


Abstract
The main objective was to determine the predictors of diastolic dysfunction in rheumatoid arthritis (RA). Articles pertaining to diastolic dysfunction in RA were retrieved from Scopus, EBSCO, PubMed, Web of Science, and Cochrane Library databases. Keywords such as: diastolic, cardiac, left ventricular function, heart failure, rheumatoid arthritis, and cardiac failure were used. Studies, which examined factors, or predictors of diastolic dysfunction in RA, and those with echocardiographic evaluation of diastolic dysfunction, were included. A total of 8 studies met the eligibility criteria. Most studies (6 out of 7 studies) demonstrated a significant inverse relationship between the E (early)/A (late) ratio and disease duration. The pooled analysis using the random effects model revealed a significant but weak inverse relationship between the ratio of the E to A ventricular filling velocities (E/A) ratio and the disease duration (p<0.05, r=-0.385). There was a significant relationship between E/A ratio and disease duration in RA.
Rheumatoid arthritis (RA) is the most common systemic autoimmune disease, which affects millions of individuals worldwide.1 Beyond destruction and deformities of the joints, there is increased morbidity and mortality in patients with RA.2,3 Cardiac failure is an independent risk factor for mortality in RA accounting for approximately one in 8 deaths.4 Left ventricular (LV) diastolic dysfunction encompasses mechanical and structural abnormalities such as hypertrophy or interstitial fibrosis, impaired myocyte relaxation resulting from ischemia, decreased distensibility, and abnormal diastolic filling of the left ventricle.5 Usually, diastolic dysfunction is an echocardiographic diagnosis based on transthoracic echocardiography, although cardiac MRI and radionuclide ventriculography were used during recent times to evaluate diastolic functions.6 Diastolic dysfunction may act as a precursor for overt cardiac failure. The prevalence of diastolic dysfunction in RA is approximately 37%.7 A recent meta-analysis concluded that patients with RA were more likely to have diastolic dysfunction, higher systolic pulmonary artery pressures, and larger left atrial size.8 The main purpose of the present systematic review was to evaluate the published literature in order to determine the predictors of diastolic dysfunction in RA.
Search strategy and study selection
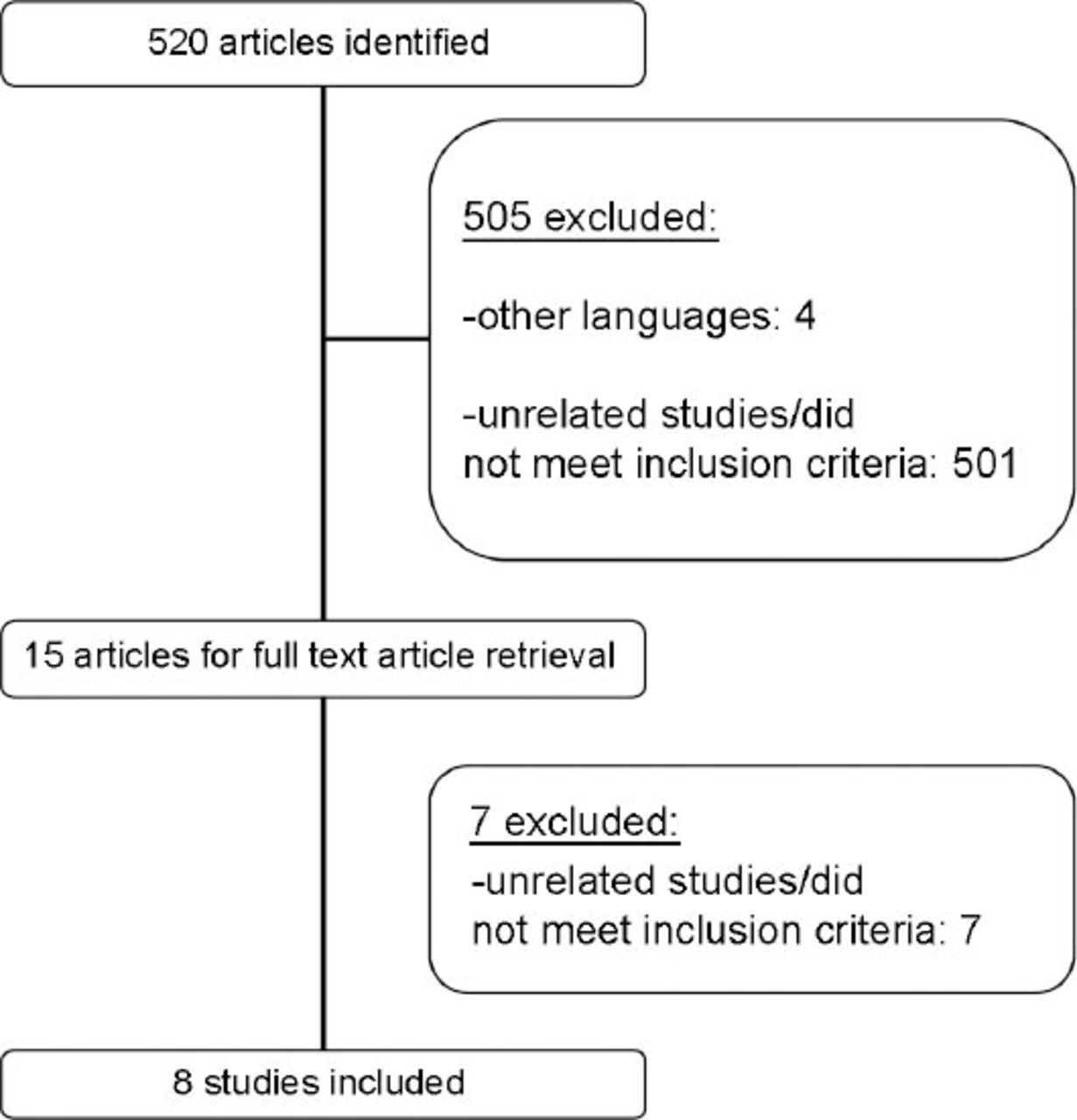
We retrieved all published studies on diastolic dysfunction in RA from Scopus, EBSCO, PubMed, Web of Science, and the Cochrane Library databases. Keywords such as: diastolic, cardiac, left ventricular function, heart failure, rheumatoid arthritis, and cardiac failure were used. The study was conducted between April and June 2014 at Medical Center, The National University of Malaysia, Cheras, Kuala Lumpur, Malaysia. We also scrutinised the bibliographies of all published articles to avoid missing any potentially relevant study. The abstracts of published studies were independently reviewed and assessed by both authors. Only those articles deemed appropriate and considered eligible by both authors, were included in this systematic review. Figure 1 summarizes the algorithm used for the selection of the studies. We used a stringent set of study criteria to ensure a high level of homogeneity across the selected studies. The inclusion criteria included: 1) Studies that examined factors or predictors of diastolic dysfunction in RA, 2) Studies with echocardiographic evaluation of diastolic dysfunction. We excluded studies written in other languages apart from English, articles such as: case reports, letters to the editor, supplements, and review articles. Studies with juvenile onset RA were also excluded.

The algorithm for selection of studies in this systematic review on predictors of diastolic dysfunction in rheumatoid arthritis.
Outcome measures
Numerous echocardiographic parameters were used in the studies namely E/A ratio (the ratio of the early (E) to late (A) ventricular filling velocities), left ventricular (LV) mass, left atrial volume index, LV end diastolic diameter, isovolumetric relaxation time (IVRT), early and late diastolic flow velocity. To date, there is a lack of a comprehensive consensus regarding diagnostic echocardiographic criteria for diastolic dysfunction. However, echocardiographic evaluation of diastolic function traditionally involves the measurements of transmitral flow parameters, including the E and A diastolic filling velocities, the E/A ratio, and the E deceleration time (DT) from an apical 4 chamber.9 The most common index of diastolic function used in these series of studies was E/A ratio. Hence, we focused on factors associated with this parameter. The following data were extracted from the selected studies: year of publication, study design, sample size, echocardiographic parameters: (E/A ratio, LV mass, early diastolic flow velocity, late diastolic flow velocity, IVRT), and associated clinical parameters (disease activity, disease duration, age, and so forth).10,11 The quantitative differences in the aforementioned parameter between the RA patients, and the controls were recorded. The data were pooled using a random effects model for a more conservative estimate of the correlation between the E/A ratio and clinical parameters. The advantage of this model is that it allows for heterogeneity across the studies.10 The results of the correlation analysis were expressed as a correlation coefficient (r) and p-value. Comprehensive Meta-analysis software version 2.0 (Biostat, Englewood, NJ, USA) was used to generate the Forest plot for the pooled data.
Study types and characteristics
A total of 8 studies met the eligibility criteria for this systematic review.12-19 Table 1 summarizes the selected studies. These studies were published between years 1999 and 2013. Half of the selected studies were conducted in Europe.14,16-18 Interestingly, all were case-control, cross-sectional, and observational studies. The controls were homogenous across the studies. Healthy subjects with unknown medical illness served as controls in all the studies. The sample sizes in this series of studies ranged from 65 to 1692 subjects.14,15 In most of the studies, the ‘cases’ were defined as patients with RA without any evidence of cardiovascular disease.
Summary of the selected studies on diastolic dysfunction in rheumatoid arthritis.
Disease duration
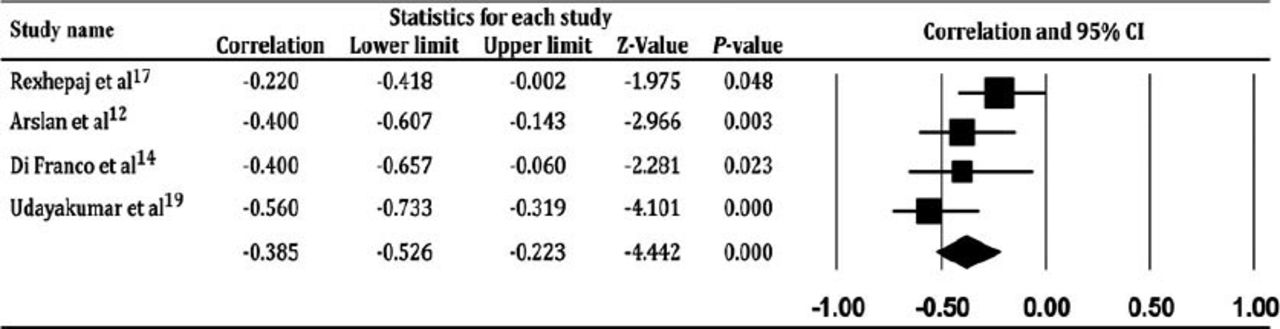
Seven out of 8 of the studies with a total of 2243 subjects investigated the correlation between diastolic dysfunction and the disease (RA) duration.12-17,19 Most of the studies (6 out of 7 studies) demonstrated a significant inverse relationship between the E/A ratio and the disease duration. The only exception was a study by Montecucco et al,16 which found no association between these 2 variables. We performed a pooled analysis using the data from 4 studies12,14,17,19 in order to determine the relationship between the E/A ratio and disease duration. Three of the studies13,15,16 were not included in the analysis as the values of the correlation coefficient (r) were not available. Our pooled analysis revealed a significant but weak inverse relationship between E/A ratio and disease duration (p<0.05, r=-0.385). Figure 2 illustrates the Forest plot on the correlation between E/A ratio and disease duration.
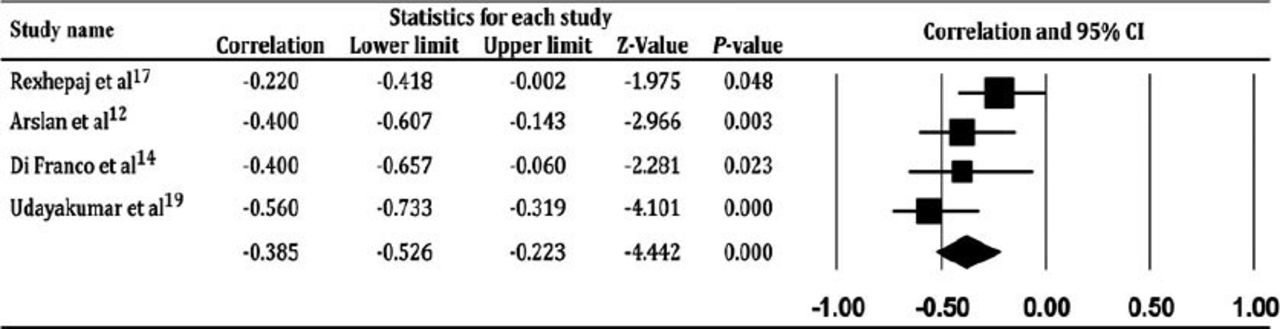
The Forest plot for the correlation between early to late ventricular filling velocity ratio and disease duration in rheumatoid arthritis.
Cytokines interleukin 6 and tumor necrosis factor-α (TNF-α)
Liang et al15 found that interleukin (IL) 6 levels were independently associated with diastolic dysfunction even after adjustment for cardiovascular risk factors (odds ratio [OR]:1.2, 95% confidence interval [CI]: 1.02-1.4). Tomas et al18 reported that TNF-α levels had a significant inverse relationship with E/A ratio. Unfortunately, our literature search failed to identify other studies examining the association between cytokines and diastolic dysfunction.
Demographic and clinical characteristics
Few of the selected studies investigated the association between diastolic dysfunction and the following demographic, and clinical characteristics namely age, disease activity, seropositivity, number of joints involved, Ritchie index, extra articular manifestations, and cumulative prednisolone doses.14,16,19 Apart from a single study16 showing a correlation between age and E/A ratio, none of the remaining studies observed any other risk factors for diastolic dysfunction in RA.
The findings of the present systematic review depict a significant inverse relationship between E/A ratio; an echocardiographic parameter of diastolic function, and duration of RA. Although the strength of the relationship was weak (r=-0.385), there was convincing evidence to support disease duration as a clinical predictor of diastolic dysfunction in RA. Although only 4 studies were included in the statistical analysis, it is noteworthy to mention that the remaining 2 out of 3 studies13,15 demonstrated a trend towards deterioration of diastolic function with disease duration. Liang et al,15 reported that the above association remained significant even after adjustment for traditional cardiovascular risk factors such as diabetes mellitus, smoking, and hypertension. The exact mechanism to explain this link still remains ill defined. However, researchers hypothesized that in RA there could be an ongoing subclinical myocardial inflammatory process, which leads to impairment of myocardial function.12,15
In RA, cytokines like IL6, IL1, IL17, IL23, and TNF-α are produced in abundance.11 Dinh et al20 reported that increased plasma levels of IL6 and TNF-α were associated with left ventricular diastolic dysfunction. It is tempting to speculate that a pro-inflammatory pathway may be one of the key orchestrators of diastolic dysfunction in RA. Keeping these findings in view, Liang et al15 and Tomas et al18 demonstrated a significant relationship between E/A ratio and IL6 and TNF-α levels. There is growing evidence suggesting that cytokines directly mediate hypertrophic remodeling and myocardial fibrosis through regulation of collagen synthesis and matrix metalloproteinase activity of the cardiac fibroblasts.21 Unfortunately, much of this evidence was derived from animal studies.22,23 Owing to the paucity of studies investigating the linking nexus between cytokines and diastolic dysfunction in RA, no firm conclusions could be made in this regard.
Montecucco et al16 reported that E/A ratio in RA correlated to the age of the patients. These findings were similar to many other population-based studies,24,25 which had proven the age-related deterioration in parameters of diastolic function. Most studies included in this review did not analyze the relationship between age and E/A ratio, probably due to the well-established influence of age on diastolic function, which requires no further verification. However, the inversion of the E/A ratio was observed at a younger age in the RA patients compared with the control, which lend credence to the notion of earlier deterioration of diastolic function in RA.16
There are a few limitations to this systematic review. Several factors may confound the reported findings in the selected studies. Observer bias should be considered as most studies did not specify if the echocardiography was blinded or not. The E/A ratio was by far the most frequently used echocardiographic parameter to assess diastolic function in the studies. Hence, we used this variable in our pooled analysis. In clinical practice, assessment of diastolic function is based on a combination of parameters such as IVRT, propagation velocity and intraventricular dispersion of E wave velocity. This limits the generalizability of our findings.
In conclusion, our systematic review indicates that there is concrete evidence supporting a significant relationship between E/A ratio and disease duration in RA. There are no robust data to suggest the role of other clinical or biochemical factors as predictors of diastolic dysfunction in RA.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. This systematic review was supported by the “Dana Lonjakan Penerbitan” research grant of The National University of Malaysia, Cheras, Kuala Lumpur, Malaysia.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.