


Abstract
Objectives: To determine the accuracy of the Broselow tape on estimating body weights of selected Saudi children.
Methods: This is prospective study of children aged 7 days to 13 years who attended the Emergency Department of King Fahd Hospital of the University, Imam Abdulrahman Bin Faisal University, Saudi Arabia, from June 2015 to September 2015. Only children <34 kg were enrolled for the study and children with triage categories I and II were eliminated to avoid delay in providing appropriate treatment in these circumstances.
Results: The relationship between the actual and tape estimated body weights showed a correlation coefficient of 0.945 (p<0.001) for all children. When adjusting the correlation coefficient related to weight groups, the correlation coefficient was 0.911 (p<0.001) for children with body weights between 10 to 25 kg.
Conclusion: The Broselow tape measurements do not provide satisfactory results for all children in the selected population, but do provide highly correlated measurements for those children with body weights between 10 and 25 kg.
Children with a wide variety of clinical conditions report to the emergency units of hospitals. The most commonly reported emergency clinical conditions are respiratory distress with or without hypoxemia, circulatory impairment or shock and seizures with distorted consciousness, which require immediate intervention and resuscitation. Pediatric resuscitation and fixing the size of instrument used for management is crucial, and is always a challenging experience for the emergency physicians, pediatricians, and anesthesiologists in the above mentioned conditions. Dosing of medicine for these conditions is absolutely based on body weight of the child and the dosing decision will be crucial in managing these critical conditions. Accurate measurement of body weight is mandatory for deciding the dosage of medication, especially for the intravenous administration of drugs during resuscitation and anesthesia. Most often it is difficult and sometimes impractical to weigh the child in a critical condition.
Broselow Pediatric Emergency Tape (BPET) is as an immediate solution to the burning problem of weight estimation faced by the pediatric healthcare team across the globe, which helps to estimate body weight of the critically ill child in accordance with his/her height. Broselow Pediatric Emergency Tape is a color-coded tape, which works with height-weight correlation, and has become one of the commonly used methods to estimate weight of children in emergency units. The tape is also embedded with pre-calculated dosage of medication, which helps to eliminate possible errors. There are many studies to illustrate its accuracy. According to AlHarbi et al,1 BPET provided accurate estimation of the body weight based on measured body height. Lubtiz et al2 also concluded in their study that the use of BPET is a simple, accurate method of estimating pediatric weights and drug doses and eliminates the need for memorization and calculation. In this respect, AlHarbi et al3 had gone one step ahead by looking into the accuracy of measurements based on the 2 versions of BPET and concluded that the 2 versions of BPET 2007 and 2011 provided accurate estimation of the body weight based on measured body height, but according to them the 2011 version provides more precise estimate for weight. Even though there are several studies agreeing with the accuracy of BPET measurements, there are a few contradictive findings from researchers on its precision among children of different ethnicity and nutritional status. Mishra et al4 observed that as pediatric weight increases, predictive reliability of BPET decreases. This raises concerns over the use of the BPET in Indian children because body weight was overestimated in those weighing >18 kg. Khouli et al5 also indicated that the BPET estimated weight was different from the scale weight by more than 10% in a substantial percentage of Mexican children. Whereas, Clark et al6 conducted their research in the “hungriest place on earth”, as quoted in the title of their study, and came up with a conclusion that the BPET and age-based formulas selected for comparison were all markedly inaccurate in both the non-malnourished and the malnourished populations studied, worsening with increasing malnourishment. Chiengkriwate et al7 reported that the accuracy of BPET in the weight estimation of Thai children decreases with increasing height, and the tape underestimates Thai children’s weight. Similar findings were reported by So et al8 as well and they concluded that BPET is accurate for weight estimation in children ≤25 Kg, but the Theron formula9 performs better with patients weighing >40 Kg. They also mentioned that the BPET was not statistically superior to the Leffler formula9 in subjects weighing 25.1 to 40 kg and suggested for a separate cohort to evaluate the validity of the alternative predictive formula.
This study was designed to test the accuracy of BPET on estimating body weight of Saudi children presenting in the emergency department in our locality with respect to their body lengths.
Methods
This is a prospective study conducted in the Emergency Department of King Fahd Hospital of the University, Imam Abdulrahman Bin Faisal University, Dammam, Kingdom of Saudi Arabia. Children aged 7 days to 13 years with body weight <34 kg were enrolled in the study conducted during the period from June 2015 to September 2015. Children with triage categories I and II were eliminated from the study to avoid delay in providing appropriate treatment in these circumstances. All demographic information of every child was gathered, which includes age (in months) and gender of each child.
The trained nursing staff of emergency department in the hospital measured the estimated body weight of children using the standard BPET (Version 2011a). Measurement was taken with the child in supine position, where the tape was positioned from crown to the heel. The marking on the tape into which the child fell was determined and the corresponding body weight estimation was recorded. Along with the BPET measurement, the actual body weight of the child was measured with a standard digital weighing machine. The measurement was taken in Kilograms up to one decimal place. In order to obtain the actual body weight the measurement was taken with clothing, but no jackets (minimal dress). The same measurement was repeated by a different person to cross-check accuracy of the measurement and the measurements were subjected to reliability by Cronbach’s alpha, which provided a reliability of 0.949 (94.9%). Children above the body weight of 34 Kg and below 3 Kg were eliminated during data analysis, since BPET provides body weight estimation in the range from 3 kg to 34 kg.11
Statistical analysis
All categorical variables were presented by frequency with percentage, and the continuous variables were presented by mean and standard deviation. Spearman’s Rank Correlation coefficient, Cronbach’s Alpha, and Bland-Altman limits were used to determine internal consistency and reliability of agreements. All the analysis was carried out using IBM SPSS Statistics for Windows, Version 21.0. (Armonk, NY: IBM Corp.). A p-value less than 0.05 were considered as significant.
Results
The data set consists of measurements from a total number of 527 children, of which 290 (55%) were males. The descriptive data illustrates demography of the enrolled patients in the study. The mean age of children was 50.4 ± 39.3 months and the median age was 36 months (range 5 days - 156 months). Most children were Saudi nationals, accounting to 90.1% (n=473) of the study group and non-Saudi children were 9.9% (n=52). The mean actual body weight was 17.5 ± 9.3 and the median weight was 15.0 (2-92). The standard scale measurement was followed using the Broselow tape and the mean body weight was observed as 17.1 ± 9.3 and its median weight was 15 Kg (range 3-81).
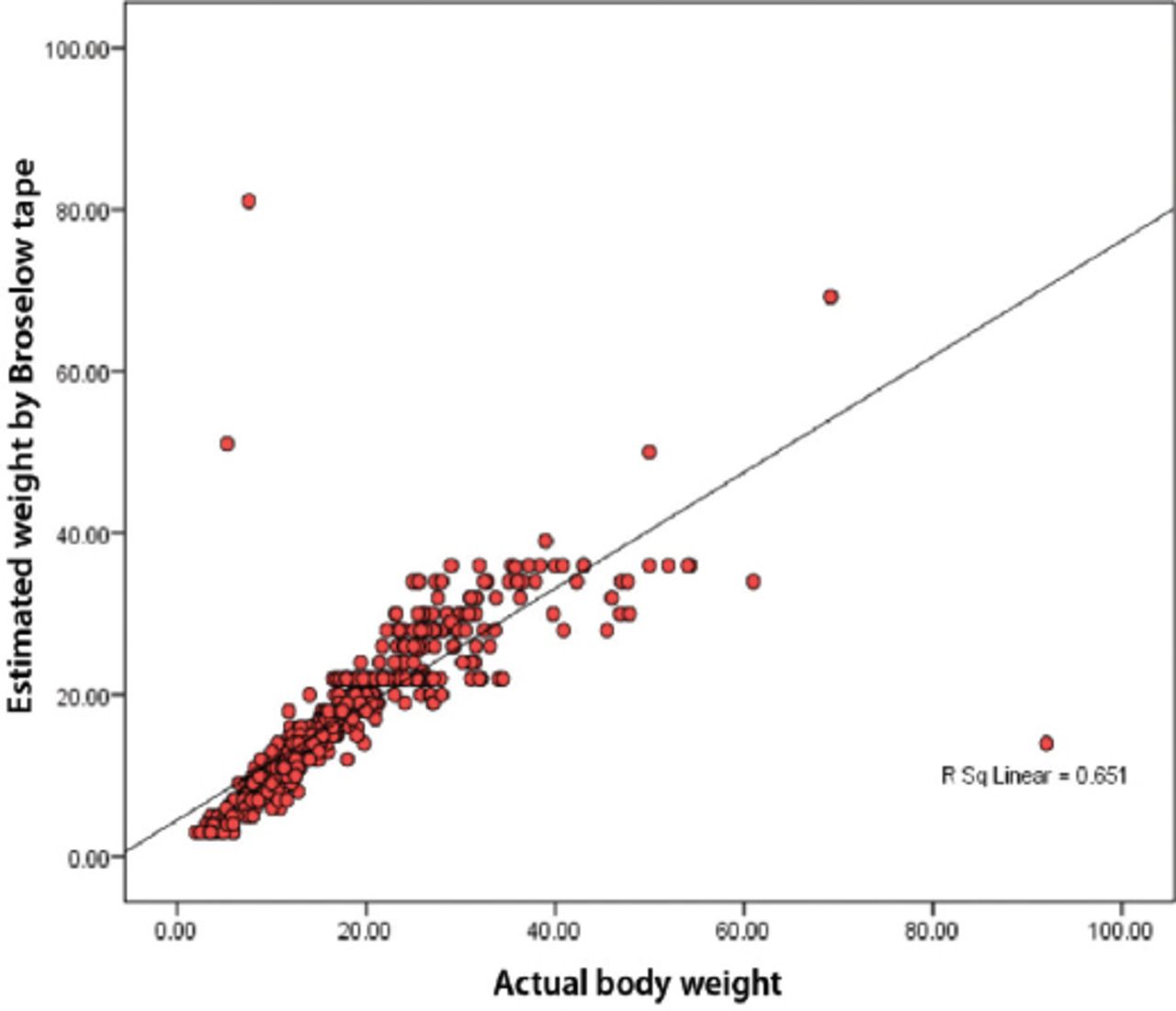
The data was analyzed to explore the relationship between overall actual body weight and the BPET measurements. The results (Figure 1) elucidates a positive relationship between weight obtained by a standard weighing machine and Broselow measuring tape, which indicates a strong correlation (r= 0.945, p<0.001). This illustrates that both the measurements are related to each other, but it is not 100% accurate. The accuracy is only up to 65.1% (r2 = 0.651). In order to find the accuracy and anomalies of 2 measurements, we explored the Bland-Altman plot with 95% confidence interval.

Scatter diagram of measured weight versus Broselow weight.
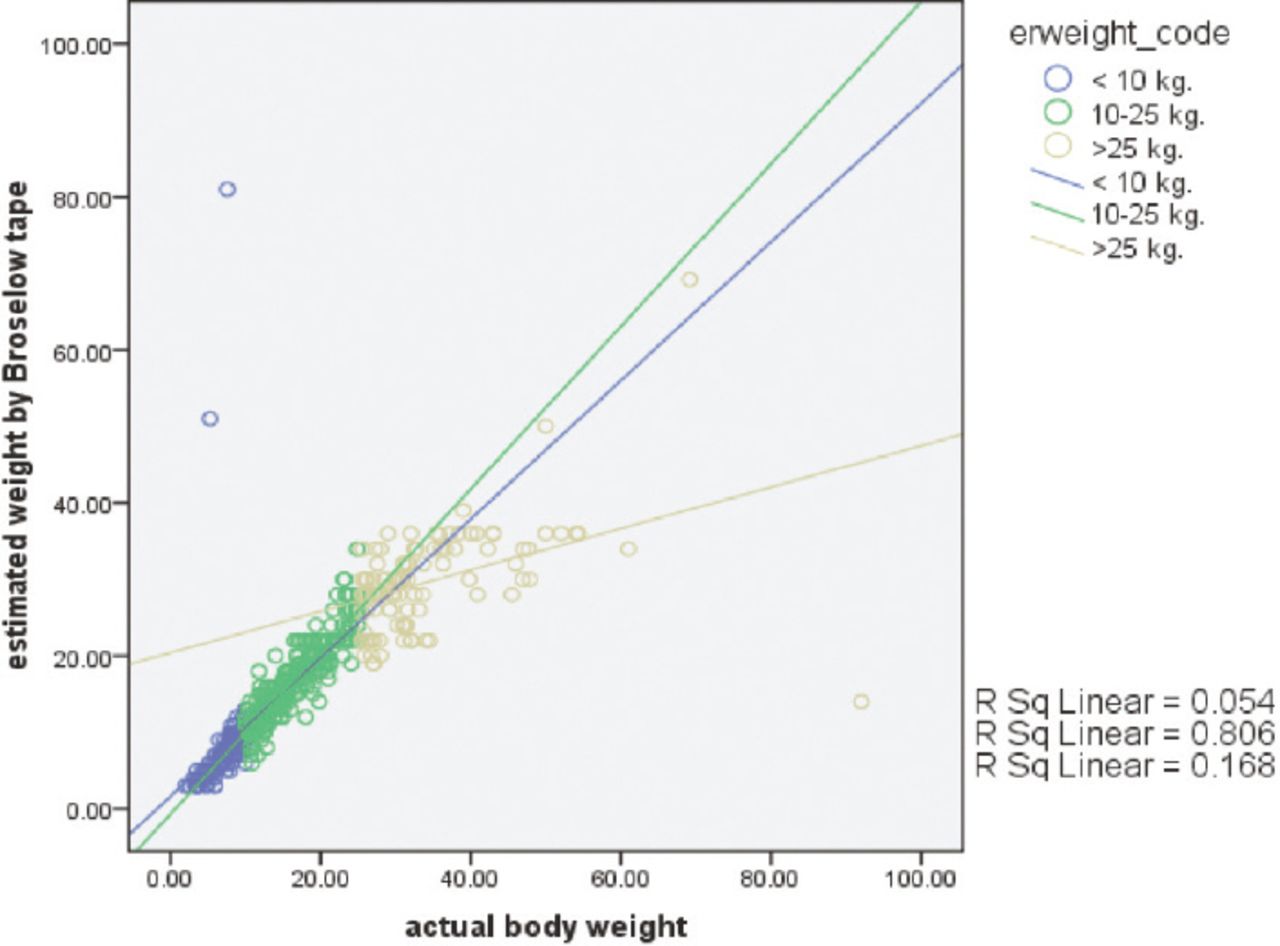
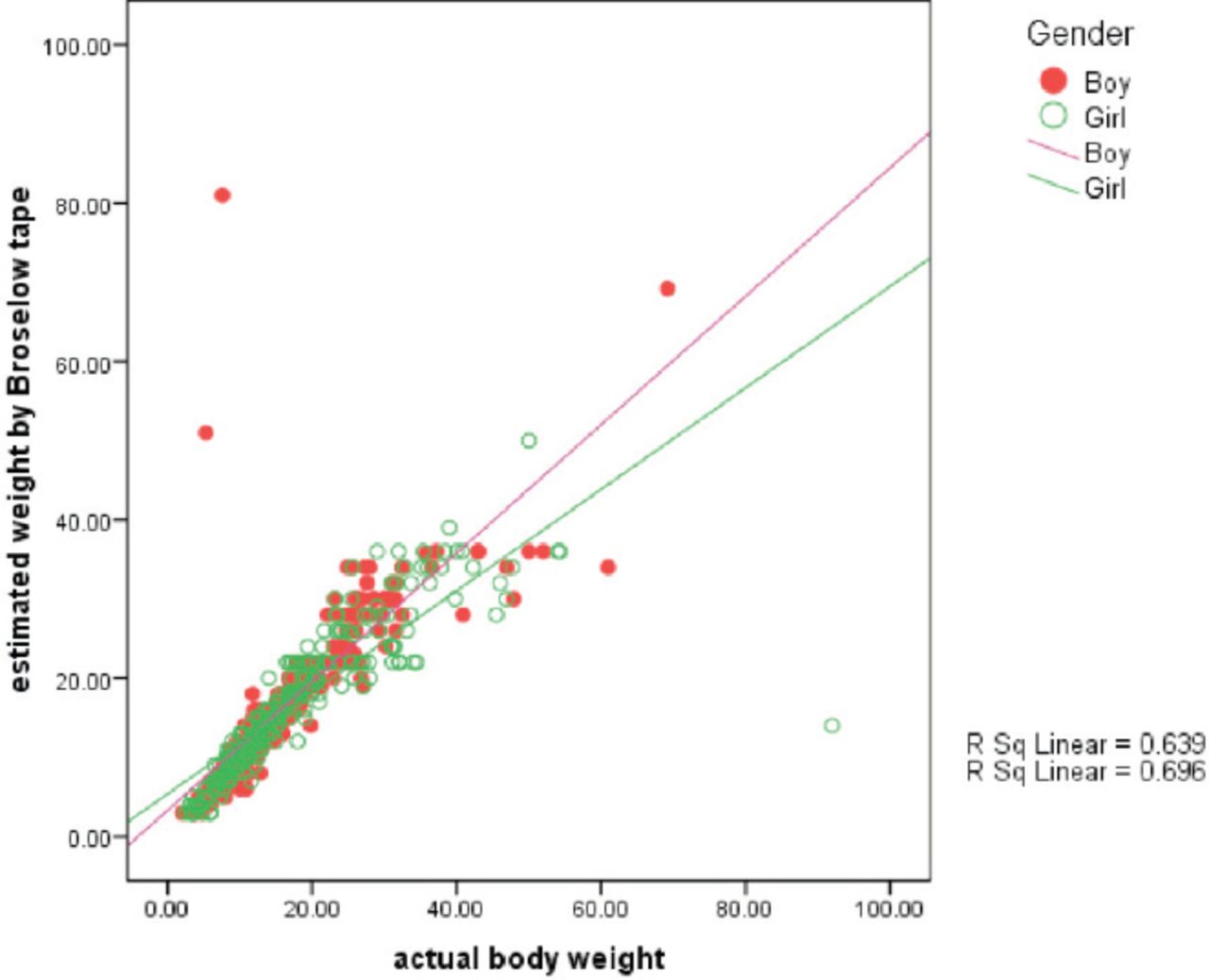
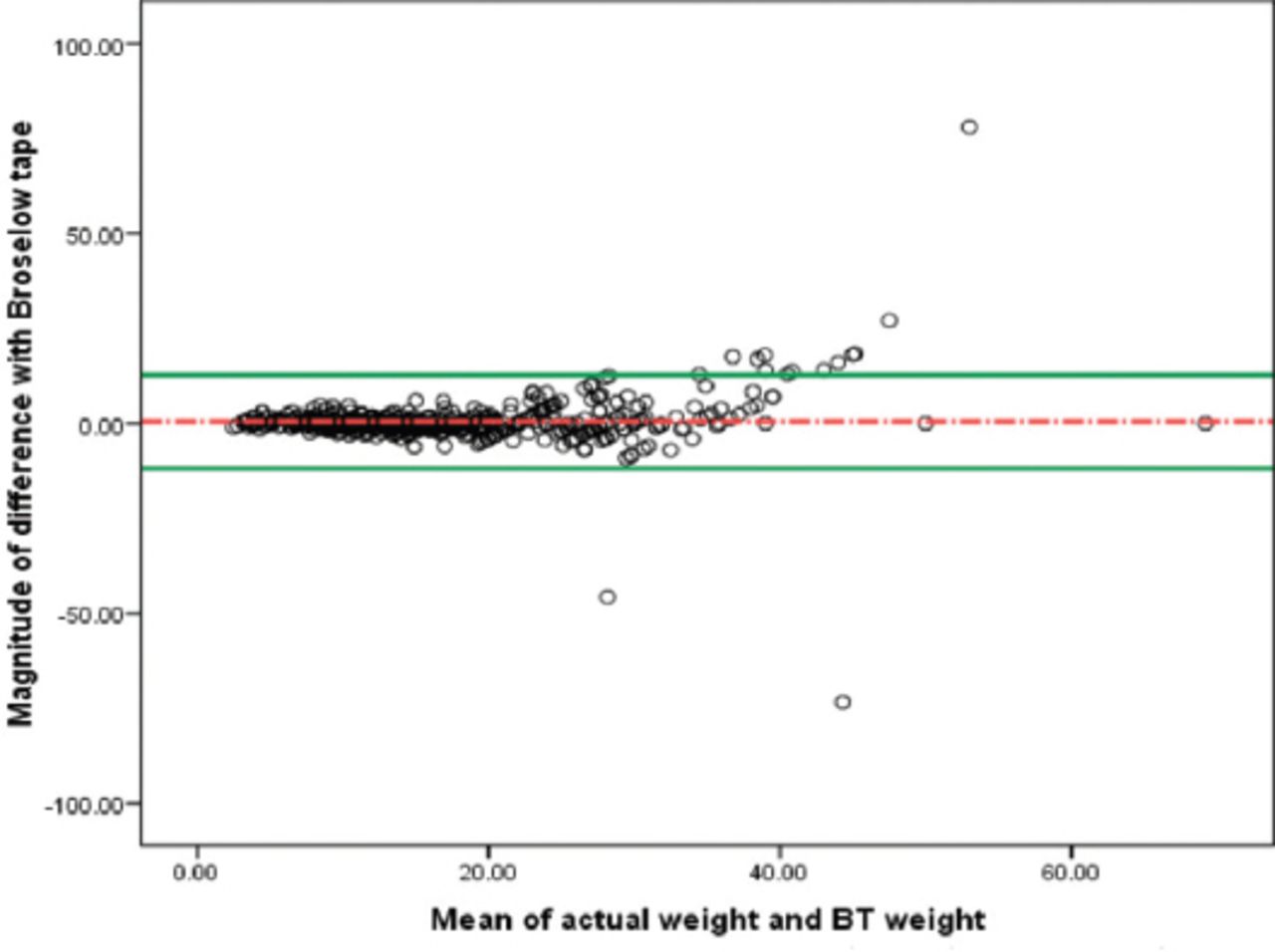
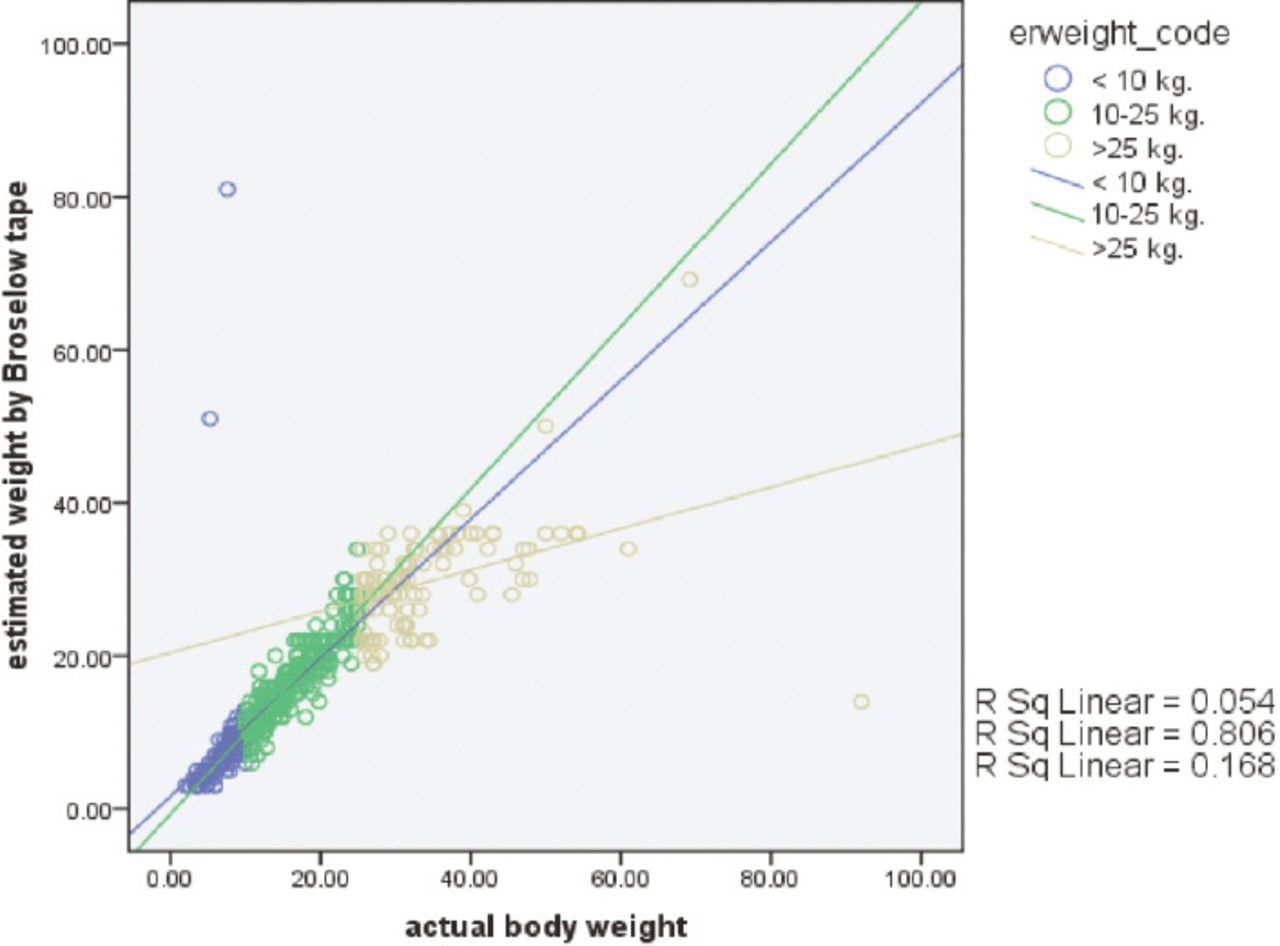
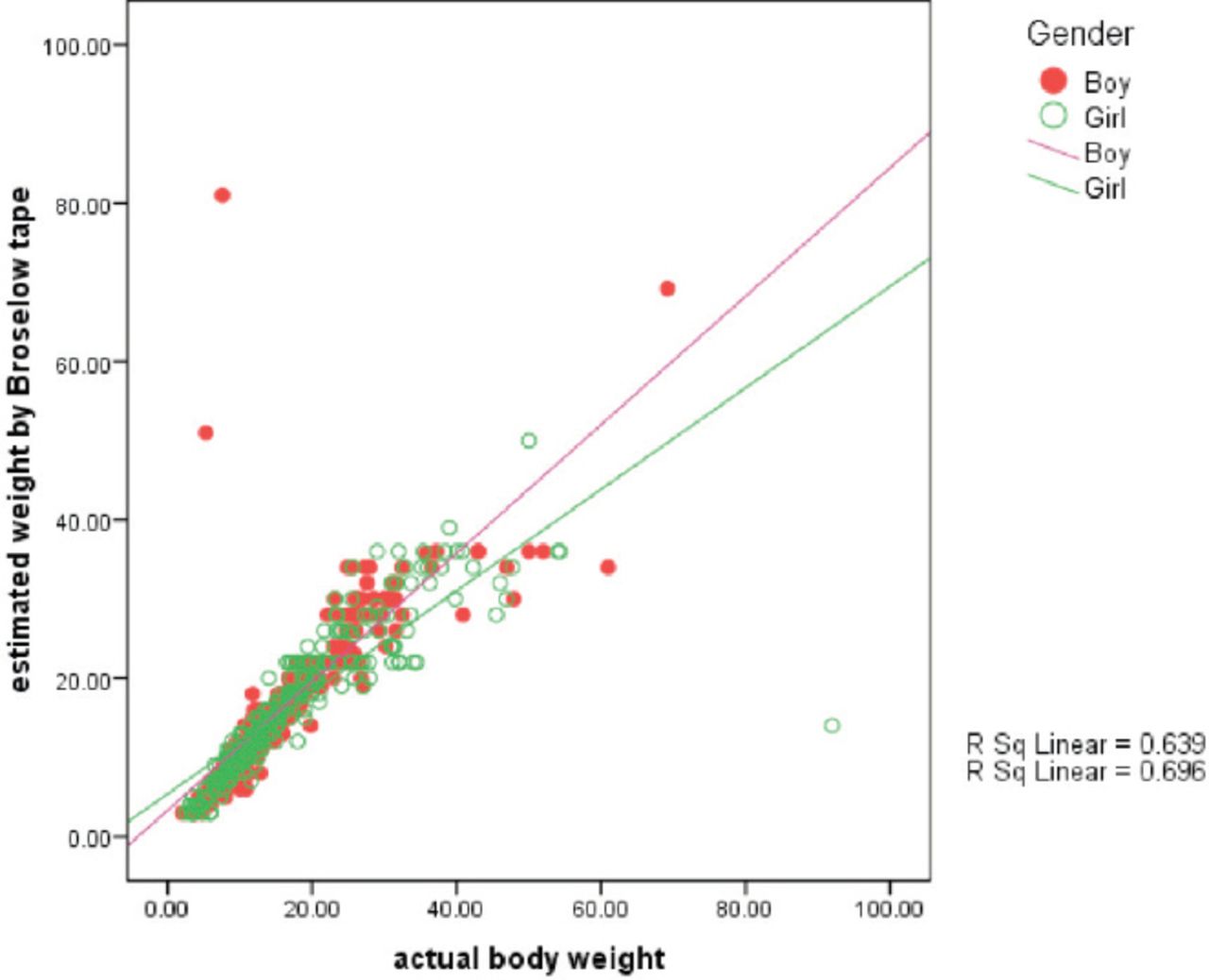
Figure 2 demonstrates that there is a significant agreement between the measurements, but all BPET measurements were not exactly matching with actual standard measurements. It also clarifies that the magnitude of difference was scattered as the body weight increases, which illustrates a high variation for the higher body weight. The accuracy of BPET was tested for the relationship between 2 measurements in both the genders and Figure 3 illustrates that there is no significant difference between boys and girls. A scatter plot was drawn with the actual or standard body weight (Figure 4), which indicates a strong positive relationship between measurements of actual and BPET measured weights in the category of 10 to 25 Kg actual weights (r=0.911, p<0.001). It is also observed that a strong positive association was not established when the BPET body weight measurement falls less than 10 Kg and also when it goes beyond 25 Kg. The data indicate a high level of significance for the correlation of measurement of actual standard weight and BEPT weight for children weighing 10-25 kg. This was the same for both the genders and the different weight groups (Table 1). A strong correlation coefficient and reliability (>0.75) is also observed among the above parameters, except the weight group <10 Kg and >25 Kg.
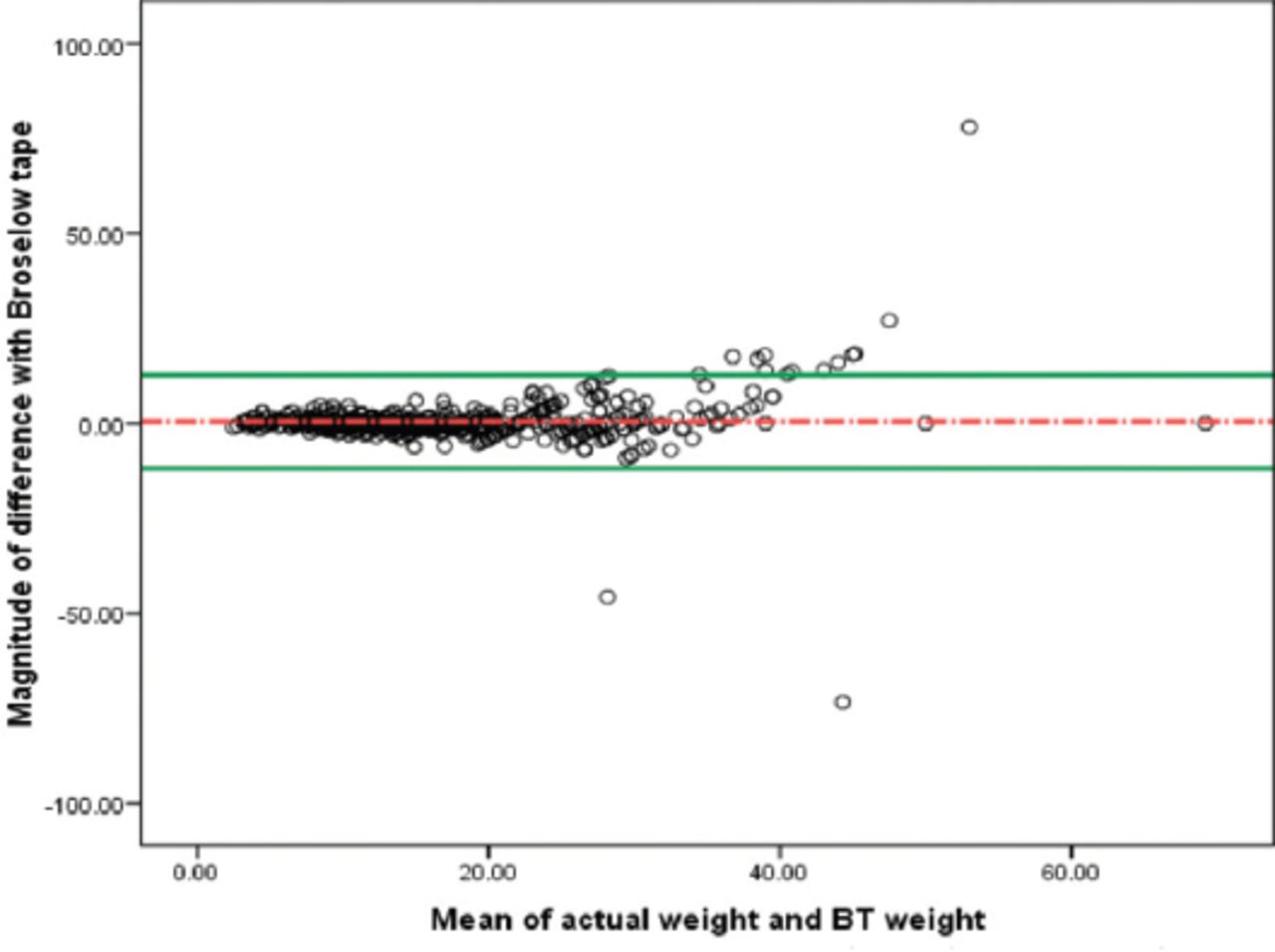
Bland-Altman plot of differences between actual weight and Broselow tape weight.
Scatter plot of measured weight versus Broselow weight by gender.
Scatter plot of measured weight versus Broselow weight by actual weight groups.
Reliability and correlation between actual weight and Broselow tape estimates.
Discussion
The color coded BPET was designed with pre-calculated medication dose to the corresponding weight estimations to combat the problem of weight estimation in emergency situations in pediatric emergency units. The invention was based in the United States population data and is accepted across the globe as an emergency tool to estimate the pediatric weight for rapid emergency management of critically ill children. There were many studies proving its adaptability and efficiency.1,11-14 However, there are several other studies with contradictory findings as well.4-6,15-22 The most recent study conducted by Waseem et al15 concluded that in their population, BPET was inaccurate in predicting weight in 42% of children; moreover, they pointed out that the majority of discrepancies involved only in one BPET color zone. A few studies also discussed their concern of using the BPET estimation of body weight among children in diverse ethnic conditions and children with malnutrition/under nutrition or obesity. A study in an Indian population by Ramarajan et al23 concluded that BEPT overestimates weight by more than 10% in Indian children >10 Kg and in order to overcome the error they suggested a 10% weight-correction factor. Almost a similar conclusion was arrived by Khouli et al24 that the BPET estimated weight was different from the scale weight by more than 10% in a substantial percentage of Mexican children. Clark6 raised their concern that in malnourished and non-malnourished African populations the weight estimation was markedly inaccurate; moreover, it was worse in malnourished children and they suggested further studies to explore appropriate methods of weight and dosage estimation for populations of low and low-to-middle-income countries and regions with a high prevalence of malnutrition. Tanner et al17 studied the possible errors in BEPT body weight estimation among overweight and obese children and suggested that an adjustment factor significantly improved BPET accuracy. In our study, we explored the data for accuracy of measurements in the study population and we observed that the measurements correlated each other well and the authors were able to establish a positive relationship between the measurements, but the data demonstrated only 65.1% accuracy. Further exploration also demonstrated that BPET measurement over estimated higher values and underestimated lower values. The Bland Altman plot provided a significant agreement of mean weight of both standard measurements and BEPT measurements. But, we observed inaccuracy of measurements when the estimated body weight exceeded 25 Kg. Another study reported by Mishra et al,4 concluded that the BPET showed good evidence for being more reliable in Indian children of weight <10 Kg and 10-18 Kg groups and they also had an opinion that as pediatric weight increased, predictive reliability decreased. Sinha et al24 also agree that it is possible to obtain an actual patient weight during pediatric trauma resuscitation with BPET, but they also concluded that the mean error was greatest in the highest weight category. AlHarbi et al1 also reported that accuracy of both BPET versions was adversely affected when age >95 months and weight >26 Kg. Even though there is a high statistical significance in all the BPET measurements, the data was not able to demonstrate the same level of correlation and reliability for the measurements <10 Kg and >25 Kg. This indicates that BPET has a strong relationship and a very high degree of reliability in the measurement of weight from 10 to 25 Kg. When compared to the previous study conducted by AlHarbi et al,1 this study was conducted exclusively in a hospital setting located in the eastern region of the country using Broselow tape version 2011a, whereas the later was conducted in an outpatient clinic and elementary schools in the Central region of Saudi Arabia using Broselow tape version 2011.
In conclusion, even though all the BPET estimated weight significantly correlated to actual weight, the body weight measurements ranging from 10 to 25 Kg were best correlated, and were measured with a high degree of reliability.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 19, 2017.
- Accepted May 17, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}
{kind=link}