


Abstract
Objectives: To investigate prevalence and association between iron deficiency anemia (IDA) and Helicobacter pylori (H. pylori).
Methods: This cross-sectional study included 79 participants with unexplained IDA. The study was carried out between November 2018 to April 2020 in the College of Medicine, Umm Al-Qura University in collaboration with Al-Noor Specialist Hospital, Makkah, Saudi Arabia. Complete blood count (CBC), serum iron, and ferritin levels were measured. Anti-H. pylori antibody was detected using anti-H. pylori immunoglobulin G enzyme-linked immunosorbent assay (ELISA).
Results: The prevalence of H. pylori infection among IDA patients was 62%. There was a significant difference between female and male subjects with a positive H. pylori status (p=0.001). There was also a significant difference between females and males with a positive H. pylori infection according to red blood cell count, hematocrit, mean corpuscular volume, and mean cor-puscular hemoglobin (p=0.001).
Conclusion: The current study shows an association between H. pylori infection and unexplained IDA with significant difference between postmenopausal Saudi females and males. This will lead to more effective treatment in IDA and the eradication of H. pylori, as well as the prevention of recurrence, which are necessary and may provide a significant reduction in the overall disease burden.
The World Health Organization (WHO) recently identified anemia as a world public health issue, as 1.62 billion members of the world’s population are anemic.1 Iron deficiency is commonly assumed to cause most anemia worldwide and is responsible for 75% of all third-world anemia cases, affecting 30% of the population.2 The average prevalence of iron deficiency anemia in Saudi Arabia is 30%-56%.3 Established causes of iron deficiency include when iron consumption is low, iron absorption is poor, or frequent iron losses occur beyond small bowel absorption. If the iron balance cannot be preserved, iron reserves will slowly decline, and iron deficiency anemia (IDA) will develop.4 In addition to the above mentioned causes, iron deficiency anemia may occur as a result of chronic gastrointestinal (GI) blood loss, which is the greatest common effect in males and postmenopausal females.3,5
Half of the world’s population is believed to have Helicobacter pylori (H. pylori), with higher prevalence in developing countries.6 It is a spiral shaped gram-negative pathogenic bacterium, which inhabits the gastric epithelium directly, causing a variety of acute and chronic gastrointestinal disorder, including peptic ulcer disease, chronic gastritis, or gastric disease.7 Away from the stomach, over 50 extra-gastric manifestations of H. pylori involving IDA have been recorded.8
Helicobacter pylori is possibly responsible for iron deficiency anemia through several mechanisms, including occult chronic GI bleeding due to gastric mucosal micro-erosions. Hypochlorhydria can allow ascorbic acid to be converted to dehydroascorbic acid, a less active form that prevents iron absorption by reducing the ferric to the ferrous form, which is important for non-haem iron absorption.9,10
Helicobacter pylori competes with the host for iron absorption by possessing certain outer membrane proteins that facilitate tissue lesions, in particular cytotoxin-associated gene A (CagA), vacuolization cytotoxin A (VacA), and heat shock proteins (HSPS),11,12 which play a role in the absorption of bacterial iron and intracellular storage of ferritin-like proteins.13 Efficient eradication of H. pylori in patients with unexplained IDA leads to the improvement of hemoglobin, iron, total blood-binding ability, and ferritin levels.5
The goal of this study was, through a cross-sectional study, to measure the prevalence of H. pylori infection among patients with IDA of unknown etiology in Saudi patients; as well as, to assess H. pylori infection association with hematological parameters among these patients.
Methods
A cross-sectional study was conducted on 79 Saudi patients (31 males and 48 females) who were diagnosed with IDA of an unknown cause, and the mean age was 42.62 ± 10.82 years old (range 21-68 years). Patients who were registered through the current study had dyspepsia and epigastric and vague abdominal pain. Patients with chronic or hemorrhagic disorders, celiac disease, overweight or obese or inappropriate weight loss, IG bleeding, chronic diarrhea, intractable vomiting, acid suppression medication, or new proton pump inhibitor (PPI) therapy were excluded. Thirty age- and gender- matched healthy volunteers as a control were enrolled in the current study which was conducted in the College of Medicine, Umm Al-qura University in collaboration with Al-noor Specialist Hospital, Makkah, Saudi Arabia, between November 2018 and April 2020. The ethical approval was obtained from the Research Ethics Committee of Faculty of Medicine, Umm Al Qura University, Makkah, Saudi Arabia, and all patients and volunteers provided informed consent form. Adequate blood samples were collected. Blood was drawn and placed in standard ethylenediamine tetraacetic acid vacutainers for analysis the complete blood count (CBC) assay and plain tubes for anti-H. pylori immunoglobulin G (IgG) antibody assays, iron and ferritin. The separated serum was split into aliquots. One aliquot was used for ferritin and iron estimation, and the remaining aliquots were kept at 70°C for anti-H. pylori IgG antibody estimation.
Diagnosis of iron deficiency anemia
A hemoglobin levels of <13 g/dL in male subjects and <12 g/dL in female subjects were identified as IDA according to WHO criteria.14 The mean corpuscular volume (MCV) was <80 fL, the serum iron was <37 g/dL, and the serum ferritin was <13 ng/mL. Electro-chemiluminescence (Elec Sys 2010 analyzer; Roche Diagnostics, Mannheim, Germany) was used to evaluate serum ferritin levels, while a CobasIntegra700 analyzer was used to determine serum iron levels (Roche Diagnostics, Basel, Switzerland). The CBC assays were carried out on a SysmexSE-9000 automated analyzer (Kobe, Japan), which was calibrated regularly with the manufacturer’s standards.
Determination of anti-H. pylori IgG
For evaluation of H. pylori satus, the titer of anti-H.pylori antibodies was measured, using anti-H. pylori IgG enzyme-linked immunosorbent assays (ELISA) to detect and evaluate qualitatively serum IgG antibodies to H. pylori infected subjects. A value less than 0.9 was deemed negative for the presence of detectable IgG antibodies against H. pylori, while a value greater than 1.1 indicated positive IgG antibodies against H. pylori.
Statistical analysis
The Statistical Package for Social Sciences, version 20 (IBM Inc., Chicago, IL, USA was applied for all statistical analyses. Continuous (numerical) data are represented by the mean standard deviation, while categorical (discrete) data are represented by numbers (percentages). The student’s t-test and the Mann-Whitney U test were used to assess if there were statistically meaningful variations between classes. The Pearson correlation test was used to measure correlation coefficients. P-values <0.05 were regarded as important.
Results
Prevalence of H. pylori
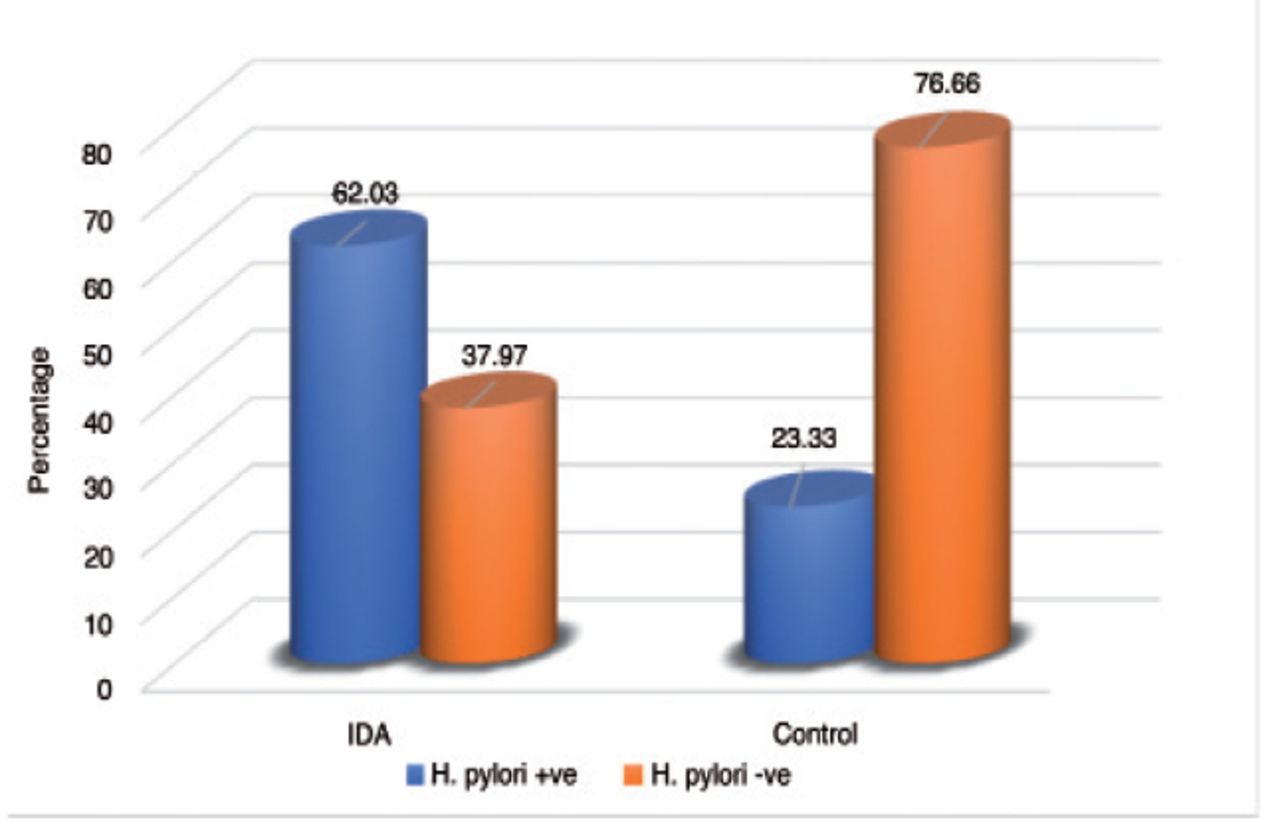
Seventy-nine percent with unknown causes of IDA who participated in our study, 31 males (39.2%) and 48 females (60.8%) with ages ranging from 21 to 68 years (mean age: 42.62 ± 10.82 years) were included. The healthy controls involved 18 (60%) men and 12 (40%) women, with a mean age of 37.6 ± 11.84 years. In IDA patients and non-anemic healthy controls, the prevalence of H. pylori infection was 49 out of 79 (62.03 %) and 7 out of 30 (23.33 %), respectively. This distinction was statistically important (p=0.001) (Figure 1).
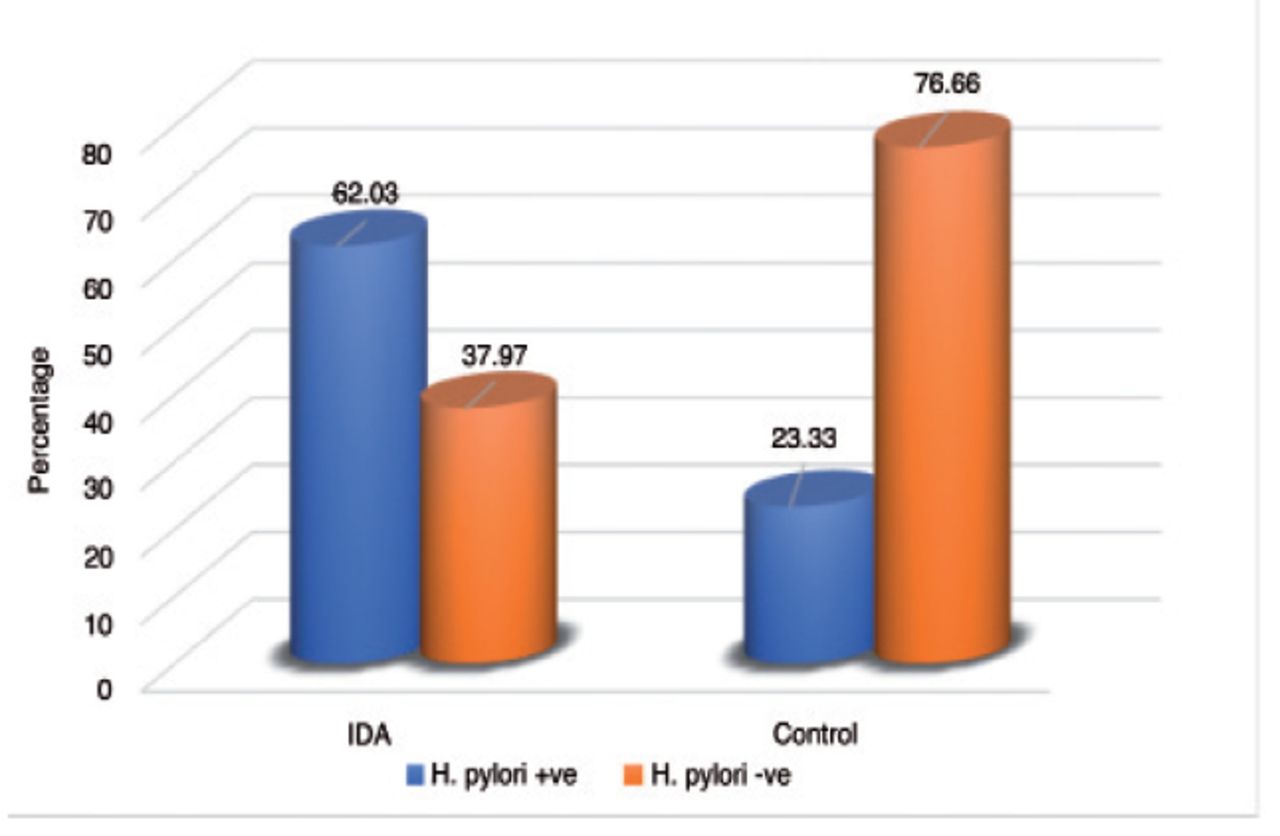
- Prevalence of H. pylori in the unexplained iron deficiency anemia and control groups. IDA, unexplained iron deficiency anemia group (n = 79); HC, healthy control group (n = 30). Mean values were significantly different between groups (p<0.001). H. pylori: Helicobacter pylori, +ve: positive, -ve: negative
Hematological parameters among IDA and control group
Table 1 displays the hematological results. Hemoglobin values were smaller than the reference range of 12 g/dL, with a mean value of 9.7 ± 1.17 compared to 13.94 ± 0.80 in the control group (p=0.0001). Values of the red blood cells (RBCs) count, mean corpuscular volume (MCV), hematocrit (HCT), and mean corpuscular hemoglobin (MCH) of the patients in the study group were all lower than those of the control group, which was not surprising. Furthermore, serum iron and serum ferritin levels in IDA patients were found to be relatively higher than in non-anemic healthy controls (p=0.0001).
- Hematological data of the patients with unexplained iron deficiency anemia.
Detection H. pylori of IgG antibodies
Since IgG antibodies are by far the most specific type of anti-bodies for detecting H. pylori infection, we examined IgG antibodies in 79 IDA patients and 30 controls for confirmation of H. pylori infection. Anti-H. pylori IgG antibody status was used to classify the IDA patients into 2 groups; H. pylori-positive as group I and H. pylori-negative as group II. There was a strong association (p=0.002) between positive (n=49, 62%) and negative (n=30, 38%) H. pylori status (Table 2).
- Hematological characteristics in patients with and without IDA with positive and negative Helicobacter pylori (H. pylori)infection, compared to the controls.
Hematological characteristics in IDA with positive and negative H. pylori
In both the male and female sample groups, there was a significant difference between the IDA group and those with and without H. pylori infection (p=0.01). However, there were no statistically meaningful discrepancies in RBC, hemoglobin (Hb), HCT, MCV, MCH, serum iron, or ferritin levels between IDA patients with and without H. pylori infections (Table 2). In comparison, there was a statistically significant discrepancy in hematological parameters (RBC, Hb, HCT, and MCV) between patients and control subjects with a positive H. pylori status (p<0.0001). Furthermore, the serum iron concentration and serum ferritin levels in H. pylori-positive IDA patients were slightly higher than in H. pylori- positive non-anemic controls (Table 2). The prevalence of positive H. pylori status in female IDA patients was found to be substantially higher than in male IDA patients (p=0.001).
Unexpland IDA and positive H. pylori in males and females
Table 3 displays a significant relationship between male and female IDA patients with positive H. pylori status and all hematological parameters (p=0.001). Also, Table 3 shows that serum iron and ferritin levels were slightly lower in female H. pylori-positive IDA patients than in male H. pylori-positive IDA patients (p=0.001).
- Corelation between unexpland IDA and positive H. pylori status in males and females.
Discussion
The present cross-sectional study aimed to evaluate the H. pylori infection prevalence in Saudi patients with unexplained IDA, as well as to explore the association between H. pylori infection and the hematological parameters of these patients. Inadequate iron consumption, inadequate iron absorption, or when normal iron losses exceed the small bowel’s capacity to absorb iron can result in the loss of iron stores. Iron deficiency anemia is considered a major public health problem. At the same time, H. pylori is a common infection of the GI tract, affecting most of the population.15,16 Although the guidance on IDA has confirmed the etiological role of H. pylori in IDA, the relationship remains controversial. The most frequent reason for nutritional deficiency causing anemia in clinical practice is iron deficiency.17 The results of the current study illustrate that 62.3% of patients with IDA were positive for H. pylori infection. Iron deficiency anemia can occur as a result of H. pylori infection through active hemorrhage secondary to gastritis, peptic ulcers, or gastric cancer, achlorhydria caused by chronic pangastritis, and iron utilization by bacteria for colonization.18-20
Several previous studies have found a high incidence of H. pylori in patients with unexplained or refractory IDA, proving these results. Demerdash et al6 reported that in patients with unexplained or refractory IDA (61.5%), H. pylori infection is more prevalent than in healthy controls (14.3%). Hershko et al21 reported that in 55% of the patients examined (n=300) with unexplained IDA, H. pylori infection was the common coexisting finding. Another retrospective study by Xu et al22 noted that the prevalence of anemia among the study group was 5.5% (428/7804) in infected subjects with H. pylori, in comparison to 5.2% (522/9987) in subjects without H. pylori infection.
The current study found a significant difference in hemoglobin concentrations between patients with positive H. pylori status with IDA and the control subjects (p<0.0001). Additionally, there was a significant difference between female and male subjects with positive H. pylori status (p=0.001). With regard to this finding in the current study, our female patient population consisted of postmenopausal-aged women to exclude other significant causes of female anemia, such as different gynecological and sociodemographic variables (fertile age, pregnancy, and lifestyle). Xu et al22 reported a lower value of hemoglobin in the infected group with H. pylori for male patients.
The results of our present study showed a significant difference between females and males with a H. pylori infection in terms of RBC, HCT, MCV, and MCH (p=0.001). In addition, the present study illustrated a significant difference in serum iron concentration and serum ferritin levels in patients with a positive H. pylori status and control subjects (p<0.0001). A significant difference between males and females in our study group was observed for serum iron concentration and serum iron levels (p=0.001).
A previous study reported that they did not find any differences with respect to iron parameters, even with H. pylori infection.21.23 Other previous work has found a relationship between H. pylori infection and declining levels of ferritin; for example, Parkinson et al24 has found a substantial correlation between low levels of serum ferritin and H. pylori infection. As far as we can tell, this is the first study to investigate the presence of a significant difference between males and postmenopausal females by studying the association between unexplained IDA and H. pylori infection.
Study limitations
Although this is an attempt to study H. pylori that might be of significance in progression of unexplained IDA, only a limited number of cases were investigated here. The present work was limited to patients from a single hospital at Al-Noor Hospital, Makkah, Saudi Arabia.This makes it impossible to deduce the findings to the whole of Saudi Arabia. Another drawback of our research is that we used a cross-sectional design, which might not be the optimal method for establishing a causal association between H. pylori infection and patient factors. The follow-up of such patients after eradication of H. pylori in the majority of our patients was lost, as many of these patients were referred to other hospitals, leading to a decrease in the evidence for a cause-and-effect association between H. pylori infection and “unexplained” IDA.
In conclusion, the GI tract assessment is a key step in the clinical assessment and treatment of IDA patients. A high percentage of patients are often left without a diagnosis. The current study proposes a relationship between H. pylori infection and unexplained IDA among Saudi population, with a considerable discrepancy between postmenopausal females and males. This study suggests that screening of H. pylori infection and appropriate treatment in any case of unexplained IDA, especially without clinical GI manifestations, will help to achieve a significant reduction in the overall disease burden.
Acknowledgment
The authors thank Afnan A. Al-Yamani, Malak H. Alfaifi, Shatha A. Haroun, Amjad Mashhour N. Altijani, and Alaa A. Abujbal for their efforts in collecting samples and recording data. We would like to thank MDPI editing company “https://www.mdpi.com/authors/english#English_Editing_Services” for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 15, 2021.
- Accepted April 18, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.




{kind=link}