sizes of 529 and 394. Meanwhile, from 2011-2015, sample sizes were 24760 and 5916 patients. Among NO populations, the sample size was found to be different between the 2 periods with a statistical significance. Due to the well-known impact of sample size on prevalence calculation, we believe that the fluctuation of L/NO-NAFLD prevalence might be attributed to this sample size difference.
Moreover, we found the NAFLD prevalence to be 18.26% for L/NO men and 10.2% for L/NO women in China. Subgroup analyses demonstrated that the NAFLD prevalence of women was lower than men, even using different BMI cut-offs. The understanding on the direct relationship of gender with NAFLD susceptibility remains insufficient, and further research is necessary.42 Most studies and meta-analyses have reported a greater L/NO-NAFLD prevalence in men than in women.5-7 Nevertheless, few studies have concluded a higher L/NO-NAFLD incidence in the females.43 According to our meta-analysis, the men had a higher L/NO-NAFLD prevalence compared to the women in China. Menopause or age-specific gender differences have been mentioned in previous studies. Some studies have found that compared to premenopausal women, NAFLD was more frequent in men/postmenopausal women.44-46 A lower NAFLD incidence was found in the females with hormone replacement therapy (HRT) compared to those without HRT.47 Current research suggests that estrogen protects against NAFLD.48 Despite of that, potential mechanisms for differences caused by gender are unclear. A current review has demonstrated that estrogen signaling conferred a high metabolic dynamicity to female livers that prevented and limited the upsurge and deterioration of metabolism and inflammation in the liver even under unbalanced diets, contributing to the gender-specific NAFLD prevalence.49,50 Men are more likely to be exposed to NAFLD risk factors, such as drinking and tobacco use, which might lead to a higher NAFLD incidence. To obtain data from qualified studies was not easy, which hindered the comparison of the prevalence of L/NO-NAFLD between postmenopausal women and men. Gender, age, the status of hormones, and gender disparities across social cultures should be considered in further NAFLD prevalence and therapy investigations.
Herein, we analyzed the epidemiological characteristics of NAFLD in L/NO Chinese people, followed by the comparison of risk factors, metabolic features, as well as complications between L/NO- and OW/O- NAFLD patients. The L/NO-NAFLD patients presented with a better metabolic profile compared to OW/O-NAFLD patients. A lower hypertension prevalence, waist circumference, triglycerides, uric acid levels, liver enzymes, and higher HDL levels were detected in L/NO-NAFLD patients in contrast to OW/O-NAFLD. The above findings were in accordance with previous studies and suggested better metabolic profiles as well as fewer metabolic complications in L/NO-NAFLD patients.5,7,11,51
We used a conventional method to define L/NO-NAFLD using BMI cut-offs based on specific age and ethnics. Scholars have described some NAFLD patients with normal weight who had a higher risk of cardiovascular and metabolic diseases, described as “metabolic obesity normal weight (MONW)”, and confirmed that NAFLD in nonobese individuals was an important predictor of insulin resistance and metabolic disorders.52 Considering the possible influence of visceral adiposity and body fat percentage on NAFLD incidence, more research should be carried out for the L/NO-NAFLD population to explore the risk factors and potential pathogenesis, thereby providing a better understanding of them.
Study limitations
There were several limitations in the present meta-analysis. Firstly, the included studies had significant heterogeneity, and the meta-regression suggested that study year, sample size, and BMI cut-off were the main causes. The types of study populations and NAFLD diagnosis methods might have also resulted in heterogeneous outcomes. However, the meta-regression and subgroup analysis could not fully explain the source of heterogeneity between studies. Of the 25 studies included, only 2 were from North China, which means that data on L/NO-NAFLD from this region are relatively rare, which might lead to biases in our final NAFLD prevalence statistics. Second, due to the lack of data in the original studies, we could not verify and compare the progression risk factors of L/NO- vs. OW/O-NAFLD patients.
In conclusion, the present meta-analysis demonstrated the NAFLD prevalence in the L-Chinese population to be 8.98% and 13.77% in the NO-Chinese population, and presented an upward trend over the years. Compared to the women in China, the L/NO-NAFLD prevalence was higher in the men with statistical significance. The metabolic profiles and liver function of L/NO-NAFLD patients were better than those of OW/O-NAFLD patients. Thus, the different pathogenesis as well as final clinical outcomes of L/NO- and OW/O-NAFLD should be explored to provide more guidance for clinical management.
Acknowledgment
The authors gratefully acknowledge CureEdit for the English language editing.
Appendix
- Quality assessment of included studies in the epidemiology of lean/nonobese NAFLD in China using the JBI-prevalence critical appraisal checklist.14
Questions:
1. Was the sample frame appropriate to address the target population?
2. Were study participants sampled in an appropriate way?
3. Was the sample size adequate?
4. Were the study subjects and the setting described in detail?
5. Was the data analysis carried out with sufficient coverage of the identified sample?
6. Were valid methods used for the identification of the condition?
7. Was the condition measured in a standard, reliable way for all participants?
8. Was there appropriate statistical analysis?
9. Was the response rate adequate, and if not, was the low response rate managed appropriately?
- Numbers of citations by each database searched.

- Funnel plot of publication bias. A) Funnel plot of the 25 original studies included in the analysis. B) Funnel plot of the 25 original studies included in the analysis (black dots) and the missing studies imputed by the trim-and-fill procedure (white dots).
- Egger’s test of subgroups for meta-analysis of clinical characteristics between lean (or non-obese) vs. non-lean or (obese) NAFLD patients.

- Subgroup analysis of NAFLD prevalence in lean/nonobese population by different regions. A) Studies in north China. B) Studies in south China

- Subgroup analysis of NAFLD prevalence in lean/nonobese Chinese population by source of population. A) Studies based on population. B) Studies based on health check-up.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 10, 2023.
- Accepted July 25, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}