

Abstract
Objectives: To examine the associations between 6-minute walk test (6MWT) and lung functions, blood gas analysis findings, fractional exhaled nitric oxide (FeNO), and hospital stay in interstitial lung disease (ILD).
Methods: The present retrospective study included patients hospitalized in Beijing Hospital of Traditional Chinese Medicine, Capital Medical University between September 2018 and December 2019. The outcomes included the difference between the actual and predicted 6MWT values (6MWT difference) and the ratio of the actual to predicted 6MWT value (6MWT ratio).
Results: This study included 137 patients. The predicted 6MWT value was 519±61 m and the actual 6MWT value was 449 (196.5,694)m. The 6MWT ratio was 84.7±177.6 and 6MWT difference was 73.9±95.1 m. Fractional exhaled nitric oxide (FeNO) (β= -2.157, standard error [SE]=0.836, p=0.014) and diffusing capacity of the lungs for carbon monoxide (DLCO) (β= -22.528, SE=7.48, p=0.004) had independent associations with 6MWT difference. The FeNO (β=0.403, SE=0.163, p=0.018) and DLCO (β=4.355, SE=1.458, p=0.005) had independent associations with 6MWT ratio.
Conclusion: In ILD, 6MWT difference and 6MWT ratio were associated with FeNO and DLCO. The 6MWT value was not associated with hospital stay. Therefore, the 6MWT might be a surrogate marker of pulmonary function in clinical ILD.
Interstitial lung disease (ILD) generally features the thickening of the pulmonary interstitium due to inflammation or fibrosis, leading to impaired gas exchange. Interstitial lung disease might be idiopathic or caused by identifiable factors such as exposure to organic and inorganic chemicals, diseases (such as connective tissue diseases and multisystemic diseases), drugs, smoking, infection, and radiation therapy.1,2 The most common type of idiopathic ILD is idiopathic pulmonary fibrosis (IPF).3,4 The risk factors associated with specific types of ILD include smoking, exposure to organic and inorganic substances, selected medications, and specific systemic conditions. Idiopathic pulmonary fibrosis represents the most prevalent idiopathic ILD and is more common in men and adults aged >55 years. The estimated incidence is 26.1-31.5/100,000 person-years, with an estimated prevalence of 25-74/100,000.1,2 The specific management depends on the underlying disease type, with tailored interventions aimed at ameliorating disease and slowing progression while improving or maintaining the quality of life.5 Disease management generally includes smoking cessation, influenza and pneumococcal vaccines, antifibrotic medications, and pulmonary rehabilitation. Prognosis is often associated with increased mortality but varies greatly by ILD type and treatment efficacy.1,2
The 6-minute walk test (6MWT) assesses the distance a person walks in a 6-minute period on a hard, flat, and leveled surface. Since the score increases with physical condition, the person has to walk the longest possible distance within 6 minutes.6,7 The 6MWT displays moderate to high correlations between 6MWT distance and maximal oxygen consumption (VO2max) obtained by maximal exercise testing in individuals with heart failure and chronic heart or lung diseases.6-8 Its accuracy is 80%, with sensitivity and specificity >90%, compared to VO2max. The 6MWT is a useful test in various patients with compromised lung function.6-9 It is associated with forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC), partial pressure of oxygen (PO2), and partial pressure of carbon dioxide (PCO2) in individuals affected by chronic lung diseases.10
In addition, the 6MWT can be affected by age, body shape/composition, comorbidities, drugs, and oxygen use.11 Fractional exhaled nitric oxide (FeNO) is often higher in individuals showing pulmonary conditions but is not sensitive to condition changes over time.12,13 Nevertheless, the relationships among 6MWT value, pulmonary function variables, and FeNO are poorly described in ILD.
Hence, this study examined the associations of 6MWT value with pulmonary functions, blood gas analysis findings, FeNO results, and hospital stay in patients with ILD. The findings could help determine the most optimal test for managing patients with ILD.
Methods
A retrospective analysis of 137 patients hospitalized in Beijing Hospital of Traditional Chinese Medicine, Capital Medical University, Beijing, China from September 2018 to December 2019. The study obtained approval from the Ethics Committee of Beijing Hospital of Traditional Chinese Medicine, Capital Medical University, and no informed consent was required.
The inclusion criteria were meeting diagnostic criteria for ILD, and completion of the 6MWT, pulmonary function test, blood gas analysis, and FeNO testing on hospital admission. While the exclusion criteria were patients who had cognitive impairment, dementia, or severe psychological disorder, or patients who were not able to complete pulmonary rehabilitation training. A query of PubMed, Web of Science, Google Scholar, and the Cochrane Library was carried out for relevant research. The study outcomes encompassed the difference between the actual and predicted 6MWT values (such as 6MWT difference) and actual 6MWT value/predicted 6MWT value ratio (such as 6MWT ratio). All clinical data were from patient charts, including demographic characteristics (gender, age, height, and body weight), diagnosis on admission, pulmonary function data, blood gas analysis findings, 6MWT value, and hospital stay.
The predicted 6MWT value was calculated as 757×height (m)–5.02×age (years)–1.76×body weight (kg)–309 for males; and 211×height (m)–5.78×age (years)–2.29×body weight (kg)+667 for females.
Statistical analysis
Continuous variates were examined for normality by the Kolmogorov-Smirnov test. Normally distributed continuous variates are mean±standard deviation (SD), and median (min, max) was utilized to describe those with skewed distribution. Categorical data were reported as n (%). Pearson’s and Spearman’s correlation tests were carried out, as appropriate, to examine the associations of 6MWT difference and 6MWT ratio with blood gas analysis findings and pulmonary function data. Univariable linear regression analysis was performed to examine factors associated with patient outcomes (6MWT difference and 6MWT ratio); variables with p<0.10 were entered in multivariable linear regression analysis. Double-sided p<0.05 was deemed to reflect statistical significance. Statistical Package for the Social Sciences, Windows 22.0 (IBM, Armonk, NY, USA) was employed to analyze all data.
Results
Table 1 presents the characteristics of the 137 analyzed cases. Median age was 63 (35,93) years, and there were 71 (51.8%) males. The diagnoses included connective tissue-related lung diseases (30.9%), idiopathic interstitial pneumonia (21.3%), granulomatous disease (2.2%), and unknown disorders (45.6%). Forty-two (30.7%) patients required oxygen inhalation. The median hospitalization duration was 9 (1,20) days.
- Baseline patient characteristics.
The 6MWT, blood gas analysis, and pulmonary function data
In the 137 examined patients, the predicted 6MWT value was 519±61 m and the actual 6MWT value was 449 (196.5,694) m. Hence, 6MWT ratio was 84.7±177.6, and 6MWT difference was 73.9±95.1 m. The actual FVC was 2.46±0.76 L and the FEV1 was 1.97±0.57 L; total lung capacity (TLC) was 4.00±1.00 L, and diffusing capacity of the lungs for carbon monoxide (DLCO) was 4.48±1.51 mmol/min.kPa. Partial pressure of oxygen was 79.2±14.4 mmHg, PCO2 was 38.9 (27.6,78.1) mmHg, and the FeNO were 17.5 (5,69) ppb. (Table 1).
Associations of 6MWT indexes with blood gas analysis and pulmonary function data
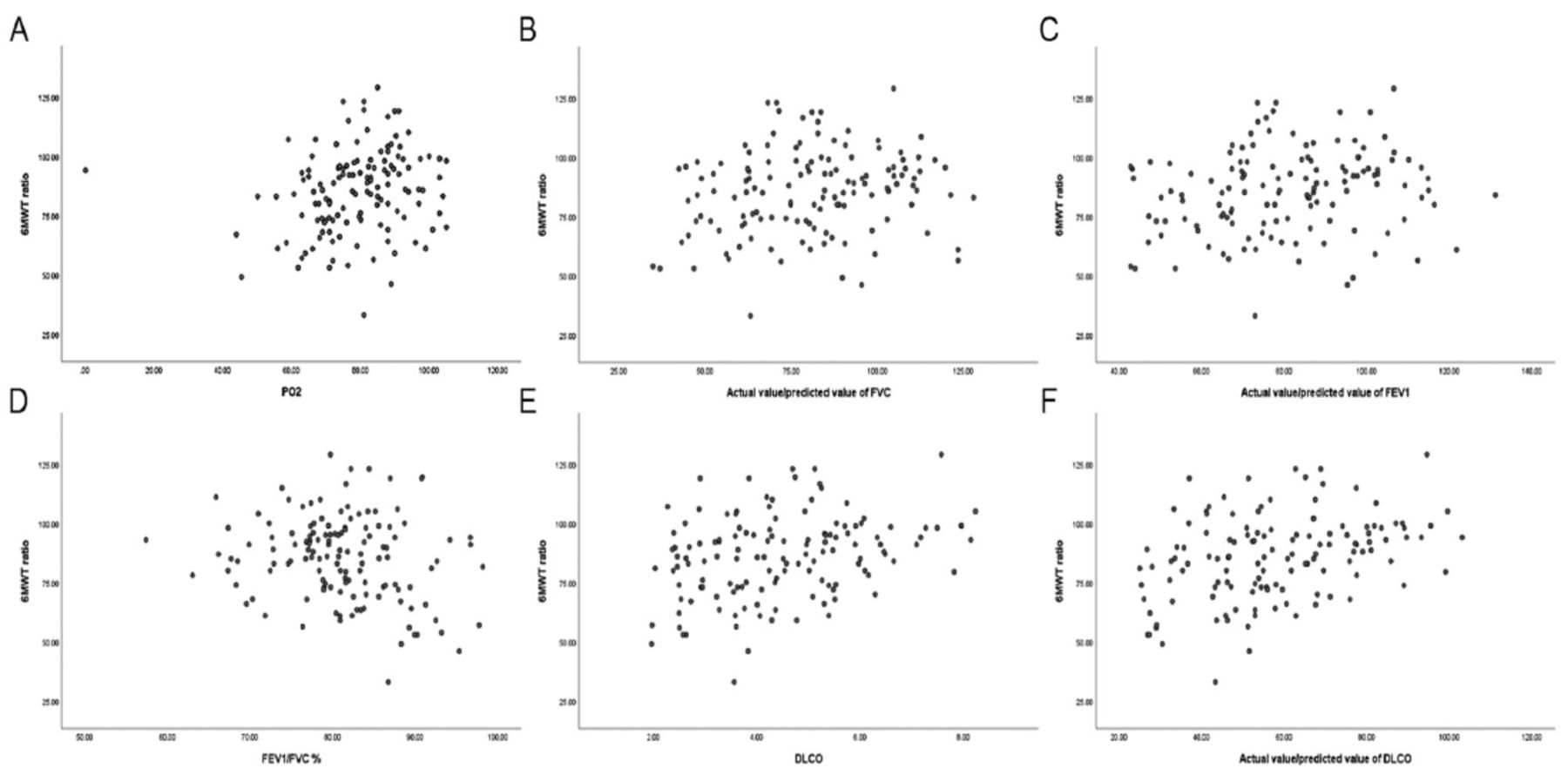
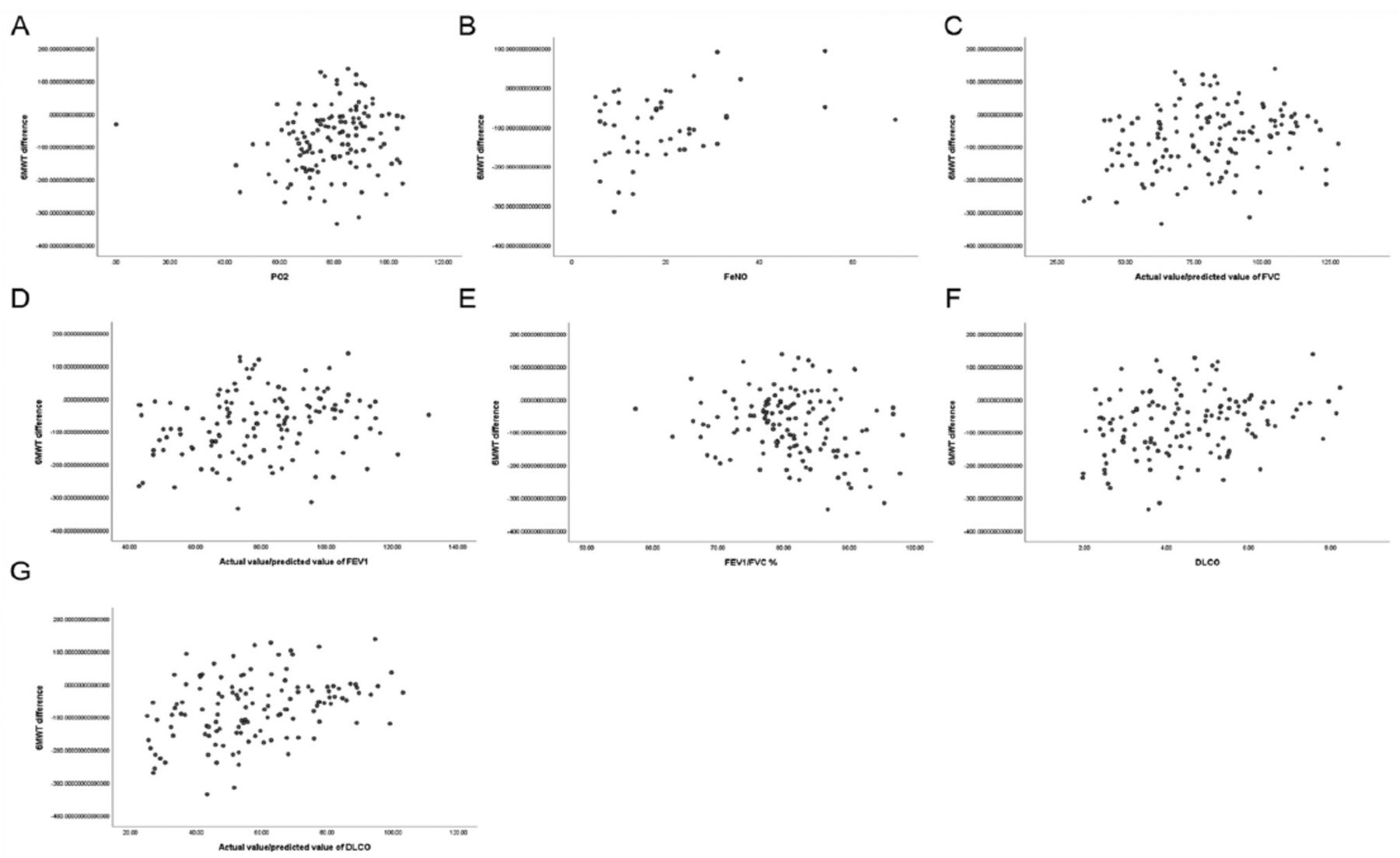
The 6MWT ratio was associated with PO2 (r=0.205, p=0.018), actual/predicted FVC (r=0.184, p=0.034), actual/predicted FEV1 (r=0.173, p=0.046), FEV1/FVC (r=-0.204, p=0.017), DLCO (r=0.303, p<0.001), and actual/predicted DLCO (r=0.355, p<0.001) (Figure 1). The 6MWT difference was associated with PO2 (r= -0.173, p=0.047), FeNO (r= -0.290, p=0.041), actual/predicted FVC (r= -0.203, p=0.019), actual/predicted FEV1 (r= -0.197, p=0.023), FEV1/FVC (r=0.202, p=0.018), DLCO (r= -0.273, p=0.001), and actual/predicted DLCO (r= -0.363, p<0.001) (Figure 2) (Table 2).

- Associations of 6MWT ratio with relevant variables. A) Associations of 6MWT ratio with PO2. B) Associations of 6MWT ratio with actual/predicted FVC. C) Associations of 6MWT ratio with actual/predicted FEV1. D) Associations of 6MWT ratio with FEV1/ FVC. E) Associations of 6MWT ratio with DLCO. F) Associations of 6MWT ratio with actual/predicted DLCO.

{kind=link}
{kind=link}
- Associations of 6MWT difference with relevant variables. A) Associations of 6MWT difference with PO2. B) Associations of 6MWT difference with FeNO. C) Associations of 6MWT difference with actual/predicted FVC. D) Associations of 6MWT difference with actual/predicted FEV1. E) Associations of 6MWT difference with FEV1/FVC. F) Associations of 6MWT difference with DLCO. G) Associations of 6MWT difference with actual/predicted DLCO.
- Associations of 6MWT difference and 6MWT ratio with relevant variables.
Multivariable analysis
Multivariable analysis showed that FeNO (β=-2.157, standard error (SE)=0.836, p=0.014) and DLCO (β=-22.528, SE=7.48, p=0.004) had independent associations with 6MWT difference (Table 3). In addition, FeNO (β=0.403, SE=0.163, p=0.018) and DLCO (β=4.355, SE=1.458, p=0.005) had independent associations with 6MWT difference (Table 4).
- Multivariable linear regression analysis of 6MWT difference.
- Multivariable linear regression analysis of 6MWT ratio.
Discussion
Although the 6MWT is a straightforward measure, it is influenced by several factors, including height, fat mass, and age, and formulas were developed to predict 6MWT value after correction for such factors.14 It’s value can be used as a surrogate for exercise capacity and cardiovascular reserve in cases affected by multiple disorders, including cardiovascular disorders and IPF.11 The 6MWT was mainly applied in idiopathic pulmonary fibrosis, the most common ILD. The 6MWT indexes are associated with the activities of daily living in IPF as well as with VO2max.15 Idiopathic pulmonary fibrosis is also correlated with reduced FVC, reduced FEV1, circulatory impairment, and peripheral muscle dysfunction, contributing to impaired physical function.16,17 In this study, 6MWT difference and ratio were associated with pulmonary function indicators in correlation and univariable logistic regression analyses, but not in multivariable analysis.
Diffusing capacity of the lungs for carbon monoxide represents the lung’s capability of transferring gas from inspired air to the blood. Therefore, low DLCO is a marker of impaired lung function.18 The 6MWT value is correlated with DLCO. Therefore, the 6MWT appears to better reflect maximal exercise capacity instead of submaximal capacity in patients with severely impaired lung function.15 In individuals with diffuse systemic sclerosis and ILD, the 6MWT and DLCO are related to and appear to be involved in desaturation events, indicating a higher mortality risk.19 Similar results have been reported in fibrotic interstitial pneumonia and ILD.20-22 In this study, a 6MWT ratio <1 or a negative 6MWT difference (actual 6MWT value lower than the predicted value) was related to reduced DLCO, indicating impaired pulmonary function in patients with ILD.
Previous clinical studies have revealed the 6MWT could help predict mortality in IPF.23-27 The present study could not examine mortality due to limitations of the available data and failed to observe an association between the 6MWT and hospital stay. Even though the length of hospital stay is considered a prognostic factor, it can be affected by several factors, including the cause of admission, disease severity, treatment effectiveness, comorbidities, self-discharge, transfer to other departments or hospitals, and death. Nevertheless, in the present study, no patient died during hospitalization.
Nitric oxide is secreted under inflammatory conditions and modulates vascular and bronchial tone.28 Fractional exhaled nitric oxide is often higher in patients with various pulmonary conditions but is not sensitive to condition changes over time.12,13 Fractional exhaled nitric oxide is generally used to determine the subtypes of asthma and COPD.29 In ILD, elevated FeNO indicates the requirement for systemic therapy, but a study showed no difference in FeNO levels between ILD cases and controls.30,31 Therefore, its use in ILD remains undefined. In the present study, a negative 6MWT difference was negatively correlated with FeNO, indicating a lower actual 6MWT value than the predicted value is correlated with high FeNO levels, suggesting enhanced inflammation with decreased exercise ability.
Study limitations
This retrospective analysis only examined clinical data in the patient charts of one hospital, with a small sample. Furthermore, ILD represents a heterogeneous class of lung conditions with different management approaches and prognoses. The available follow-up data did not allow us to examine mortality. Further larger prospective, multicenter, randomized, controlled studies are required to provide higher grades of evidence.
In conclusion, in patients with ILD, 6MWT difference and 6MWT ratio were associated with FeNO and DLCO. The 6MWT was not associated with hospital stay. The 6MWT value might be employed clinically to assess lung function in ILD.
Acknowledgment
We would like to thank MedSci (http://www.medsciediting.com/index.asp) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received June 24, 2023.
- Accepted August 31, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.