


Abstract
Objectives: To review the evidence of the benefits and harms of infant male circumcision, and the legal and ethical perspectives of infant male circumcision.
Methods: We conducted a systematic search of the literature using PubMed, EMBASE, and the Cochrane library up to June 2015. We searched the medical law literature using the Westlaw and Lexis Library law literature resources up to June 2015.
Results: Male circumcision significantly reduced the risk of urinary tract infections by 87%. It also significantly reduced transmission of human immunodeficiency virus among circumcised men by 70%. Childhood and adolescent circumcision is associated with a 66% reduction in the risk of penile cancer. Circumcision was associated with 43% reduction of human papilloma virus infection, and 58% reduction in the risk of cervical cancer among women with circumcised partners compared with women with uncircumcised partners. Male infant circumcision reduced the risk of foreskin inflammation by 68%.
Conclusion: Infant male circumcision should continue to be allowed all over the world, as long as it is approved by both parents, and performed in facilities that can provide appropriate sterilization, wound care, and anesthesia. Under these conditions, the benefits of infant male circumcision outweigh the rare and generally minor potential harms of the procedure.
Male circumcision is defined as partial or complete surgical removal of the foreskin (prepuce) of the penis. The word ‘circumcision’ comes from the Latin circumcidere (meaning ‘to cut around’).1 Infant male circumcision dates back more than 6000 years as indicated in pharaonic drawings and circumcised Egyptian mummies.2 Male circumcision is mandatory in Judaism and it is required to be performed on the eighth day after birth.3 Male circumcision is also mandatory, per the majority of Muslim scholars and it is preferred to be performed on the seventh day after birth.4 Both religions relate the practice of circumcision to Abraham (Ibrahim) who circumcised himself after the age of 80.3,4 Male circumcision is prevalent in many countries as part of the cultures and customs, or for the claimed health benefits of circumcision. The prevalence of male circumcision in the United States is around 85%, 25% in the Philippines, and 4.7% in Australia.5 In UK 15.8% of men are circumcised.6 Therapeutic circumcision represents 2.5% of neonatal circumcisions, which is performed for patients with inflammation in the foreskin, such as phimosis, balanitis, and localized diseases of the foreskin.7 The aim of this paper is to review the evidence of the benefits and harms of infant male circumcision, and the legal and ethical perspectives of infant male circumcision.
Methods
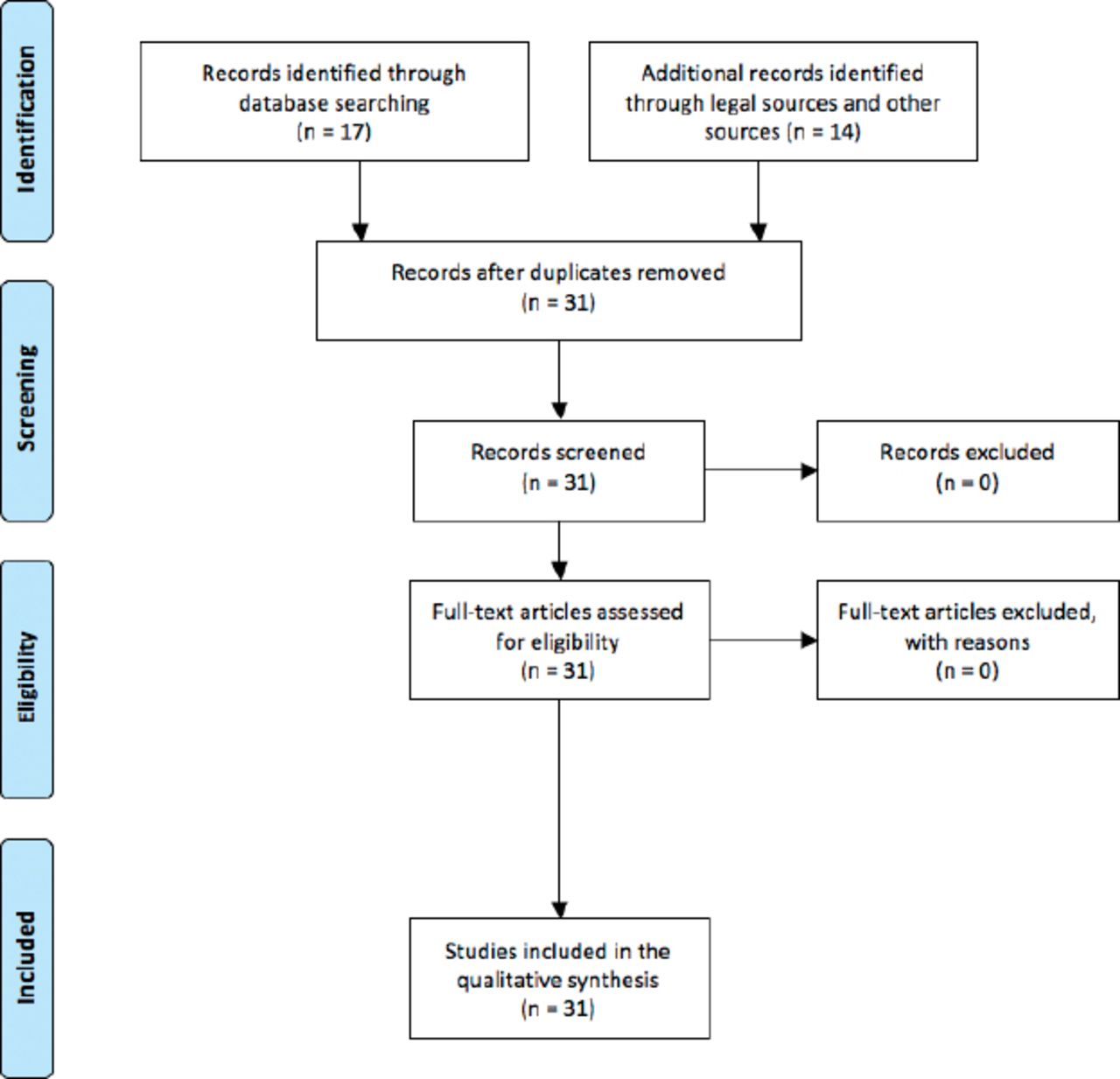
There is significant controversy around non-therapeutic male circumcision. The debate regarding health benefits and harms of male circumcision is a very important component of the controversy. Proponents and opponents of male circumcision can be very selective in citing biased medical research to support their view and dismiss their opponents. The claimed medical benefits of infant male circumcision are very important to the discussion of the ethical and legal debate of infant male circumcision. We conducted a systematic search of the literature using PubMed, EMBASE, and the Cochrane library up to June 2015. We limited main references on the benefits and harms of infant male circumcision to systematic reviews of the literature. Systematic review of the literature is a very important type of medical research, which systematically searches for all relevant publications, combines it and analyzes it using appropriate statistical methods. This methodology helped in resolving several controversies in the medical literature. Systematic reviews are considered to be at the top of the hierarchy of the levels of evidence by almost all medical guidelines authorities in the world.8 We searched medical law literature using Westlaw and LexisLibrary law literature resources up to June 2015 (Figure 1).

Flow diagram of searching results addressing the cost-effectiveness of circumcision.
Results
Seventeen systematic reviews and meta-analysis were found in our search. Four additional studies addressed the cost-effectiveness of circumcision. 10 relevant legal cases were found and reviewed see Figure 1.
Benefits of circumcision
Male circumcision is an active area of research. Several well-conducted research papers evaluated the benefits and harms of male circumcision. In a large systematic review of 12 studies9 including 402,908 children, circumcision significantly reduced the risk of urinary tract infections (UTI) by 87%.9 This is a very important outcome as UTIs are relatively serious infections, which can cause permanent kidney damage.10 In a large systematic review including 15 studies (4 randomized control trial and 11 prospective cohort studies) there was a significant reduction in the transmission of human immunodeficiency virus (HIV) among circumcised men by 70%.11 A systematic review including 8 studies showed childhood and adolescent circumcision to be associated with 66% reduction in the risk of penile cancer. This benefit disappeared among males circumcised during their adulthood.12 Circumcision was associated with 43% reduction of human papilloma virus (HPV) infection as shown in a large systematic review of 21 studies including more than 14000 participants.13 Human papilloma virus infection is associated with genital warts, penile cancer, and cervical cancer.14,15 The benefits of circumcision extend to their partners. In a large systematic review of 7 studies including 1913 couples, circumcision was associated with a 58% reduction in the risk of cervical cancer among women with circumcised partners compared with women with uncircumcised partners.16 This is a very significant outcome as cervical cancer is the second most common cancer among women worldwide.17 A large systematic review including 8 studies showed male infant circumcision to reduce the risk of foreskin inflammation by 68%.18 Circumcision is an important cultural and religious part of the identity of several communities. Circumcision has important positive influence on the mental and psychosocial aspects of individuals within these communities.19,20
Several studies evaluated the harms associated with infant male circumcision. One of the main arguments against infant male circumcision is the claim that male circumcision adversely affects the male sexual function. This claim does not stand scientific scrutiny. A large systematic review of 10 published studies, including a total of 9317 circumcised and 9423 uncircumcised men did not show any adverse effects of circumcision on any aspect of the male sexual function, including erection, orgasm, and ejaculation.21 This was confirmed in another large systematic review analyzing 10 studies including more than 18000 individuals, which showed that male circumcision did not have any adverse effects on different aspects of sexual functions.20 Another large systematic review of 16 prospective studies evaluated complications following neonatal and infant male circumcision, and did not show severe adverse events in 14 studies. Two studies reported severe adverse events at a rate of 2%. The main adverse events were bleeding, infections, incomplete circumcision, and adverse events related to anesthesia. Older children circumcision was associated with more complications than that for neonates and infants.22 A large analysis including 1,400,920 circumcised males in the United States showed the incidence of total male circumcision’s adverse events to be less than 0.5%. The incidences of adverse events were 10-20-folds greater for males circumcised after the age of one year.23
Pain is an important harm associated with circumcision; however, several anesthetic methods were shown to be safe and effective in controlling pain during the procedure among infants.24,25
To give an estimate of one aspect of the benefit risk ratio of infant male circumcision in UK we use the prevention of penile cancer as an example. The prevalence of penile cancer in UK is increasing and it is exceeding 400 cases of penile cancer diagnosed annually with a 5 years survival rate of around 65%. Approximately 90 patients die because of penile cancer in UK annually, 66% of these deaths (60 deaths) would be prevented by infant male circumcision.26 The documented annual number of deaths related to male circumcision is very rare; however, it is estimated to be 16.27 Overall at least 40 deaths in UK could be prevented by adopting infant male circumcision. Similar figures were estimated in Australia and the United States.28
Cost-effectiveness of male circumcision
Fair distribution of the available scarce resources is a very important factor in adopting health care policies and legislations. Several studies evaluated the cost-effectiveness of male circumcision within different settings. A large systematic review of 5 cost-effectiveness studies showed male circumcision to be a very cost-effective intervention in the prevention of HIV. The reported cost per HIV infection averted ranged from US$174 to US$2808.29 Infant male circumcision is more economically attractive that adolescent and adult male circumcision. The direct cost of adolescent and adult circumcision is 4 times the direct cost of neonatal circumcision. In addition the overall direct and indirect cost effectiveness of infant male circumcision programs are much more attractive than that of adolescent and adult circumcision mainly due to the lower direct cost of the procedure, fewer complications, and faster recovery.30 The overall cost of post-neonatal circumcision was estimated to be 10 times more than that of neonatal circumcision.31 In the event that male circumcision rates were to decrease to 10% in the United State the additional costs to be added to the health care system over 10 years would exceed $4.4 billion.32
Discussion
Based on an extensive review of the American Academy of Pediatrics (AAP) Task Force on Circumcision, which included members from the American Academy of Family Physicians, the American College of Obstetricians and Gynecologists, and the Centers for Disease Control and Prevention concluded that the current evidence indicates that the health benefits of newborn male circumcision outweigh the risks, and the benefits of newborn male circumcision justify access to this procedure for those families who choose it.33 The analysis of the AAP included the literature published before 2012. Over the last 3 years, more research was published supporting the AAP taskforce recommendations. Some of these publications were referred to in previously mentioned analysis of the benefits and harms of male circumcision. Other international health authorities supported the practice of infant male circumcision. The World Health Organization (WHO) and the Joint United Nations Program on HIV/AIDS (UNAIDS) recommend infant male circumcision as an important element of HIV prevention.34
Law and ethics of infant male circumcision
Common law as in indicated in SS v Secretary of State for the Home Department affirmed that circumcision could be carried out without violating the child’s rights if it was carried out in the context of loving family relationships and was supported by both parents.35 The court in Re U (A child) emphasized that the 2 parents jointly can exercise parental responsibility to arrange the ritual circumcision of their male child.36 Common law considered circumcision lawful despite the fact that it involves violation of bodily integrity as indicated in R v Brown, where lord Templeman said “Surgery involves intentional violence resulting in actual or sometimes serious bodily harm but surgery is a lawful activity. Other activities carried on with consent by or on behalf of the injured person have been accepted as lawful notwithstanding that they involve actual bodily harm or may cause serious bodily harm. Ritual circumcision, tattooing, ear-piercing, and violent sports including boxing are lawful activities”.37 There is no single country in the world that bans infant male circumcision; such legislation will set a legal and ethical precedence. The only court to ban infant male circumcision was in Cologne in 2012, which resulted in a very strong reaction within Germany and all over the world. The District Court of Cologne held that the circumcision of a 4 year old Muslim boy was unlawful mainly because of the violation of bodily integrity and due to the lack of consent from the child. The doctor performing the circumcision was, however, acquitted because the court decided that he acted under an unavoidable mistake of the law due to the lack of unanimous opinion on this issue at the time.38 The Cologne court decision was criticized by legal and ethical experts within and outside Germany. Chancellor Angela Merkel warned that Germany would become a “laughing stock” for the rest of the world if it allowed any ban on the circumcision of boys to stand. A few months later Germany’s parliament approved a resolution that called on Berlin to create legislation that would ensure that circumcision of boys remain legal in the country.39 Ultimately, Germany’s parliament passed a law allowing infant male circumcision.40
In UK, the Children Act 1989 (and Children Act 2004) gives parents various parental responsibilities in regards to their children. One of these responsibilities is the responsibility to safeguard and promote the child’s health, development, and welfare. The Children Act 1989 requires that child welfare be the paramount consideration. According to this Act, parents also have the right to act as the child’s legal representative. These responsibilities and rights give parents, (or the one with parental responsibility), the right to consent to medical treatment on behalf of their infant.41,42 The best interest of infants is a very important test and pre-requisite for legitimacy of medical interventions in infants.43 Best interest includes the physical and mental health and emotional well-being of the child.44 Medical bodies within UK including the National Health Services (NHS), and the British Medical Association (BMA) encourage parents and health care professionals to consider the best interest of children as part of the consent of any medical treatment provided for minors.45,46 The BMA issued an ethical and legal guidance for physicians, which requires both parents to consent to infant male circumcision.47 As indicated previously, multiple systematic reviews with comprehensive review of the literature have consistently showed infant male circumcision to have multiple significant benefits compared with the harms associated with it. In addition, the important cultural and religious values linked to infant male circumcision add to the mental and emotional well-being of the child. Banning infant male circumcision will deprive parents from promoting their children health and welfare, which is a serious violation of the Children Act 1989.41
At the international level the United Nations Convention on the Rights of the Child Article 14, 20, and 30 give parents the rights to teach their children regarding their religious and cultural beliefs and practices.48 Furthermore, according to article 4 of the United Nations Declaration on the Elimination of All Forms of Intolerance and of Discrimination Based on Religion or Belief “The parents or, as the case may be, the legal guardians of the child have the right to organize the life within the family in accordance with their religion or belief and bearing in mind the moral education in which they believe the child should be brought up”.49 Logically we cannot assume that infant male circumcision is excluded from these international agreements as theses conventions and declarations were signed by several countries, which practice infant male circumcision as part of their religious and cultural beliefs. Criminalizing infant male circumcision will violate these international agreements recognized by UK. In addition, Article 8 of the European Convention on Human Rights (ECHR) supports the right to respect private and family life. Based on the consistent evidence, which shows infant male circumcision to promote health, banning infant male circumcision arguably violates Article 8 of the ECHR. Furthermore, Article 9 of ECHR supports freedom of thought, conscience and religion. Depriving parents from consenting to circumcision of their children is a violation of their rights to manifest their religious beliefs guaranteed by article 9 of the ECHR.50 Common law supported the view that circumcision does not infringe the ECHR as indicated in SS v Secretary of State for the Home Department.35
Infant male circumcision fulfills the principle of beneficence based on the established benefits of circumcision. The harms associated with infant male circumcisions compared with the significant benefits associated with it make infant male circumcision meet the non-maleficence principle. The benefits of infant male circumcision by far outweigh its harms, which make it in the best interest of the infant. Infant male circumcision will result in health maximization of the overall public health because the benefits of infant male circumcision are not limited to the circumcised individual but it expands to cover the health, economy, social, and cultural aspects of the community. Infant male circumcision is cost-effective, prevents diseases, and allows fair and just distribution of resources. These facts make infant male circumcision an ethically acceptable practice. Infant male circumcision should continue to be allowed in virtue of its proven wide spectrum benefits. To ban the use of an intervention with a potentially substantial beneficial physical, psychosocial, and public health effect violates the basic principles of virtue ethics. The wide and significant benefits of infant male circumcision compared with its harms would justify circumcision from a consequentialist ethical view. On the other hand, there are several serious catastrophic consequences of banning infant male circumcision, which represent deeply-held religious beliefs cultural customs and social norms. Such a ban may drive the practice underground, which could be associated with higher risks of adverse events and serious medical consequences for infants.
Opponents of infant male circumcision raised several important arguments against the practice. One of these arguments is the suggestion that circumcision can be delayed so that the boy can make his own decision and exercise autonomy and self-determination when he gets older as a Gillick competent child (namely, a child who is 16 years or younger, and who is able to consent to his/her own medical treatment without the need for parental permission or knowledge, per English law” or as an adult. This argument does not consider the fact that conducting circumcision during infancy is crucial to maximize a wide range of medical benefits. The benefits of infant male circumcision start early after the procedure and continue through life. As indicated previously, these benefits include the early prevention of UTIs, and inflammatory foreskin conditions. Infant’s circumcision will ensure protection against multiple sexually transmitted diseases in case they became sexually active early in their adolescence. In addition, circumcision during infancy caries much lower risks of complications than circumcision during adolescent age or later, which make circumcision in the best interest of the infant. Furthermore, circumcision during infancy is by far more cost-effective than circumcision performed later in life. Adult and adolescent circumcision is disruptive to the work and education of the individual, it requires more time for recovery, causes loss of privacy and absenteeism from sexual activities. Based on these facts legally and ethically parents can consent to infant circumcision because it is in the best interest of their infant.
Violation of the bodily integrity of the infant is another important argument against infant male circumcision. The general legal interest in bodily integrity was first affirmed in Schloendorff v. Society of New York Hospital. Judge Cardozo affirmed that “Every human being of adult years and sound mind has a right to determine what shall be done with his own body”.51 The argument that circumcision violates the child’s rights to bodily integrity does not consider the fact that infant’s right to bodily integrity can be breached in the best interest of the infant, which makes vaccination tonsillectomy and other medical and surgical interventions permissible. Infant male circumcision is in the best interest of infants as shown in the review of the medical benefits which outweighs its harms. The additional important cultural and religious impacts of infant male circumcision in certain cultures add to the mental and psychological well-being and integrity of the individual within his own community.
Finally, a large benefit-risk analysis evaluating the risk-benefit ratio of infant male circumcision revealed that benefits exceed risks by at least 100 to 1 over the lifetime. This benefit risk ratio was similar to that of immunization.52 This makes infant male circumcision in the best interest and welfare of the infant. In English law The Children Act 198941 gives child welfare the paramount consideration. In addition common law gives children best interest priority over children autonomy, self-determination, and body integrity as indicated in F v F.53
In conclusion, infant male circumcision should continue to be internationally as long as it is approved by both parents, and performed by individuals with appropriate surgical skills in facilities that can provide appropriate sterilization, wound care, and anesthesia. Under these conditions, the harms associated with infant male circumcision are rare. Infant male circumcision is justified legally and ethically. It is in the best interest of the infant from the physical, mental, and cultural aspect. Its benefits outweigh its harms. Banning infant male circumcision will deprive parents from their rights to ensure the welfare of their children, which is paramount. Such a ban will deprive families from their rights to practice their religious and cultural beliefs. Prohibiting male infant circumcision will violate several ethical principles including beneficence and justice and will result in serious catastrophic consequences.
Acknowledgment
The authors would like to thank Dr. Gerard Porter, Lecturer in Medical Law & Eithics, School of Law, University of Edinburgh, United Kingdom for his help as Course Director of the Medical Law & Ethics Program.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received February 4, 2016.
- Accepted June 19, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}