

ABSTRACT
Objectives: To investigate the association between thyroid-stimulating hormone (TSH) levels and lipid profiles in patients with subclinical hypothyroidism (SCH) to assess the metabolic risks.
Methods: This retrospective study included patients diagnosed with SCH between January 2023 and August 2024. Thyroid function markers (TSH, free triiodothyronine, and free thyroxine levels) and lipid profiles (total cholesterol, low-density lipoprotein, high-density lipoprotein, and triglyceride levels) were assessed in 137 patients.
Results: The mean age of patients was 44.6±13.6 years, with 86.1% being female and 92.7% having dyslipidemia. Thyroid-stimulating hormone levels were correlated with serum creatinine levels (r=0.27, p=0.001) and showed a non-significant trend toward higher cholesterol levels (r=0.15, p=0.09). Free thyroxine were significantly lower in women (p=0.035) and in patients with hypertriglyceridemia (n=32; p=0.005), showing an inverse correlation (r= -0.2; p=0.02). Free triiodothyronine were lower in patients with obesity (p=0.003) and inversely associated with body mass index (BMI, r= -0.2, p=0.019). Serum creatinine levels independently predict TSH levels, whereas triglyceride levels inversely predict free thyroxine levels.
Conclusion: Subclinical hypothyroidism impairs lipid metabolism, particularly in females with high BMI. Triglycerides suppress free thyroxine levels, whereas elevated TSH levels correlate with increased creatinine levels. Our findings suggest a potential relationship between SCH and lipid alterations, warranting further investigation into targeted lipid management in these patients.
Subclinical hypothyroidism (SCH) is characterized by a mild elevation in serum thyroid-stimulating hormone (TSH) levels, with thyroid hormones, including thyroxine (T4) and triiodothyronine (T3), remaining in normal circulation. Although SCH is considered an early or mild form of hypothyroidism, it is often associated with metabolic disturbances, particularly dyslipidemia.1 The impact of SCH on lipid metabolism is of critical concern because of its effects on cardiovascular (CV) risk. Thyroid hormones play significant roles in lipid synthesis, mobilization, and degradation, and even minor fluctuations can disrupt normal lipid homeostasis.2
Minor alterations in the thyroid function can significantly affect lipid metabolism. Reduced thyroid hormone levels are strongly associated with increased total cholesterol, low-density lipoprotein (LDL), and triglyceride levels as well as decreased high-density lipoprotein (HDL) levels.3 Although SCH is less severe, it may alter lipid profiles, potentially increasing the risk of atherosclerosis and CV disease (CVD).4,5 It is assumed that the reduced activity of LDL receptors, lipoprotein lipase, and changes in cholesteryl ester transfer proteins contribute to lipid metabolism abnormalities in patients with SCH.6 Notably, in hypothyroidism, reduced hepatic expression of LDL receptor - related protein 1 is associated with the impaired clearance of circulating residual lipoproteins.7
Patients with SCH have an increased prevalence of dyslipidemia.8 However, the results on lipid alterations have been inconsistent, ranging from minimal to significant changes.9 These variations may be due to differences in the study populations, diagnostic criteria for SCH, and sample sizes. Despite these discrepancies, growing evidence suggests that SCH is not benign, especially considering its long-term effects on lipid metabolism and CV health.10 As an atherogenic disease, SCH increases the CV risk, highlighting the necessity of assessing lipid profiles in affected patients.11
In populations with frequent thyroid disorders, the potential role of SCH in exacerbating dyslipidemia merits further investigation. Given the worldwide increase in metabolic disorders and the identification of thyroid dysfunction as a contributing factor, a deeper understanding of the relationship between SCH and lipid abnormalities is essential.12 Early detection and management of dyslipidemia in patients with SCH may be pivotal for mitigating CV risks and enhancing long-term health outcomes.13
This study aimed to investigate the lipid profile alterations in patients with SCH and determine the clinical implications of these changes.
Methods
This study included 137 patients diagnosed with SCH at the Endocrinology Clinic, Internal Medicine Department, King Abdulaziz University, Jeddah, Saudi Arabia, a tertiary care center. Subclinical hypothyroidism was defined as increased serum TSH level (>4.5 mIU/L) with normal free T4 (FT4).14 Patients with a history of thyroid disease, dyslipidemia, CVD, diabetes, or other comorbidities were excluded.
This study was approved by the institutional ethics committee of King Abdulaziz University, Jeddah, Saudi Arabia (HA-02-J-008), and informed consent was obtained from all participants.
Demographic and clinical characteristics, including age, gender, body mass index (BMI), family history, and medication use, were documented from medical recorded. Fasting blood samples were measured for serum TSH (normal: 0.27-4.2 uIU/mL), FT4 (normal: 12-22 pmol/L), free T3 (FT3, normal: 2-7 pmol/L), total cholesterol (normal: <5.17 mmol/L), HDL-C (normal: >1.55 mmol/L), LDL-C (normal: <2.6 mmol/L), and triglyceride levels (normal: <1.69 mmol/L).
Statistical analysis
The Statistical Package for the Social Sciences, version 27.0 (IBM Corp., Armonk, NY, USA) was used. Continuous variables are expressed as mean ± standard deviation (SD), and categorical variables as frequencies and percentages (%). Spearman’s correlation analysis was used to examine the relationship between the TSH levels and lipid parameters. Multiple linear regression analysis was used to evaluate the independent association between TSH and lipid profiles while adjusting for possible confounding variables. A receiver operating characteristic (ROC) curve was plotted to verify the ability of the thyroid hormone profiles to detect dyslipidemia. Statistical significance was set at a p-value of <0.05.
Results
The mean age of the patients was 44.6±13.6 years. The cohort included 118 women (86.1%) and 19 men (13.9%, F:M 6.2:1). Among these, 91 were Saudi and 46 were non-Saudi patients. Patient characteristics are presented in Table 1. Only one patient had an elevated creatinine level (120 µmol/L), whereas 6 (4.4%) had systolic blood pressure (SBP) and 11 (8.03%) had diastolic BP (DBP). The thyroid profiles according to gender, BMI, and dyslipidemia are shown in Table 2. Free T3 levels were significantly higher in obese patients. The TSH levels tended to be higher in patients with hypercholesterolemia. No significant differences in TSH (p=0.66), FT3 (p=0.26), and FT4 (p=0.14) levels were observed between Saudi and non-Saudi patients.
- Characteristics of the patients with subclinical hypothyroidism (N=137).
- Thyroid profile according to the gender, body mass index grade, and dyslipidemia in patients with subclinical hypothyroidism (N=137).
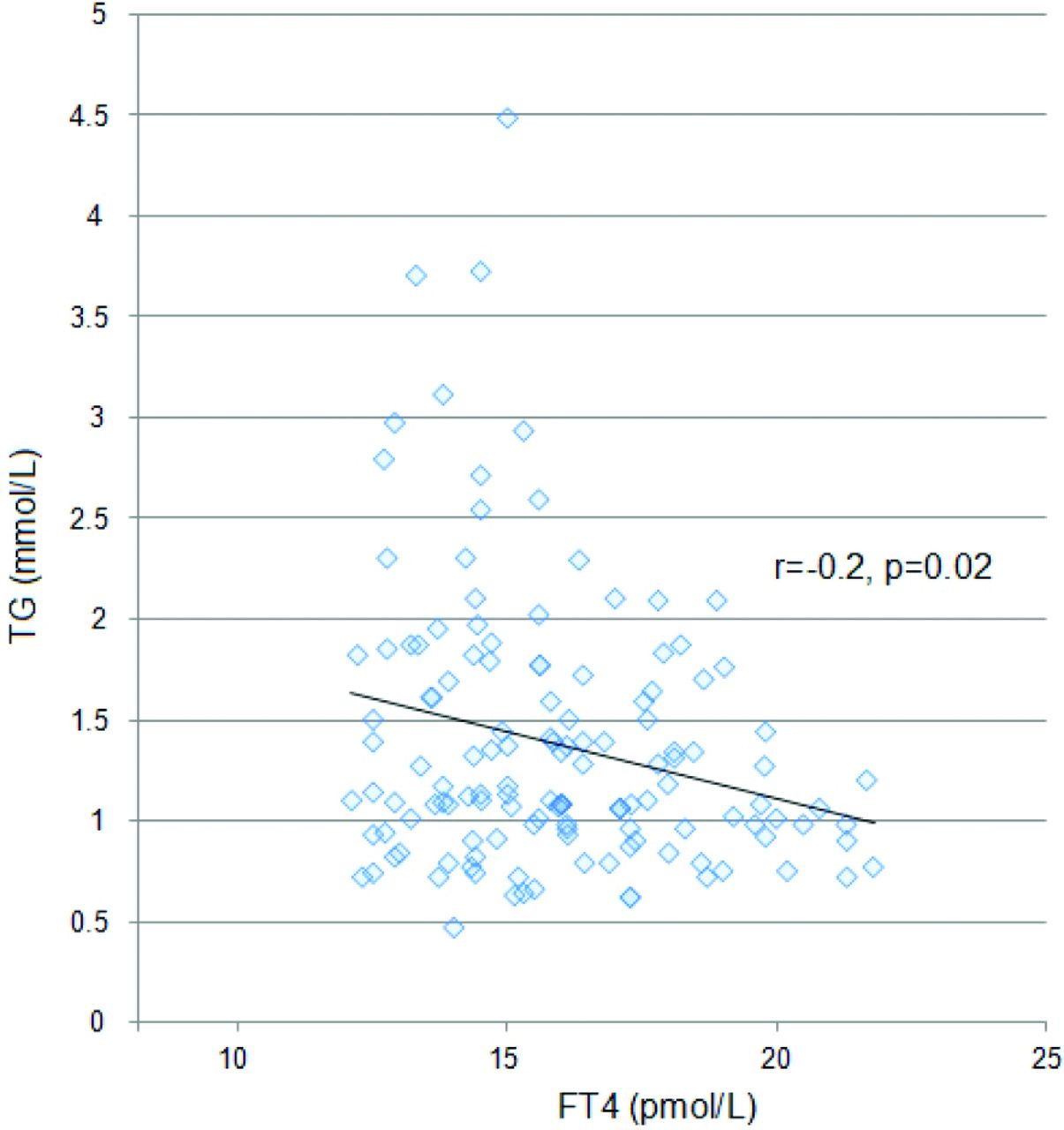
Correlations among thyroid hormone profiles, various manifestations, and lipid profiles are presented in Table 3. The FT4 levels were significantly associated with triglyceride levels (Figure 1). The FT3 and FT4 levels were significantly correlated (r=0.27, p=0.002).

{kind=link}
- Correlation of free thyroxine with triglycerides in patients with subclinical hypothyroidism. FT4: free thyroxine, TG: triglyceride.
- Correlation of the thyroid profile hormones with age, body mass index, blood pressure, serum creatinine, and lipid profile in patients with subclinical hypothyroidism (N=137).
Linear regression analysis showed that serum creatinine (b=0.33, p=0.001) was the only significant predictor for TSH level, regardless of confounding factors including age, BMI, BP, and lipid profile. Only triglycerides negatively predicted FT4 levels (b= -0.22, p=0.016). Age (b= -0.31, p=0.001) and cholesterol levels (b=0.33, p=0.02) significantly influenced FT3 levels.
Receiver operating characteristic curve analysis showed poor area under the curve for TSH (0.43, p=0.49), FT3 (0.59, p=0.32), and FT4 (0.45, p=0.57) in detecting dyslipidemia.
Discussion
Thyroid hormones regulate lipid metabolism, and hypothyroidism causes hypercholesterolemia and hypertriglyceridemia. Both overt and SCH are associated with hypercholesterolemia, hypertriglyceridemia, insulin resistance, metabolic syndrome, and an increased risk, necessitating timely diagnosis and management, particularly in young women.15-17 A meta-analysis confirmed the association between SCH and dyslipidemia, necessitating proper clinical management to prevent dyslipidemia and related conditions.18 Given that SCH is asymptomatic, regular screening for thyroid disorders is crucial for the management of thyroid disease.11
In this study, 137 patients with SCH were predominantly females (86.1%) in their fifth decade of life. Furthermore, FT3 levels were significantly inversely related to patient age, whereas FT4 levels were significantly lower in female patients than in males. Total cholesterol, triglyceride, and LDL-C levels were associated with TSH levels in patients in their eighth decade; however, this association weakened beyond 80 years.19 Subclinical hypothyroidism is more prevalent in women with the last menopause at <45 years.20 In SCH, CV mortality increases in patients aged <65 years.21 The distributions of SCH and TSH increasingly shift toward higher concentrations with age.22 An age-specific reference range for TSH levels can prevent overdiagnosis of SCH in older adults. Aging can reduce the effects of TSH on lipid profiles.19 Increasing evidence suggests that TSH concentrations are higher at the extremes of life.23 Subclinical hypothyroidism is common in females, reproductive age groups, and older adults.11 Following this increase, a study in Nepal reported that 71.8% of patients with SCH were women.16 Women with SCH show increased total cholesterol level ≥45 years of age.24 Moreover, in another study from China, SCH was linked to older age and obesity, as indicated by a high BMI and a significant increase in the prevalence of dyslipidemia, including higher grades of triglycerides, total cholesterol, and LDL.25 Another study from Saudi Arabia with a smaller number of patients determined a substantial relationship between SCH and lower HDL levels and higher TG and LDL levels.26 In a study carried out in Morocco, a remarkable frequency of dyslipidemia (50.87%) was observed in patients with SCH with high total cholesterol and LDL-C levels.27 It is a widespread endocrine disease characterized by elevated TSH and FT4 levels and is overdiagnosed and managed in older patients. Thyroid-stimulating hormone levels increase with age and these patients can recover without treatment.28
Currently, half of patients with SCH have a negative correlation with BMI and obesity, with FT3 levels being lower in this population. Obesity is associated with SCH, and ongoing evaluation of thyroid function is vital in patients with high BMI.29 Other studies have reported considerable increase in BMI in patients with SCH.30 The synergistic effects of SCH on the metabolic profiles of obese patients have been previously established.31
In the present study, elevated DBP was more frequent than elevated SBP in patients with SCH. Thus, patients with SCH commonly have dyslipidemia and arterial hypertension, and particularly high DBP.32 Hypothyroidism affects myocardial contractility and relaxation, primarily causing cardiac diastolic dysfunction rather than systolic dysfunction.33 Thyroid function may influence BP to a greater extent in women with SCH.34
In this study, 92.7% of the patients had dyslipidemia, and FT4 levels were significantly lower in patients with SCH and hypertriglyceridemia and were inversely associated with triglyceride levels. Furthermore, TSH levels tended to correlate with cholesterol levels; however, this association was not significant. Dyslipidemia is common in patients with SCH.11 Notably, triglyceride levels inversely predicted FT4 levels. In SCH, an increase in total cholesterol is independently coupled with a higher risk of progression to overt hypothyroidism, and its decrease increases the likelihood of regression towards a euthyroid state.35 Patients with SCH have significantly higher triglycerides.36 In patients with SCH, levothyroxine (LT4) treatment may decrease total cholesterol, triglyceride, and LDL-C levels.37 Distinct increases in cholesterol, LDL-C, and HDL-C levels have been observed in patients with SCH.30 Subclinical hypothyroidism often causes changes in lipid profiles that negatively influence human health. Thus, lipids can alter the course of SCH.35 Subclinical hypothyroidism must be treated to avoid the complications associated with dyslipidemia.11 Consistent with this study, a direct relationship between TSH and total cholesterol, LDL, and triglycerides was observed in patients with SCH, whereas an inverse relationship was observed between FT4, cholesterol, and triglycerides.38
In the present study, high TSH levels were significantly associated with elevated creatinine levels. Similarly, the creatinine level was a key predictor of high TSH levels. Patients with SCH have significantly elevated serum creatinine levels. Moreover, LT4 therapy may lower urinary albumin excretion, protect kidney function, and slow chronic kidney disease progression in patients with SCH with marginally elevated TSH levels.39 Hypothyroidism is thought to reduce glomerular infiltration rate and increase urine protein loss.40
Despite their global predominance, thyroid disorders are often overlooked, and may have serious health consequences. In Saudi Arabia, the prevalence of thyroid disease is approximately 50%, and most patients have SCH. The awareness and knowledge of thyroid disorders in Jeddah, Saud Arabia, are low, thus necessitating more attention to prevent and manage them.41 Despite their wide use in endocrinology, the optimal application of thyroid tests, including those for TSH and thyroid hormones, remains debatable. The American Thyroid Association emphasized the need for improved standardization and harmonization of thyroid testing.42
Study limitations
The relatively small number of cases and the absence of a control group, which limits the generalizability of the results. Large-scale longitudinal studies are required to verify these results, uncover potential mechanisms, and demonstrate the effects of treatment on CV consequences. Future inclusion of a control group may enhance the interpretation of the findings. Close monitoring of these “high-risk” individuals could help optimize treatment and reduce morbidity. Further in-depth analyses of the association with renal involvement are required.
In conclusion, the adverse impact of SCH on the lipid profile has been confirmed, particularly in female patients with increased BMI and in their fifth decade of life. Triglyceride levels inversely predict FT4 levels. The relationship between TSH and increased creatinine levels was notable. Raising awareness and knowledge on thyroid diseases, risk factors, and subclinical conditions is indispensable for the timely anticipation and treatment of these disorders and their consequences. Routine lipid monitoring and management may aid in the development of targeted therapies to mitigate the CV risk in this population. However, further research is needed before broad screening is recommended.
Acknowledgment
The authors gratefully acknowledge Editage for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 28, 2024.
- Accepted April 13, 2025.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.