


Abstract
Objectives: To evaluate the accuracy of transcutaneous bilirubin (TcB) measurement in healthy, jaundiced Saudi term newborns.
Methods: This prospective, cohort study was carried out from January 2009 to December 2012 on jaundiced, term infants admitted at the King Abdulaziz University Hospital, Jeddah, Kingdom of Saudi Arabia. Paired TcB and total serum bilirubin (TSB) from healthy jaundiced term newborns were obtained. The correlation and the mean difference between the 2 methods were calculated, and Bhutani nomogram for prediction of TSB by TcB was used. Any bilirubin level at low and above the intermediate risk zone was considered significant.
Results: We obtained 665 paired TcB and TSB measurements from 665 newborns. The mean age at bilirubin measurement was 44.2 ± 21 hour. Mean TSB was 147 ± 45 µmol/L, and TcB was 156 ± 50 µmol/L. Linear regression analysis showed a significant correlation between TcB and TSB (r: 0.84; 95% confidence interval [CI] = 0.82-0.86; p<0.001). The TcB tends to overestimate TSB. The mean difference between paired TcB and TSB was 17 µmol /L with a 95% CI of 40 ± 77 µmol/L. The TcB was sensitive, but less specific. The TcB sensitivity was 83% and specificity was 71% to predict TSB during the first 72 hours of life for the whole study group. The positive predictive value was 63%, and negative predictive value was 87%.
Conclusion: As found in this study, among the jaundiced healthy term Saudi newborns, TcB measurement provided accurate estimates of TSB values. The TcB measurements can be used effectively to screen newborns for significant jaundice.
Jaundice is one of the most common diagnoses during the neonatal period, which requires treatment with either phototherapy, or exchange transfusion. Cases of bilirubin induced neurologic dysfunction have been observed in otherwise healthy term and late preterm infants.1,2 The clinical evaluation of jaundice involves visual estimation of the color of the skin. However, quantification of total serum bilirubin (TSB) based on visual assessment of jaundice is subjective and inaccurate.3 Therefore, chemical methods for measurement of bilirubin in the sera of newborn infants are still the standard of care in the assessment of neonatal jaundice. However, blood sampling involves pain for newborn infants. In addition, it is important to minimize the quantity of blood that the infant loses through blood sampling. Over the last 2 decades, several studies addressed the value of transcutaneous bilirubin (TcB) measurement in newborns. The TcB measurement is quick, simple, less invasive, and cost effective. Most of the studies had validated TcB in relatively homogenous populations, such as Greek, Caucasian, Chinese, Hispanic, and Africans.4-7 Studies were varied in their assessment of the accuracy of TcB measurement; poor to excellent agreement between TSB and TcB has been reported.4-9 The aim of this prospective cohort study was to investigate the accuracy of TcB as measured by BiliCheck device (SpectRx, Inc., Norcross, GA, USA) in jaundiced, otherwise healthy, Saudi term infants who required TSB measurements.
Methods
A prospective, cohort study of jaundiced, otherwise healthy term infants who were admitted during the study period from January 2009 to December 2012 into the normal nursery at King Abdulaziz University Hospital (KAUH), Jeddah, Saudi Arabia were enrolled in the study. They were included if they fulfill the following criteria: clinically jaundiced but otherwise healthy term newborns (gestational age: 37-42 weeks); postnatal age ≤120 hours; decision by the treating physician to measure TSB for clinical purposes; and parental consent to participate in the study. The exclusion criteria were: newborns requiring phototherapy or exchange transfusion; and newborns with skin bruises, hyperpigmentation, or hemangioma on the forehead. The study was conducted according to the principles of Helsinki Declaration, and was approved by the Ethics Committee of the Faculty of Medicine & King Abdulaziz University Hospital, Jeddah. Newborns who met the inclusion criteria were enrolled in the study on a daily basis. Once the treating physician decided to carry out TSB and the parents provided consent, the TcB and TSB were performed as follows: TcB was measured by BiliChek® (SpectRx, Norcross, GA, USA) by 5 trained nursery nurses. Bili-Check® is a bilirubinometer, which corrects for the skin’s melanin, gestational age, and the skin’s hemoglobin content. All TcB measurements were obtained from the forehead using the same BiliCheck device. The BiliCheck was calibrated before each measurement using a disposable probe (BiliCal, SpectRx, Norcross, GA, USA) as per manufacturer’s instruction.9 Areas with hair, hyperpigmentation, bruises, and hemangioma on the forehead were avoided. The device displays the average in micromole/l of 5 measurements from different areas of the forehead for each bilirubin. All newborns were exposed to only the ambient fluorescent lighting in the nursery. All blood specimens were obtained by heel sticks within 10 minutes after TcB measurements. After warming of the heel and lancet puncture, blood was collected by drip method into heparin-containing tubes. The blood specimen were sent immediately for analysis using Diazo method (Dimension Vist® System and Flex® reagent cartridge, Siemens).10 The following demographic data were recorded for all infants enrolled in the study: gestational age; mode of delivery; gender; birth weight; and postnatal age in hours at the time of TSB and TcB measurement
Statistical analysis
The Statistical Package for Social Sciences version 21 (IBM Inc., Armonk, NY, USA) was used for statistical analysis. The agreement between the 2 measures of TSB and TcB was assessed using Pearson’s correlation and linear regression model including 95% confidence interval (CI) for intercepts and slopes. As Pearson’s coefficient alone can be a poor indicator to estimate the agreement between 2 diagnostic tests, we used the Bland-Altman technique to assess TSB and TcB variability.11 In this analysis, the mean bias TSB-TcB was compared against their mean for every patient, and variability was defined as ±1.96 standard deviation (SD) of the mean bias. Only the first paired sample of each baby was used for analysis.12 Prediction of TSB by TcB was assessed at low intermediate risk zone of Bhutani nomogram using standard sensitivity, specificity, and positive and negative predictive value calculations. Any bilirubin level at the intermediate low and above risk zone (40th percentile) was considered clinically significant because it usually affect the decision to discharge jaundiced newborns home. The TSB values which represent the low intermediate risk zone: were 85-≤110 µmol/L at ≤24 hours, 135-≤185 µmol/L at >24-≤48 hours, and 145-≤220 µmol/L at >48-≤72.12
Results
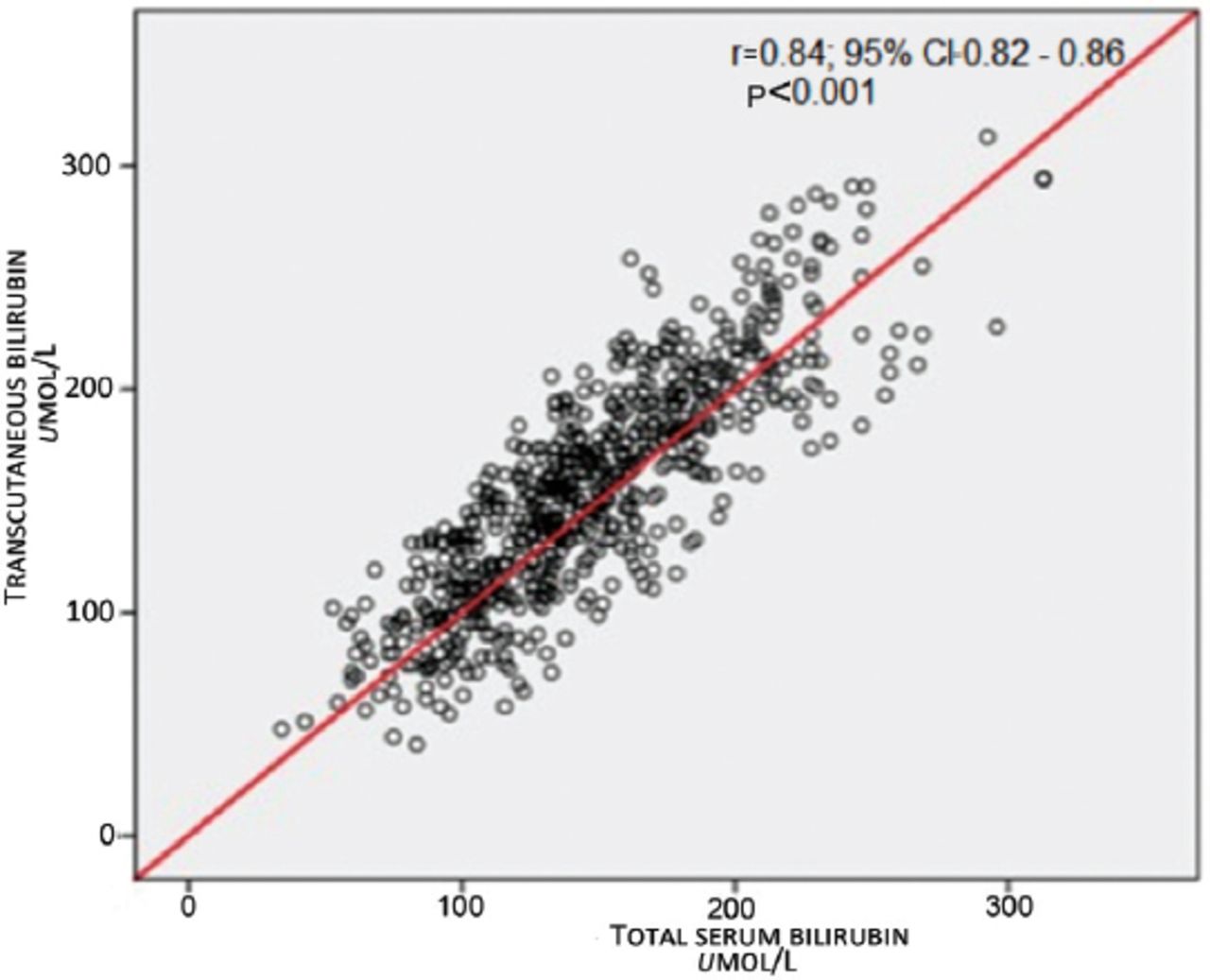
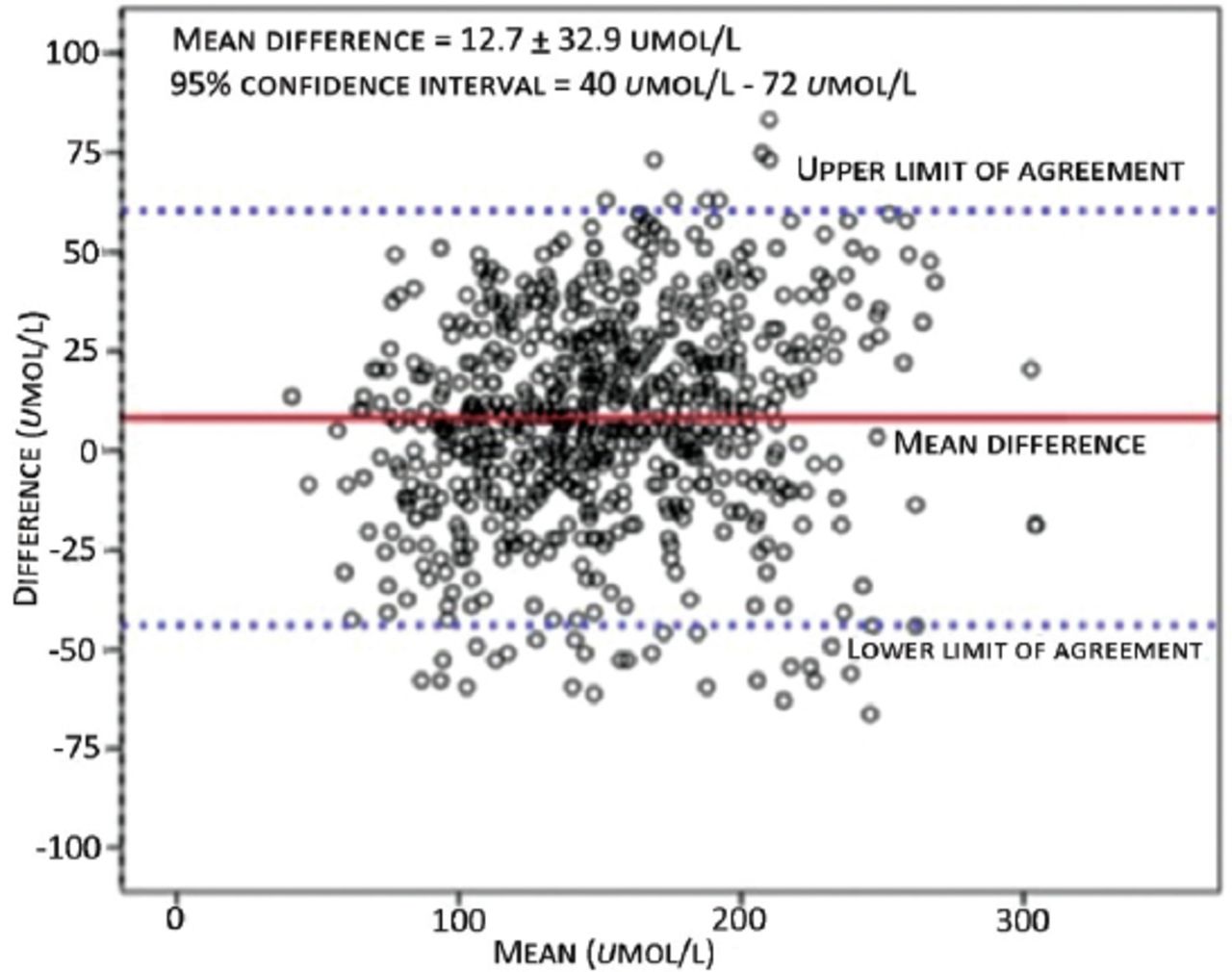
A total of 665 paired first TSB and TcB measurements were performed in 665 healthy term infants. The mean gestational age ± SD was 38.8 ± 1.2 weeks (range; 37-42 weeks), mean birth weight (BW) was 3.2 ± 0.5 kg (range; 1.7-4.8 kg), 346 (52%) were male, and 492 (74%) were born by spontaneous vaginal delivery. The mean age of bilirubin measurement was 44.18 ± 20.97 hours (range; 9-120 hours). Most of the paired TSB/TcB measurements were performed during the first 48 hours (419 [78%]). Mean TSB was 147 ± 45 µmol/L (34-313 µmol/L), and mean TcB was 156 ± 50 µmol/L (41-313 µmol/L). The TSB was ≤170 µmol/L in 477 newborns (71.7%), between 170 and 260 µmol/L in 178 newborns (26.8%), and more than 260 µmol/L in 10 newborns (1.5%). The ability of TcB measurements to predict TSB levels at intermediate low and above risk zone (40th percentile) of Bhutani nomogram is shown in Table 1. Linear regression analysis (Figure 1) showed a significant correlation between TcB and TSB (r: 0.84; 95% CI=0.82-0.86; p<0.001). The Bland-Altman plot demonstrates the level of precision of the BiliCheck device by comparing the difference versus the average of measurements between TcB and TSB values (Figure 2). The mean difference between these measurements was 12.7 ± 32.9 µmol/L with a 95% CI of 40 µmol/L to 72 µmol/L.
Ability of transcutaneous bilirubin measurements to predict serum total serum bilirubin at the intermediate low and above risk zone of Bhutani nomogram.

Relationship between transcutaneous bilirubin and total serum bilirubin levels.

Bland-Altman plot of transcutaneous bilirubin versus total serum bilirubin values.
Discussion
The identification of newborns at risk of developing significant indirect jaundice based on pre-discharge risk assessment and measurement of TSB plotted on hour-specific nomogram had been validated and widely used.8-9,13 Transcutaneous measurement of bilirubin is a non-invasive, quick tool aiming to reduce the number of painful blood sampling and the amount of blood loss. Our study showed a good correlation between TcB measured by BiliCheck™ and TSB in a cohort of normal Saudi term infant admitted to the nursery. The results of our study indicate that TcB measurement provides an accurate estimate of TSB values in healthy Saudi newborn infants, and it can be used as a screening method before discharging them from the nursery. The Bland-Atman analysis demonstrates that TcB on average tends to overestimate TSB but measurement of TcB can both under- or over-estimate TSB values. The TcB was quite sensitive but relatively less specific. The sensitivity was 83% and specificity was 71% during the first 72 hours of life for the whole study group. The positive was 63%, and negative predictive value was 87% during the same period. When the mean difference (bias) was added, the sensitivity increased to 91%, but the specificity remains almost the same. The positive predictive value was 63% while the negative predictive value increased to 94%. The positive predictive value of TcB in our study is low, while the negative predictive value is high.
Overestimation of TSB by TcB measurement is quite safe but possibly leads to unnecessarily blood works. However, if TcB measurement significantly underestimates TSB, newborns requiring phototherapy, or close follow up will be missed. This is in agreement with other studies conducted in the North American, Hispanic, Chinese, and Italian populations.7-9,12-14 However, a study from Greece4 concluded that TcB does not correlate well with TSB and tends to underestimate TSB.
There are some limitations in this study: 1) we specifically studied clinically jaundiced newborns as determined by the treating physician rather than including all newborns. We feel this is an important time for the newborns because clinical decisions need to be finalized, such as measuring TSB, or deciding on the outpatient follow up after discharge from the hospital; 2) the TcB were measured by trained nursery nurses rather than one study investigator. This raises the issue of inter-observers variability. However, in real life, multiple users will use BiliCheck; 3) the TSB values in our study sample were relatively low. Only 71.7% of TSB values were ≤170 µmol/L, and only 1.5% of TSB values were ≥260 µmol/L. This is because the study was conducted in the nursery where jaundice was discovered early, and subsequently TSB was measured. Some studies15,16 reported that TcB levels provide less accurate estimates of TSB values at higher serum bilirubin levels as opposed to lower levels, in which TcB tended to overestimate the TSB levels; and 4) the study was conducted in the western region of Saudi Arabia with a population of diverse ethnic backgrounds and various degree of skin pigmentation to address the issue of the accuracy of TcB. We did not look at the degree of skin color, however, BiliCheck scans the whole spectrum of visible light and automatically subtracts the beam reflected by confounding factors, such as hemoglobin, dermal thickness or melanin, and it isolates the absorption of light due to bilirubin in the capillary bed and subcutaneous tissue, therefore calculating the concentration of bilirubin.
In conclusion, among jaundiced otherwise healthy term Saudi newborns, TcB measurement using BiliCheck provided a reasonably accurate estimate of TSB values. The TcB measurement has a high negative predictive value, so it can be used effectively to screen newborns for significant jaundice. The TSB measurements can be reserved for those newborns with TcB level above intermediate low risk zone of Bhutani nomogram. Further studies are needed to address the reliability of TcB measurement at high levels of total serum bilirubin. Also, studies are needed to evaluate the impact of routine TcB measurement before home discharge on the re-admission into the hospital due to high bilirubin levels.
Illustrations, Figures, Photographs
All figures or photographs should be submitted in a high resolution (minimum 300 DPI) electronic version saved in jpeg or tiff format. Original hard copies of all figures may be requested when necessary. Photographs will be accepted at the discretion of the Editorial Board. All lettering, arrows, or other artwork must be done by an artist or draftsman. If arrows are used please ensure they appear in a different color to the background color, preferably black with a white border, or white with a black border. If arrows distinguish different items on the figure then different arrow styles should be used ie. long, short, wide, narrow. Written informed consent for publication must accompany any photograph in which the subject can be identified. Written copyright permission, from the publishers, must accompany any illustration that has been previously published.
Acknowledgment
The author gratefully acknowledges the Deanship of Scientific Research, King Abdulaziz University, Jeddah, Saudi Arabia for funding this study and the nurses in the normal newborn nursery of King Abdulaziz University Hospital for helping in the measurement of transcutaneous bilirubin.
Footnotes
Disclosure. Author has no conflict of interests, and the work was not supported or funded by any drug company. This study was funded by the Deanship of Scientific Research, King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia.
- Received September 17, 2015.
- Accepted December 23, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}