


Abstract
Objectives To determine the prevalence of macrovascular and microvascular complications of type 2 diabetes mellitus and its associated determinants.
Methods We evaluated the online medical records of patients with type 2 diabetes mellitus who have been seen in chronic disease unit between April and June 2014. Seven hundred and forty-eight participants satisfied the inclusion criteria. Of these, 317 (42.4%) were males with a mean age of 57.9 years, 681 (64.3%) were obese with body mass index (BMI) of greater than 30, while only 9.6% had normal BMI (<25).
Results Only 158 (21.1%) had controlled hemoglobin A1c level. Retinopathy prevalence was 14.8% and neuropathy was 5.6%. Macrovascular complications accounted for 12.1%. Patients’ age and duration of diabetes were main predictors of developing complications. Patients with more than 20 years history of diabetes have 30% more odds of developing the complications when compared to patients with less than 10 years of diabetes history. Each increment in age by one year increases the odds of developing microvascular complications by 4% and macro vascular complication by 2%.
Conclusion Our results showed diabetic patients with poor glycemic control, and longer duration of diabetic history had higher prevalence of both macrovascular and microvascular.
Type 2 diabetes mellitus (T2DM) develops in adults and is associated with poor lifestyle habits, obesity, lack of physical activity, and unhealthy diets.1 The prevalence of diabetes in developing countries has increased over the past few years.2 The estimated number of diabetic patients globally as of 2013 was 382 million, with an estimated prevalence of 8.3%.3 The Middle East region had one of the highest prevalence rates. Kingdom of Saudi Arabia (KSA) has been classified as one of the top ten countries affected by diabetes mellitus (DM).4 The current prevalence of diabetes in KSA is estimated to be around 23%.5
Diabetic patients are at high risks of developing microvascular complications of small blood vessels or macrovascular complications affecting larger blood vessels.6 Microvascular complications are long-term complications and can be classified into diabetic retinopathy nephropathy or neuropathy.7 The narrowing of arteries leads to decreased blood flow to the heart, or to the brain, or to the limbs leading to several macrovascular complications.8
Although diabetes represents a huge health burden in KSA, data are limited regarding population-based assessment of the prevalence of various microvascular and macrovascular complications in KSA. Based on high prevalence of DM, high cost of treatment and follow up of T2DM patients and gap in existing literature, this study aimed at estimating the prevalence rate of both the microvascular and macrovascular complications and its determinants.
Methods
The study population consisted of adult patients who visited the Al-Wazarat Healthcare Center (WHC) for treatment and follow-up for T2DM between April and June 2014. The WHC is a primary health center located in Riyadh, the capital city of KSA. The study was approved by the Medical Research Ethics Committee, Prince Sultan Military Medical City, Riyadh, KSA.
Participants with active and complete medical records were included. Patients with incomplete medical records, inactive records (no visits in one year or more), and those with type 1 DM were excluded from the study. The review identified 748 eligible files.
The research team designed a form for retrieving data from the online medical records by a trained research assistant. Data collected includes the patient’s hospital number and date of visit, patient’s information such as socio-demographic characteristics, types of DM, date of diagnosis, duration of being diabetic, height, weight, body mass index (BMI), presence or absence of microvascular complications such as retinopathy, neuropathy or nephropathy, presence or absence of macrovascular complications such as stroke and cardiovascular disease (CVD).
Statistical analysis
The variables were categorized into dependent variables (macro-vascular and microvascular complications of T2DM) and independent variables such as socio-demographic characteristics such as age, gender, BMI, disease duration and hemoglobin A1c (HbA1c) level. The statistical analysis was conducted using Statistical Package for Social Sciences (SPSS) version 20.0 (Armonk, NY: IBM Corp.). The prevalence of microvascular and macrovascular complications was calculated, and then the association between participants’ sociodemographic and disease characteristics such as age, gender, disease duration, glycemic control (glycemic control is defined when the HbA1c was <7)9 BMI, and hypertension were examined using the Chi-squared test. A multiple logistic regression test was used to assess the association between the dependent and independent variables. Associations were considered to be significant at a p-value less than 0.05.
Results
The sociodemographic and baseline characteristics of the participants are shown in Table 1. Out of the 815 patients who fulfilled the inclusion criteria, 748 patients had completed the medical records and satisfied all the inclusion criteria. A total of 53 (5%) patients were removed due to incomplete data. Female participants were 431 while 317 were males. Of the 748, 327 (43.7%) were age 60 years and above with a mean age of 57.9. Most participants were obese, 681 (64.3%) had a BMI of greater than 30, while only 9.6% had normal BMI of less than 25.
Sociodemographic and disease characteristics of 748 eligible participants who visited the Al-Wazarat Healthcare Center, Riyadh, Saudi Arabia for treatment and follow-up for type 2 diabetes mellitus.
Prevalence of microvascular and macrovascular complications
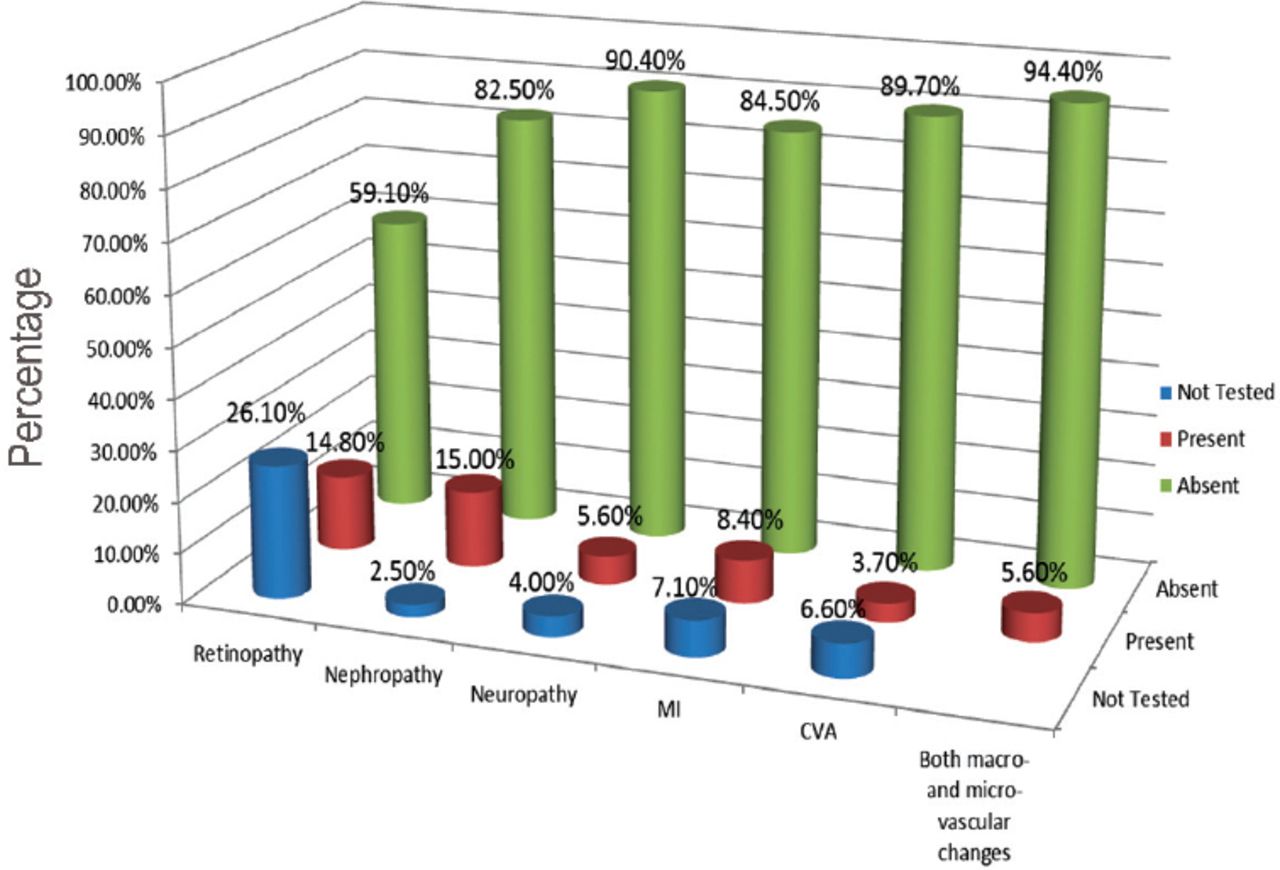
The prevalence of micro- and macro-vascular complications in patients with type 2 DM are presented in Figure 1. Out of the 748 participants, 111 (14.8%) had retinopathy, 112 (15%) had nephropathy, and 5.6% had neuropathy. Approximately 63 (8.7%) had myocardial infarction (MI), 49 (6.6%) had cerebrovascular accident (CVA). The prevalence of both micro- and macro- vascular changes in the same patient were 42 (5.6%).
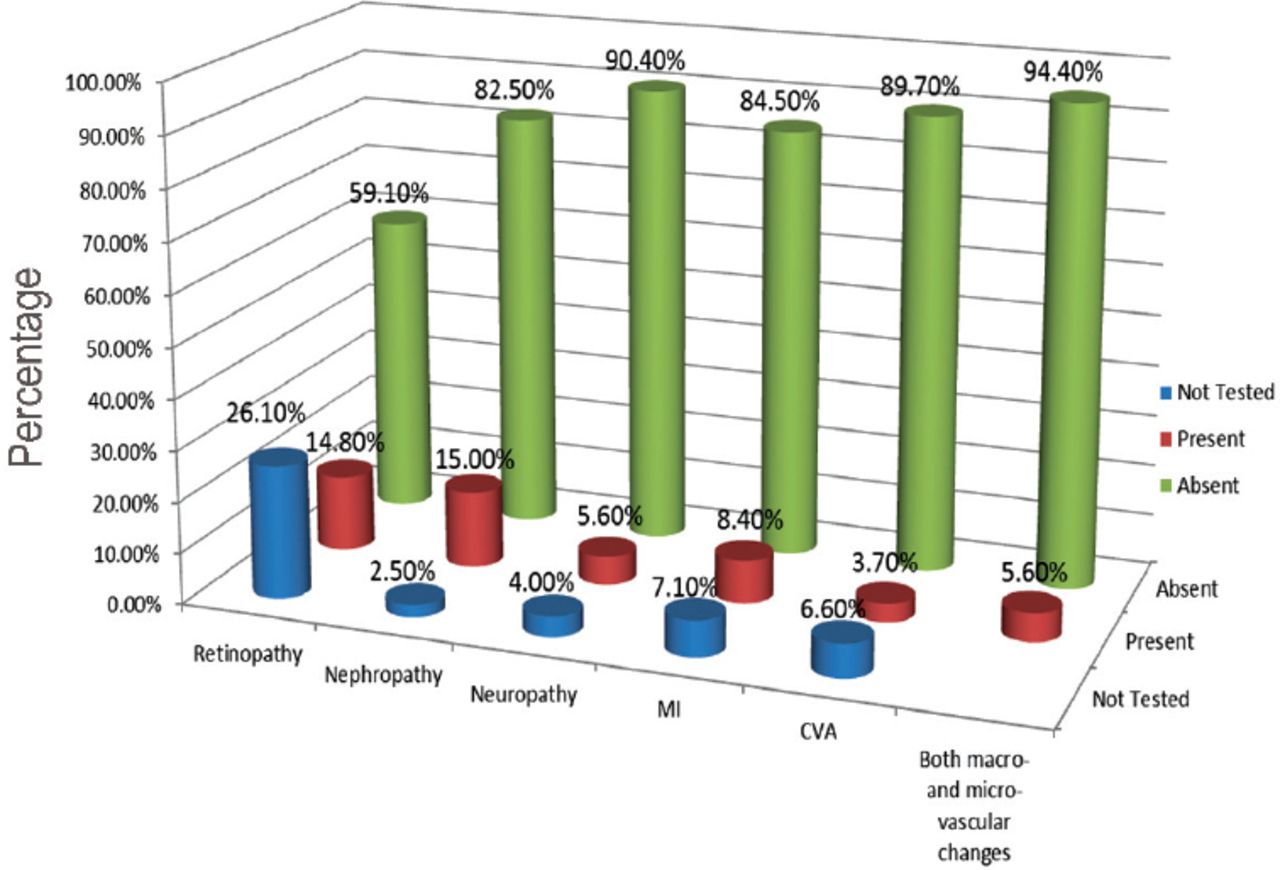
Prevalence of microvascular and macrovascular complications in type2 diabetes patients (n=748).
Predictors of microvascular and macrovascular complications
Microvascular complications and risk factor modeling with the best-fitted model are shown in Table 2. The variables that formed the model are: age (years), duration of DM (years), the HbAIc level and controlled hypertension level. Assuming all the variables remain the same, each increment in age by one year increases the odds of developing microvascular complications by 4%. Each additional year in duration of DM increases the odds of developing microvascular complications by 5%. Each high level of HbAI2 increases the odds by 40%. Patients with controlled hypertension show a protective effect on microvascular complications with the odds decreasing by 57%.
Best fitting multiple logistic regression model for the occurrence of microvascular complications.
The best-fitted model for risk factors and macrovascular complications is presented in Table 2. Age (years), duration of DM (years) and the level of HbA1c (mmol/mol) are the variables associated with macrovascular complications. For each year, increase in age and assuming all other variable are the same, the odds of developing macrovascular complications increase by 2%. For each year increase in duration of DM, the odds increase by 3%. Finally, each unit increase in HbA1c concentration increases the odds of macrovascular complications by 11%.
Discussion
Diabetes mellitus is growing faster and becoming a serious medical problem associated with higher morbidity and mortality in the KSA. The prevalence of microvascular complications such as retinopathy is as high as 14.8% in the WHC; this prevalence could even be much higher nearby private centers with less established diabetic control services. The most recent study in KSA conducted in 2000 by Khan et al10 conducted in Al-Hasa area estimated the prevalence of retinopathy by 13.6%. Our study was conducted in the capital city of Riyadh, which has a diverse population from across KSA. Globally, nephropathy prevalence among type 2 diabetic patients in different studies is much higher when compared with our result. A 2005 study conducted in South Korea estimated the prevalence of nephropathy in 267 type 2 diabetic patients to be 27%.11 The prevalence of nephropathy in this study is lower by approximately 12-13% than the 2 studies conducted in KSA, and by approximately 9-11% than studies carried out in different countries.10,11 Such difference could be related to the nature of the center as primary healthcare center. More advanced cases are referred to the endocrinology and nephrology departments in Prince Sultan Military Medical City (PSMMC).
The prevalence of macrovascular complications were found to be high, but lower when compared with the prevalence of microvascular complications. Our findings revealed the prevalence of MI was 8.4%, which was lower than other international studies such as the United Kingdom Prospective Diabetes Study (UKPDS) study (15.3%).12 However, an Italian cohort study found the prevalence of MI to be 2.2% in a cohort of 11,644 patients.13 The difference in the UKPDS and Italian studies can be attributed to the differences in diet habits. This issue can be extended to the results in our study where the consumption of fat is high, similar to North Europe, lower than Mediterranean area, and slightly higher than some regional countries like Iran.14 Cerebrovascular accident prevalence was 3.7% in our sample. In the UKPDS study, the prevalence of fatal and non-fatal CVA was 3.7% over the follow-up period.12 Peripheral VD prevalence in our study was 1.2%. The UKPDS study reported 1.4% peripheral VD in the participants without adjustment to hypertension control. This percentage dropped to 1% when hypertension control is considered. All macrovascular changes (MI, CVA, and peripheral VD) presence was 12% in our study. The UKPDS reported 22.9% macrovascular changes comparatively for the same complications.12
The prevalence of neuropathy was found to be 9.6%. The prevalence is lower than other studies as the criteria used to define neuropathy cases are stricter in our study than studies with questionnaire-based assessments.15-17 Neuropathy is tested in our center using the modified Toronto Clinical Neuropathy Score (mTCN)18 in diabetic patients to assess the neuropathy presence and severity.
Study limitations
The limitation of the study of the design does not allow inferences about cause and effect between risk factors and the presence of microvascular complications to be drawn due to the inability to investigate temporal relationships between risk factors and understanding of the relationship of the pathophysiological events responsible for these micro- and macro- vascular complications. This study is a single-center study, which is a limitation that we aim to overcome in future studies. Logistically, applying this study to a wider number of primary care centers and to the main hospital PSMMC proved problematic. Other risk factors that may confound the results, such as the smoking status of the participant, should be included in any future investigation.
In conclusion, the prevalence of both microvascular and macrovascular complications were found to be high in our study populations. It highlights the urgent need for implementation of better diabetic management services. Better public health awareness services, aggressive health educations and promotion campaigns will reduce the deadly complications of DM in the country. Further and urgent prospective and clinical trial studies to determine the prevalence of diabetic complications and its associated predictors among patients with T2DM in KSA are highly recommended.
Footnotes
Disclosure. This study was approved by the Medical Research Ethics Committee, Prince Sultan Military Medical City, Riyadh, Saudi Arabia (Project # 711).
- Received June 9, 2016.
- Accepted August 31, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}