

ABSTRACT
Objectives: To identify and summarize studies carried out in Arab countries on anti-obesity medications (AOMs), with a focus on the types of medications investigated, study designs, and the efficacy/effectiveness and safety metrics reported.
Methods: We carried out a comprehensive scoping review of primary studies examining the use of AOMs in adult Arab populations. Five databases (Medline, Embase, Cochrane Library, Index Medicus for the Eastern Mediterranean Region, and e-Marefa) were searched for English-language publications up to October 2024. Data extraction was carried out on study characteristics, participant demographics, interventions, and outcomes related to weight reduction, metabolic parameters, and side effects. The risk of bias (RoB) was assessed using the Newcastle-Ottawa scale for non-randomized studies and a modified RoB tool for randomized controlled trials.
Results: A total of 59 clinical studies published between 2014-2024 were included. The majority (89.8%) were observational in design. Most studies were carried out in Saudi Arabia (40.7%) and the United Arab Emirates (20.3%). Glucagon-like peptide-1 receptor agonists were investigated in 72.9% of the studies, with liraglutide being the most frequently studied agent (54.2%). The most commonly reported efficacy outcomes included changes in total body weight (45.8%), body mass index (39.0%), and the proportion of weight loss (28.8%). Gastrointestinal side effects were reported in 32.2% of patients across studies.
Conclusion: Despite the growing body of research on AOMs in Arab countries, most studies remain observational and focus primarily on earlier-generation agents. There is a need for randomized controlled trials to evaluate the efficacy and safety of newer AOMs, such as semaglutide and tirzepatide, within Arab populations to inform culturally and genetically tailored obesity management strategies.
Obesity affects approximately 2.5 billion adults globally and presents a significant public health challenge. The Middle East, particularly Saudi Arabia, has a notable prevalence of overweight/obesity, with 38% of adults being overweight and 20% being obese, as reported in a 2019 World Health Organization (WHO) survey.1,2 Obesity not only predisposes individuals to a range of serious health issues, including metabolic and cardiovascular diseases but also imposes a significant economic burden.3,4 The etiology of obesity is complex and influenced by genetic, environmental, behavioral, and sociocultural factors, which complicates its management.5,6
Arab populations exhibit a distinct genetic susceptibility to obesity, likely exacerbated by consanguinity, which is highly prevalent in many Arab countries. A systematic review identified 76 genetic variants associated with obesity in these populations, of which 2 are unique, and 19 show specific associations compared with non-Arab groups.7-9 These genetic variants can significantly influence drug metabolism by altering the activity of drug-metabolizing enzymes, leading to variations in drug efficacy and toxicity.8,10-12
The United States (US) Food and Drug Administration (FDA) has approved various pharmacotherapies, such as liraglutide and semaglutide, which, when integrated with lifestyle modifications, can be very effective in reducing body weight.13,14 However, the specific impact of these medications on the Arab population requires further investigation to ensure optimal treatment efficacy.15 Despite the relatively early stage of obesity pharmaceutical research in Arab countries, there is an increasing focus on this area. Effective pharmacotherapy, which is essential for managing obesity where lifestyle modifications alone are insufficient, must be adapted to the unique genetic and environmental contexts of Arab populations to improve long-term outcomes.15
With this scoping review, we aimed to provide a comprehensive description of the body of evidence on the use of anti-obesity medications (AOMs) among adults in the Arab world. The results of this scoping review will help inform future research initiatives in the Arab world.
Objectives
To summarize the characteristics of the studies carried out in Arab countries such as the type of medication, the research setting, the duration of intervention investigated, the primary outcome reported, and to compare these characteristics across studies by type of AOM. Additionally, we aimed to assess the diversity of study designs and methodologies used in this research area, and to identify and map all relevant medications.
Methods
We adhered to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) extension for scoping reviews statement.16
Eligibility criteria
We included clinical studies examining the use of AOMs in adults within Arab countries. We included studies of any design except narrative, systematic reviews, clinical guidelines, correspondence, or studies investigating irrelevant interventions. We excluded studies on participants under the age of 18, non-Arab populations, and multi-site clinical studies initiated outside Arab countries.
Information sources and search strategy
We systematically searched 5 databases: Ovid Medline, Embase, the Cochrane Library, Index Medicus for the Eastern Mediterranean Region, and e-Marefa. The search strategy was developed using key concepts related to our research objective: the use of AOMs in Arab countries. These concepts included AOMs, overweight, obesity, and weight management interventions in adult populations within the Arab world (Algeria, Bahrain, Comoros, Djibouti, Egypt, Iraq, Jordan, Kuwait, Lebanon, Libya, Mauritania, Morocco, Oman, Palestine, Qatar, Saudi Arabia, Somalia, Sudan, Syria, Tunisia, the United Arab Emirates [UAE], and Yemen). We employed Medical Subject Headings (MeSH) terms and Boolean operators to ensure comprehensive coverage of the literature. The search was limited to English-language studies and included publications from inception through October 2024. Further details of the search strategy are shown in Appendixes 1 & 2.
Study selection
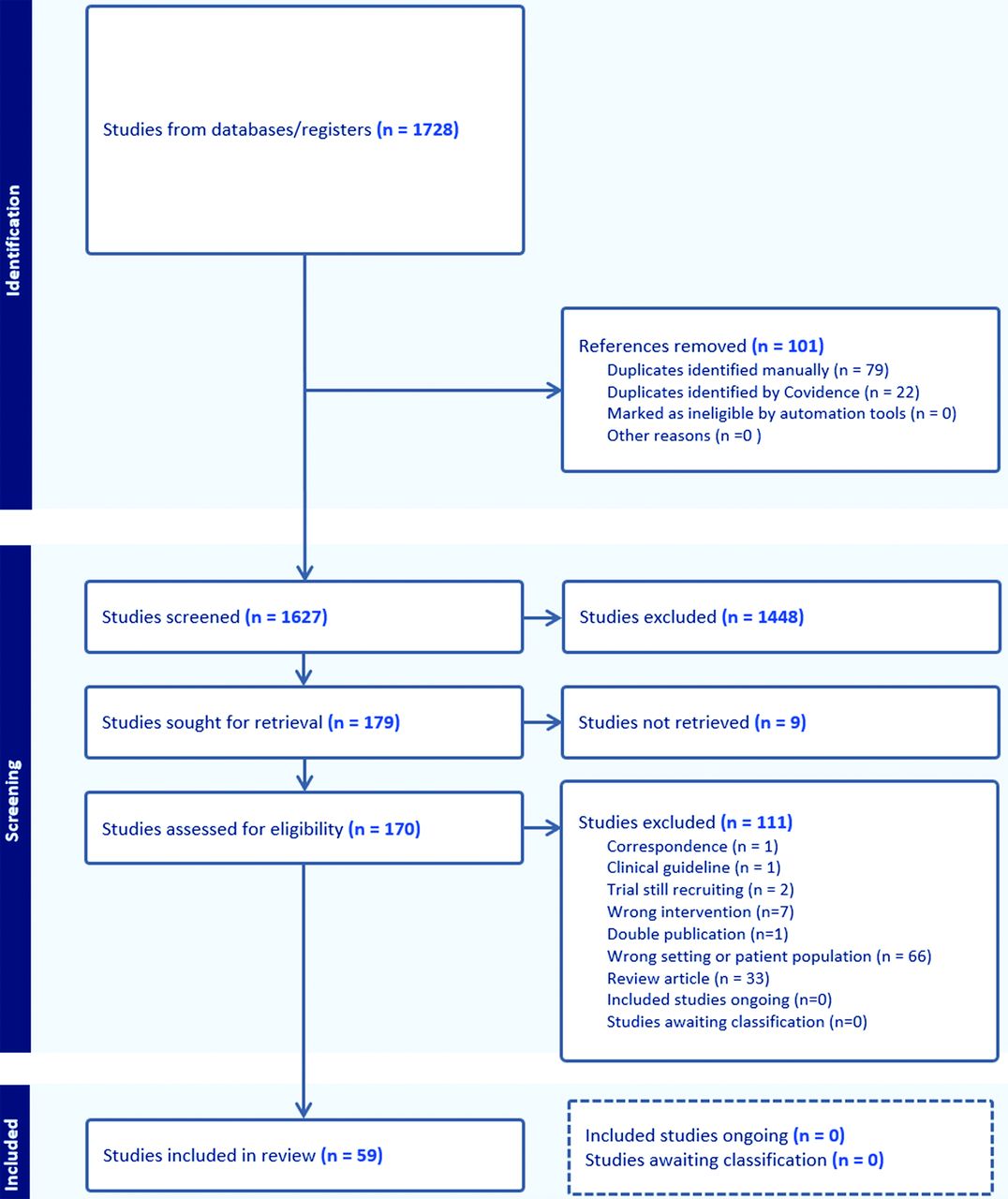
Reviewers used the Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia) to organize and facilitate the study selection process.1 Two reviewers, independently and in duplicate, screened the titles and abstracts of the identified studies, excluding irrelevant studies. Subsequently, 2 independent reviewers assessed the full texts of potentially eligible articles and extracted relevant data from the eligible studies. Any disagreements among the reviewers were resolved by a third reviewer. The PRISMA flow diagram outlining the study selection process is presented in Figure 1.

- The Preferred Reporting Items for Systematic reviews and Meta-Analyses flowchart diagram showing the study selection steps.
Data extraction
Two authors independently extracted data using a standardized, predesigned data extraction form. The extracted data included study characteristics (author, publication year, study design, and sample size), participant demographics and baseline characteristics (country, percentage of female participants, mean age, and population/diagnosis), intervention details (type of AOM, dosage, duration, route of administration, and frequency of administration), and information on which outcome metrics were reported.
Outcome measures
Our scoping review focused on identifying which outcomes were reported in the included studies. These outcomes included but were not limited to weight-related measures (for example, change in total body weight [TBW], body mass index [BMI], waist circumference [WC], metabolic parameters [namely, blood glucose levels, lipid profiles, and blood pressure], and side effects associated with AOMs). For side effects, this review collected the proportion of patients experiencing gastrointestinal (GI) symptoms in studies that reported them. Gastrointestinal side effects were defined as any GI-related symptoms reported. Gastrointestinal side effects with additional symptoms were defined if any additional symptoms were reported, such as headache or fatigue. Serious complications were defined as acute pancreatitis, intragastric balloon migration leading to small bowel obstruction (SBO), or other serious complications, as specified by the study’s authors. The outcome measures were documented and categorized pragmatically by merging similar outcomes into broader categories to facilitate reporting (namely, patient-reported outcomes [PROs], biomarkers and biochemical effects, cardiometabolic outcomes, health behaviors/practices, and health economics).
Risk of bias assessment
For non-randomized studies, we utilized the Newcastle-Ottawa scale (NOS) to assess the risk of bias (RoB).17 This scale evaluates studies based on the selection of the study groups, comparability of the groups, and ascertainment of the outcome/exposure.17 For randomized controlled trials (RCTs), we applied the revised Cochrane risk-of-bias tool for randomized trials (RoB 2), assessing domains such as randomization, deviations from intended interventions, missing data, measurement of outcomes, and selection of the reported result.18 The risk of bias assessment was carried out independently and in duplicate by 2 reviewers. Each domain was rated to provide a comprehensive evaluation of the RoB for each study. Discrepancies between reviewers were resolved through discussion and consensus or by consulting a third reviewer if necessary.
Data synthesis
We summarized and presented the data descriptively according to the type of medication, country, duration of the intervention, and the outcomes reported. We evaluated the diversity of study designs and methodologies used in research carried out on the use of AOMs.
Statistical analysis
Descriptive statistics were used to summarize the data. For categorical variables, absolute frequencies and percentages (%) were calculated, whereas continuous variables were summarized using medians with interquartile ranges (IQRs) and range values. Statistical analyses were carried out using the statistical Package for the Social Sciences, version 29.0 (IBM Corp., Armonk, NY, USA). For quantifying the frequency of AOMs studied, some studies were counted more than once if they included multiple types of AOMs to provide a comprehensive overview of the medications studied.
Results
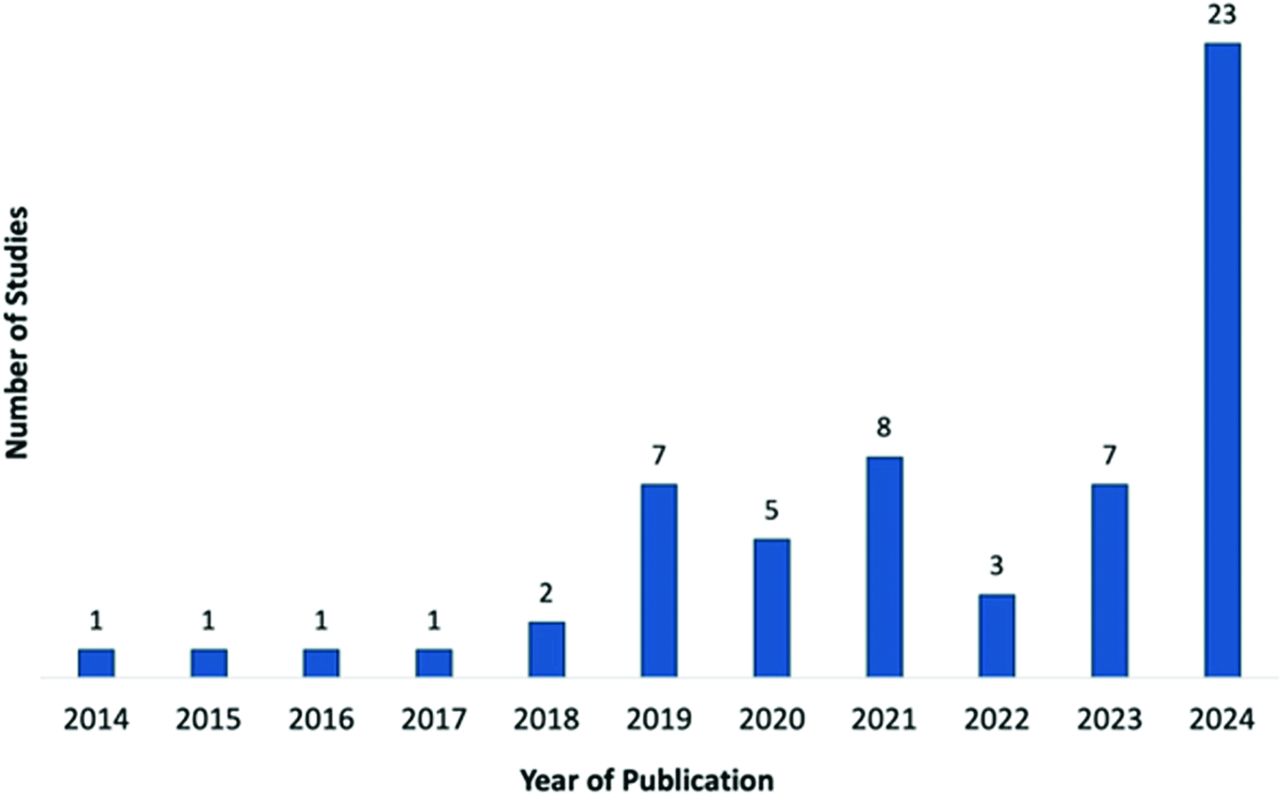
Out of 1627 titles, 170 were assessed for eligibility, 111 were excluded for various reasons (Figure 1), and 59 studies met our eligibility criteria and were included. Eligible studies were published between 2014-2024 (Figure 2). Among these, 12 studies (20.3%) were published as abstracts and 47 studies (79.7%) were published as full texts.20-78 The detailed characteristics of these studies are provided in Table 1.

- Anti-obesity medication study counts by year of publication (N=59).
- Characteristics of the studies included in this scoping review.
The 53 observational (non-randomized) studies accounted for 89.8% of the total, with 11 (18.6%) studies including control arm (6 observational and 5 RCTs). Most studies originated from Saudi Arabia (39%) and the UAE (20.3%, Table 2). Funding was reported in 22.0% of the studies. The median sample size was 91 (IQR: 50-180), with a median participant age of 43.0 years (IQR: 37.7-48.0). The median proportion of females in the included studies was 71.0% (IQR: 55.2-81.0%).
- Summary of included studies overall and by type of anti-obesity medications evaluated (N=59).
The primary outcomes that were reported across eligible studies were changes in TBW (45.8%), BMI (39.0%), weight loss proportion (28.8%), and WC (6.8%). Approximately 36% of the studies reported multiple anthropometric measures. Cardiometabolic outcomes included changes in hemoglobin A1c (HbA1c, 20.3%) and lipid profile (10.2%).
Risk of bais assessments, where applicable (excluding abstracts and cost-effectiveness analyses), revealed that among the 41 observational (non-randomized studies), 53.7% had moderate RoB, 2.4% low RoB, and 43.9% high RoB. Four of the 6 (66.7%) RCTs were classified as having high RoB, and 2 (33.3%) were classified as having low RoB. Details on the study characteristics, interventions, and outcomes can be found in Tables 1 & 2.
Figure 3 displays a geographic heatmap that visualizes the distribution of AOM clinical studies across the Arab world, providing insight into the regional variation in research activity related to AOMs.

- Geographic heatmap of included anti-obesity medication study count in the Arab world (N=59).
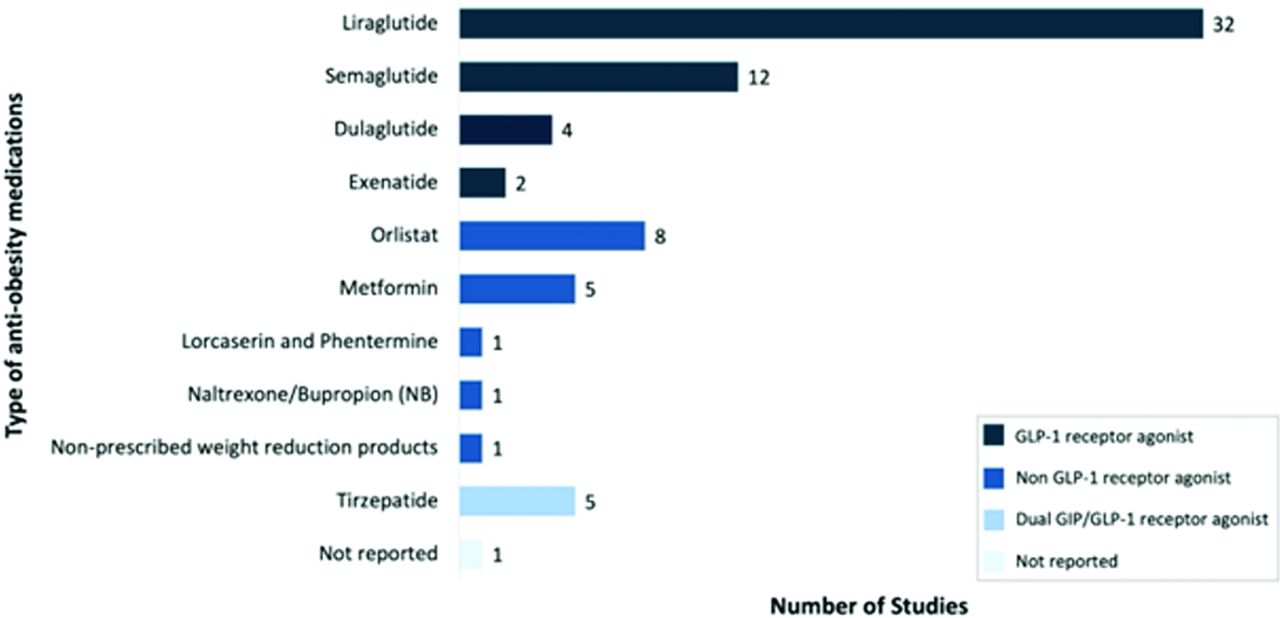
Glucagon-like peptide-1 (GLP-1) receptor agonists were investigated in 43 (72.9%) studies (Figure 4), with liraglutide being the agent used in 54.2% of all studies. Other GLP-1 receptor agonists included semaglutide (20.3%), dulaglutide (6.8%), and exenatide (3.4%). Tirzepatide (dual glucose-dependent insulinotropic polypeptide [GIP]/GLP-1 agonists) was used in 8.5% of the studies. Orlistat (13.6%) and metformin (8.5%) were among the non-GLP-1 agents studied. Naltrexone/bupropion and lorcaserin/phentermine were each used in one study. In studies investigating GLP-1 receptor agonists only, TBW was reported in 56.4%, BMI in 35.9%, and weight loss proportions in 33.3%. Changes in HbA1c were reported in 25.6% and the lipid profile in 5.1% of GLP-1 studies. Studies of dual GIP/GLP-1 agonists reported TBW (40.0%) and weight loss proportions (40.0%). Non-GLP-1 studies reported BMI (58.3%), TBW (25.0%), weight loss proportion (16.7%), WC (16.7%), HbA1c (8.3%), and lipid profile (33.3%).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
- Number of included studies by type of anti-obesity medications (N=59). Some studies were counted more than once because they included multiple types of anti-obesity medication. GIP: glucose-dependent insulinotropic polypeptide, GLP-1: glucagon-like peptide-1
Whether patients experienced GI side effects with additional symptoms was reported in 15.3% of the studies; reporting of GI side effects with serious complications was reported in 6.8% (exclusively among GLP-1 receptor agonist studies). Overall, 78.0% of the studies were published between 2020-2024, with all dual GIP/GLP-1 studies published in 2024. Cohort studies represented 74.4% of GLP-1 studies, 60.0% of dual GIP/GLP-1 studies, and 41.7% of non-GLP-1 studies. Among non-GLP-1 studies, 41.7% were RCTs. Saudi Arabia carried out 48.7% of GLP-1 studies. All dual GIP/GLP-1 studies were from the UAE (60.0%) and Kuwait (40.0%). Among the GLP-1 studies, 46.2% of the population focused on individuals with obesity only, while 20.5% specifically evaluated those with type 2 diabetes only. Other studies included participants with both obesity and type 2 diabetes, or combined these conditions with others, such as bariatric surgery, dyslipidemia, or metabolic dysfunction-associated steatotic liver disease (MASLD).
Discussion
The current scoping review examines the evidence surrounding the use of AOMs in clinical practice in Arab nations. Most of the studies included were retrospective observational cohort studies, whereas only 6 were RCTs, all of which were non-GLP-1 AOM studies. Globally, research on AOMs is more extensive, with numerous funded high-quality RCTs demonstrating their efficacy and safety.79,80 This discrepancy could be attributed to many challenges in carrying out high-quality RCTs among Arab countries, including inadequate research resources such as limited funding opportunities, an underdeveloped regulatory framework, inadequate research facilities, and a lack of skilled personnel.81,82 Despite the limitations of the currently available knowledge in the literature from Arab countries, the number of included publications has notably increased since 2018, highlighting the growing positive clinical attitudes toward treating obesity. The marked increase in publications between 2020-2024 may reflect a surge in clinical and research interest in AOMs across Arab countries. This could be attributed to the global momentum following recent regulatory approvals of newer agents, such as semaglutide and tirzepatide, growing public awareness, and increased availability of these therapies in the region.
Most of the studies included in this scoping review were carried out in Saudi Arabia, followed by the UAE. Similar to global findings, the majority of the participants in the studies in this review were females with obesity, and most did not have diabetes.13,83 This female predominance reflects the higher prevalence of obesity observed in women globally.84
A total of 43 (72.9%) studies investigated GLP-1 receptor agonists, primarily administered subcutaneously. Liraglutide was most common, followed by semaglutide, dulaglutide, and exenatide. By comparison, oral AOMs have been studied less frequently. This aligns with global reviews emphasizing GLP-1 receptor agonists as a frequent research focus.85
Studies included in this review also evaluated several non-GLP-1 receptor agonists, including orlistat (8 studies), lorcaserin, phentermine, metformin, and naltrexone/bupropion aligning with their reported use in literature from Arab countries.83,86 This difference can be attributed to several factors, such as the non-availability of many non-GLP-1 receptor analogs, limited access to AOMs in public hospitals, limited knowledge among healthcare providers, and a limited number of obesity specialists.87 Although this review revealed orlistat to be the most frequently studied non-GLP-1 AOM, global guidelines generally discourage its use as a first-line therapy due to its GI side effects.88 Similar to global studies, only a few studies in this review investigated the combination of GLP-1 and non-GLP-1 receptor agonists.83,86,87
This scoping review identified weight loss proportion, change in TBW and BMI, and WC as the primary outcomes for evaluating weight loss across the included studies. In contrast, TBW was the most frequently reported outcome in studies investigating GLP-1 receptor agonists (approximately half), studies focusing on non-GLP-1 receptor agonists more often utilized BMI. Using different ways to measure outcomes makes it difficult to compare treatments and may hide true differences in how well they work.
Approximately one-third (35.6%) of studies, mostly those evaluating GLP-1 receptor agonists, incorporated multiple anthropometric measures, with fewer reporting visceral fat indices (namely, visceral adiposity index). These findings are consistent with systematic reviews highlighting TBW as a frequent measure of obesity, whereas others emphasize BMI and WC as primary efficacy measures for both AOM classes.15,89,90 Improvement across various anthropometric parameters is a recognized surrogate for reduced obesity-related morbidity and mortality.83
Cardiometabolic indices such as lipid profiles, HbA1c, and blood pressure are established surrogates for assessing obesity-related mortality risk.91 A significant portion of studies, primarily those investigating GLP-1 receptor agonists, reported cardiometabolic measures, most commonly HbA1c reduction. This aligns with global AOM reviews.92
Liraglutide was the most frequently prescribed AOM in this review, which is consistent with its high efficacy and frequent use in obesity clinics.89 Semaglutide was the next most common GLP-1 receptor agonist, which is also supported by other reviews.89 Notably, recent US data indicate a substantial increase in semaglutide prescriptions.93 Additionally, tirzepatide, a dual GIP/GLP-1 receptor agonist, has gained prominence following USFDA approval in 2023 for weight management in adults with obesity or overweight and has demonstrated robust efficacy in RCTs.93-95
However, this review identified only 5 tirzepatide studies, primarily cohort studies from the UAE and Kuwait published in 2024, which contrasts with international research in which tirzepatide has been investigated in multiple RCTs.85
There are several new medications in phase 2 trials, including dual and triple hormone receptor agonists, which have shown promising early results for treating obesity. One example is retatrutide, a triple agonist targeting GLP-1, GIP, and glucagon receptors, which demonstrated statistically significant weight loss (22.8-24.2%) and metabolic improvements in systolic and diastolic blood pressure and levels of glycated hemoglobin, fasting glucose, insulin, and lipids in a 48-week phase 2 trial, highlighting its potential for future obesity management.96
Researchers have compared the safety and tolerability of GLP-1 and non-GLP-1 receptor agonists. While serious GI side effects are more common with GLP-1 receptor agonists, the overall incidence of serious side effects is similar between groups.81,84 However, this review identified a significant gap in the reporting of such side effects. Only 15.3% of included studies reported whether patients experienced GI side effects with additional symptoms, and 6.8% serious GI complications like pancreatitis and severe nausea and vomiting (exclusively in studies of GLP-1 receptor agonists).
The study offered a comprehensive evaluation of scientific literature surrounding AOMs in Arab populations, highlighting several key elements. The study emphasizes the importance of addressing obesity as a public health priority. The distinct genetic susceptibilities among Arab populations may necessitate tailored pharmacotherapy approaches. The predominance of observational studies indicates a significant gap in high-quality RCTs. This suggests a need for more rigorous research to validate the efficacy and safety of AOMs in this demographic. The emphasis on older AOMs such as liraglutide suggests that newer options like semaglutide and tirzepatide are under-researched. A network meta-analysis comparing various GLP-1 receptor agonists (23 RCTs, N=11,545) demonstrated the superior efficacy of newer agents like semaglutide (2.4 mg) for weight loss compared to older options such as liraglutide (3.0 mg), although all GLP-1 RAs outperformed placebo.97 Therefore, investigating these newer medications in Arab countries could lead to improved treatment outcomes. The barriers to carrying out high-quality research, such as limited funding and resources, point to a broader issue within Arab healthcare systems. Addressing these challenges could promote better obesity management strategies. In summary, this study highlights the need for more targeted research on AOMs in Arab populations, emphasizes the importance of understanding genetic and environmental factors, and calls for improved healthcare resources to address the obesity epidemic effectively.
Study’s strengths & limitations
This study revealed significant gaps in the literature and unmet needs in obesity management for the Arab population.
We acknowledge several limitations. Most evidence comes from non-Arabic literature, with limited data from the Middle East. Additionally, studies from non-Arab sources may differ in their methodologies, populations, or inclusion criteria, which may limit comparability and generalizability to the Arab context. The studies we reviewed were mainly observational with moderate to high RoB, indicating the need for well-designed, larger, randomized trials to determine their efficacy and safety. Notably, there is a lack of rigorous high-quality studies on novel AOMs, such as semaglutide and tirzepatide, in the region. Additionally, our focus on studies initiated within Arab countries may limit comparative insights from broader, internationally initiated research.
In conclusion, the current scoping review emphasizes the need for targeted, high-quality research to inform evidence-based strategies for obesity management in Arab countries. Notably, there is a lack of sufficient studies in this region, with existing research often being limited in number, of low quality, and inconsistent in reporting key outcomes. Future research should focus on improving study quality, standardizing methodologies, the adoption of a standard outcome measure, and expanding representation to improve our understanding of the efficacy and safety of AOMs in this region. By addressing these areas, future research can significantly improve obesity management and inform policy development tailored to the unique genetic and socio-cultural context of Arab societies.
Acknowledgment
The authors gratefully acknowledge the Scientific Publishing Department, Health Research Center, Ministry of Defense Health Services, Riyadh, Saudi Arabia, for the English language editing.
Appendix
- Literature search of anti-obesity medications in Arab countries - SR (Embase 1974-2024 October 04, Ovid MEDLINE(R) ALL 1946-October 04, 2024).
Appendix
- Literature search of anti-obesity medications in Arab countries - SR the Cochrane Library (CENTRAL).
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 3, 2025.
- Accepted April 13, 2025.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.
- 65.
- 67.
- 68.
- 69.
- 70.
- 71.
- 72.
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.
- 88.
- 89.
- 90.
- 91.
- 92.
- 93.
- 94.
- 95.
- 96.