


Abstract
Objectives: To examined published literature describing the predictors of smoking cessation (SC) and cessation interventions in Gulf Cooperation Council (GCC) countries.
Methods: Systematic literature review using PubMed, Google Scholar, and grey literature. The study was conducted between October and December of 2017. Inclusion criteria were studies reporting factors associated with SC or studies of utilization or delivery of SC medications in GCC countries.
Results: Twenty-one articles met the study criteria. Thematic analysis revealed factors associated with SC that were classified as individual or clinician level. Individual-level factors were access and cost of SC medications, knowledge about harms, concern about health, self-efficacy, perceived stress, level of tobacco consumption, belief about SC medications, clinician advice, social support, and enforcement of smoke-free ban. Clinician-level factors were time to provide counseling, training to assist patients, patient acceptance, best practice for treating patients, resources, perception related to responsibilities, and knowledge about effective medications.
Conclusion: This review revealed perceived barriers to SC among smokers and clinicians in GCC countries. It highlighted cultural factors that need to be addressed by tobacco use policies in GCC countries to help smokers quit.
The Gulf Cooperation Council (GCC) is an intergovernmental political and economic union comprised of 6 countries: Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, and United Arab Emirates (UAE). Gulf Cooperation Council countries share not only political and economic interests but also social and health affairs. They have a similar environment, culture, and life style that are associated with similarities of health risk factors. Gulf Cooperation Council countries also have similar trends in health indicators; for instance, recent trends across these countries show a decrease in the crude mortality rate and improve in the life expectancy.1 Tobacco use is a major public health problem in the GCC countries. It is associated with personal characteristics and social context including the family and peers, community, and public policy.2 Tobacco use has become culturally popular in GCC countries, social norms regarding tobacco use likely would influence community members.3 Cigarettes are the main form of tobacco use among smokers; water pipe is the next popular tobacco product, especially among women and youths. The increase use of water pipe may reflect misconceptions of reduced harm and addiction to users, the variety of flavor available, and the poor public health policies aimed at tackling this alternative form of tobacco use.4 The highest smoking prevalence rate among men occurs in Kuwait (35.4%) while the lowest prevalence is in Oman (12.3%). The highest reported smoking prevalence rate among women appears in Bahrain (5.7%) while the lowest rates are in Oman and Qatar (0.1%).5 A particular concern is the high smoking rates among adolescents and young adults. Tobacco use rates among young men in the GCC countries range from 4.9% in Oman to 25% in Bahrain, while rates among young women range from 1.7% in Oman to 10.1% in Bahrain.6 The GCC countries provide free of cost healthcare services to their citizens, who expressed their satisfaction toward the quality of delivered services.7 The GCC national governments provide access to smoking cessation (SC) treatment including Bupropion (namely, Zyban®, Wellbutrin®), nicotine replacement therapy (NRT) (patch, gum, lozenge, spray or inhaler), and Varenicline (Chantix®) in diverse healthcare settings. The cost coverage of the SC medications varies across the GCC countries. Qatar and Saudi Arabia offer full cost coverage for all types SC treatments while UAE covers the partial cost of them. Bahrain and Kuwait provide coverage for NRT products only, but Oman does not cover the cost of all SC medications.5 The GCC policy of governments offering SC treatment is a significant policy to help individuals quit smoking. Efforts to successfully facilitate SC treatment need to be culturally relevant. To enhance SC among GCC countries, information is needed on the individual and clinician-related factors associated with SC treatment policy in these countries. No published manuscript has provided a systematic review on these key areas. In this paper, we conducted a systematic literature review to examine the predictors of SC and interventions to facilitate cessation among smokers in the GCC countries.
Methods
A comprehensive search of published research on PubMed and Google Scholar was conducted between October and December of 2017. The following keyword searches were used in the electronic databases: (smoking OR tobacco products OR tobacco use OR tobacco use cessation OR tobacco use disorder OR smoking cessation) AND (Bahrain OR Kuwait OR Oman OR Qatar OR Saudi Arabia OR United Arab Emirates OR GCC countries OR Gulf Cooperation Council). In addition, relevant grey literature was identified using GCC country governmental websites in order to reduce any possible publication bias. This study was designed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guideline.
Eligible studies included all age groups, male and female individuals who live in the GCC countries as a citizen or resident. Studies that collected information about factors associated with SC or studies about utilizing or delivering SC medications from either smokers or clinicians were included. Studies examining cessation with all forms of tobacco were eligible, including, but not limited, chewing tobacco, cigarettes, cigars, dip, electronic cigarette, midwakh, dokha, shisha, and waterpipe. All types of SC medications, both NRT and non-NRT (bupropion and varenicline), were considered. We included qualitative and quantitative studies, randomized clinical trials (RCTs), quasi-experimental studies, and observational studies. The expanded inclusion criteria were developed as an effort to collect all relevant information about SC in the GCC countries. Finally, we excluded studies that published before 2005, not in English, conducted in non-GCC countries, and did not include human data. Letters to editors, reviews, comments, and correspondences identified during the search process were excluded.
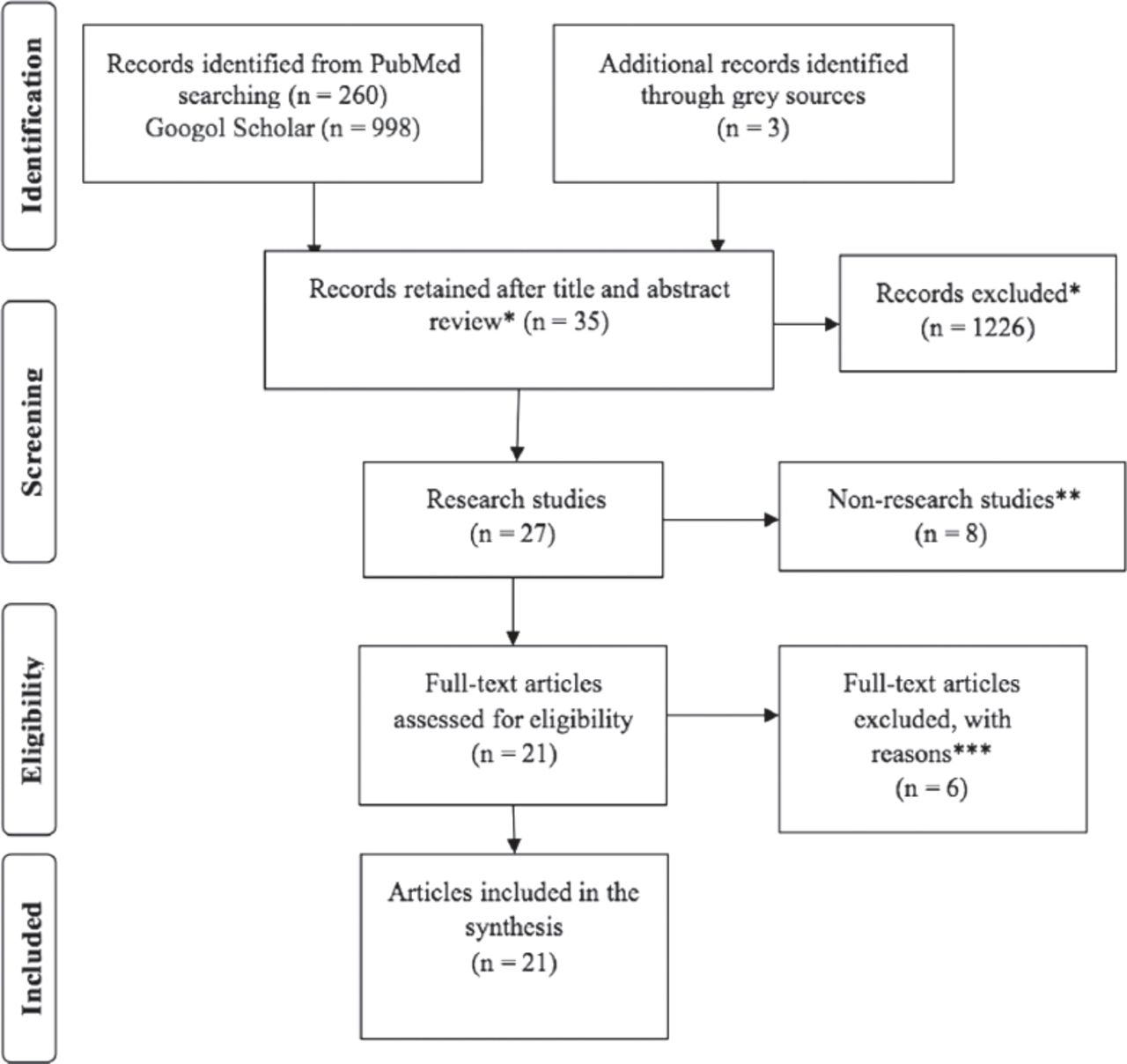
The initial online database searches by using the above keywords yielded 1261 articles in total (PubMed (n=260), Googol Scholar (n=998), and grey literature (n=3). These studies were reviewed based on their titles and abstracts. After resolving duplicate, removing irrelevant articles, the eligible articles became 21. Full-text of these studies were obtained to apply the inclusion/exclusion criteria for further review (Figure 1).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram depicting the selection of papers at each stage. Note: Records excluded for the following reasons. *Excluded results that were unrelated to the topic of the review or duplicates. **Letter to the editor (n=2), review (n=2), correspondence (n=1), a medical guideline (n=1), and governmental documents (n=2). ***unstated outcomes (n=1), included Yemen as a pervious GCC country (n=1), had non-smoking patients (n=1), had no interventions (n=3)
The quality of evidence strengthens the causal inferences. All eligible studies were given a grade. To assess the quality of each study, we utilized the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) model. The GRADE model would determine the range of the confidence that estimates the effect of the policy. The GRADE model has 4 primary grades: high, moderate, low, or very low. The quality of evidence was assessed based on 4 essential elements: study design, study quality, consistency, and directness (Appendix 1).8
Quality of Evidence Grades*.[8]
Data from eligible studies were extracted and summarized in a spreadsheet. The extracted data were organized as author names, year, country, study setting, study design, population, outcomes relevant to SC use and deliver, and information needed to examine the risk of bias of each study naemly, randomization protocols, and response rate in cross-sectional studies (Appendix 2).9 Due to the diversity of articles in term of countries, populations, and settings, the results did not appropriately fit the meta-analysis method of synthesis. The findings were reported by narrative summary and realistic synthesis in which evidence was selected, recorded, and analyzed to enhance the causal inference of the policy and its outcomes.10
Results
A total of 21 articles met the eligibility criteria and were included in this review. Studies were one experimental study, namely, RCT; 20 observational studies: one prospective cohort study obtained from the grey literature, and 19 cross-sectional surveys, one of them from grey literature. The quality of studies was graded as high (4.8%), moderate (28.6%), low (28.6%), or very low (38.1%). The number of the included articles based on their countries ranged from zero to 9 articles. The majority of studies were conducted in Saudi Arabia while no article was found from Oman (Table 1) (Appendix 2 provides a detailed summary of studies).
The percentage of yielded articles based on their countries.
Summary and quality grade of studies included in the review by study design*.
Experimental study
Only one RCT study was included in this review that was graded based the randomization protocol and its outcomes.
High quality of evidence
The RCT study was conducted in Qatar and was graded as a high quality of evidence. It was primarily evaluated based on the randomization that gave equal probability of a smoking individual to be assigned to either sample or control group. Procedures were controlled to assure that all subjects were treated the same except for the SC services given to the smoking participants in the sample group. Outcomes were measured using the continuous abstinence at 12 months and the daily number of cigarettes smoked. El Hajj et al11 examined the effectiveness of trained ambulatory pharmacists in delivering SC services (both therapeutic and behavioral interventions). They recruited 314 smoking adults, 97.8% of them were men who were other than Qatari or Egyptian. After adjusting for nationality, the reviewed RCT study found no statistically significant differences between intervention group and control group. But the daily number of cigarettes at 3 and 6 months for those who relapsed had significant reductions compared to control group at 95% CI (p=0.041, p=0.018,).11
Observational studies
Multiple cross-sectional studies were included. These studies used survey questionnaires and narrative findings. The quality of evidence of the observational studies ranged from moderate to very low. The grade was given based on the reliability and generalizability of methods and outcomes.
Moderate quality of evidence
A total of 6 moderate studies were included. A study assessed the changes in scores of implementing tobacco use policies, including SC programs and smoke-free policy, in the Eastern Mediterranean region. The cessation program was evaluated by the authors who used a checklist that had scores ranged from 0 to 4 (0= unavailable data, 1= none, 2= NRT and/or some cessation services [neither cost-covered], 3= NRT and/or some cessation services [at least 1 cost-covered], 4= national quitline, and both NRT and some cessation services cost-covered). The GCC countries’ scores in cessation programs have fluctuated. From 2011 to 2013, the scores were improved in Kuwait (3 to 4), declined in Bahrain (4 to 3) and Saudi Arabia (4 to 3), and stabilized in Oman (2), Qatar (3), and UAE (4). According to the grade of smoke free policy, Bahrain, Qatar, and UAE did not report data while Kuwait, Oman, and Saudi Arabia improved their compliances with the policy.12
Two cross-sectional Kuwaiti studies explored the predictors of SC among governmental employees and industrial workers. The first study found that personal self-efficacy is a significant predictor for quitting among governmental employees. The self-efficacy could be developed through the short duration of smoking and less daily cigarette consumption.13 In the second study, industrial workers who intended to quit received NRT mainly patches. More than 50% of the quitters (abstinence from tobacco for >3 months) reasoned their quit to the knowledge of the harmful effect of smoking on health, 12.4% stated physician advice, and 6.5% reported cost reasons. The study also found a significant association between smoke-free workplace policy and quit rate (OR=3.58).14 One study from Bahrain provided information about the effectiveness of the quit tobacco clinics that improved access to free SC medications. About 93% of male smokers, 80.6% of them were Bahraini, used NRT and counseling sessions. Only 11.7% had to purchase NRT from private entities, 7.2% of them found the cost unaffordable. Results showed that 56.5% of participants quitted all tobacco forms. Compared to tobacco smokers, shisha smokers were more successful in quitting. The study found a significant statistical relationship between successful quit and number of previous quit attempts at 21 months duration and number of clinic visits.15 Two Saudi studies assessed the feasibility to deliver SC medications among physicians. Lack of time and training were the main reasons that discourage physicians from delivering SC services. Ninety-six percent of general and family practitioners, who worked in 2 academic medical centers in Riyadh City, had not prescribed SC pharmacotherapy to their patients.16 Similarly, at least 50% of family practitioners, general internists, cardiologists, and vascular surgeons in four regions of Saudi Arabia would not advice smokers who have history of heart diseases to use SC medications.17
Low quality of evidence
Six studies were graded as low quality of evidence. Two Saudi studies investigated quit motivational factors among smokers and quitters. The intention to quit among school-age youths was associated with the level of tobacco consumptions, the perceived knowledge about the dangers of smoking, and the cost of tobacco.18 Recently, Abdelwahab et al19 assessed adult smokers’ perception of the effectiveness of cessation interventions. The majority agreed that school-based intervention and media awareness are proactive approaches, and 70.9% of participants believed that NRT is an effective method for cessation.19
In a Bahraini study, waterpipe smoking adults in Cafés were surveyed to explore reasons behind intention to quit. Researchers found that receiving physician advice, opposing families to waterpipe smoking, and considering oneself as an unhooked were the main predictors of quit intentions.20 In a Saudi prospective cohort study, Alraihan21 (2016) looked at the feasibility of offering SC treatment by comparing mobile SC clinics to fixed clinics in ten regions. Mobile SC clinics, where NRT given for free, leaded to 55.74% quit attempts across both genders and all age groups while fixed SC clinics had 44.26% quit attempts.21 In term of clinicians, 2 studies focused on the feasibility around delivering SC medications among different medical specialties in Saudi Arabia and dentists in Kuwait. Studies reported multiple reasons hinder the advice and assistance including insufficient time, inadequate training, unclear guideline, and patient resistance to and compliance with physician advice.22,23
Very low quality of evidence
Eight studies were evaluated as a deficient quality of evidence. Two cross-sectional studies surveyed smoking adults in Saudi Arabia and UAE about their perceived factors that affect their decision to quit smoking. Knowledge of harms, health concerns, self-willpower, social support, and level of stress were mentioned in these studies.24,25 Six studies assessed the feasibility of delivering SC services across diverse health practitioners including general physicians and nurses in UAE, dentists in Saudi Arabia, primary care physicians in Bahrain, and pharmacists in Qatar. Barriers to advice smokers included lack of resources namely, educational materials and referral agencies, patient resistance, inadequate skills, perceived unrelated jobs, and limited time.26-31 Two studies of them reported the lack of knowledge about non-NRT such as Bupropion.
Themes from included studies
Table 2 presents themes that were found in the included studies. Themes were categorized into 2 groups: factors influencing the utilization of SC treatment at the individual level and factors affect the delivering of SC medications at the clinician level. At the individual level, access to SC medications, cost of medications, concern about health, and social support were more often stated in the literature review. Other factors were knowledge about the harms of smoking, self-efficacy, perceived stress, level of tobacco consumption, belief on the SC pharmacotherapy, clinician advice, and enforcement of smoke-free policy in public and workplace. At the clinician level, time for counseling smoking patients, training to assist patients, patient acceptance, and knowledge about the effective SC medications were more frequently stated in the included studies. Other factors involve best practice evidence for treating and refereeing smoking patients, resources, namely, educational materials and referral clinics, and perception related to responsibilities.
Themes emerging from the thematic analysis.
Discussion
This review examined studies that explored factors associated with SC and use of SC medications in the GCC countries. The grading of evidence and the analysis of themes helped in assessing the SC treatment policy. The GCC countries show success in addressing tobacco epidemic. Since the availability of SC treatment promote cessation among tobacco users, the GCC governments provide fully and/or partially coverage for SC medications for their citizens.6 Despite the GCC countries’ efforts to facilitate SC treatment, there were perceived barriers that discourage the use and delivery of the SC medications. From the individual perspective, the availability of SC medications in the GCC countries did not enhance the utilization because of the lack of social support, access constraints, and cost challenges facing smoking population who pay (at least partially) for these medications.32 In addition, clinicians were less likely to advise patients to quit and recommend use of SC medications due to their limited time with patients and inadequate training to deliver SC services.
The shortage of physicians in GCC countries may explain physicians’ barriers to deliver SC treatment.7 Therefore, most GCC countries made an effort to expand access to SC services by increasing the number of cessation clinics and involving non-physician clinicians such as nurses and pharmacists to deliver SC services. Moreover, sociocultural factors in GCC countries could illustrate the barriers to use SC medications and quit smoking. GCC populations are influenced by their peers and families, which are critical units in the community.33 Since the tobacco smoking became culturally popular in GCC countries, efforts need to be exerted to reduce the visibility of smoking in public. Smoke free policies in public and private entities should be well implemented and enforced to create antismoking norms, motivate smokers to quit, and protect individuals from the harmful effects of exposure to secondhand smoke.
Study limitations
We were not able to identify studies that provided accurate data on the use of SC treatment, and we found few studies of clinicians’ attitudes in delivering SC medications. This review could not quantify the actual effect of GCC policies affecting the use of SC medications due to limited information. Furthermore, the inference should be made by cautious. Although the GCC countries have similar cultures, individuals’ characteristics in each country are different.
Health policy research is a new field in the GCC countries. Therefore, future research with strong study designs and methodologies are needed to assess the effectiveness, efficacy, equity and feasibility of tobacco control measures. In particular, studies are needed to examine whether SC treatment policy can successfully help smokers to quit and tackle the use of tobacco in GCC countries.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 31, 2018.
- Accepted January 1, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}