


Abstract
Objectives: To determine the association between comorbidities and the severity of the disease among COVID-19 patients.
Methods: We searched the Cochrane, Medline, Trip, and EMBASE databases from 2019. The review included all available studies of COVID-19 patients published in the English language and studied the clinical characteristics, comorbidities, and disease outcomes from the beginning of the pandemic. Two authors extracted studies characteristics and the risk of bias. Odds ratio (OR) was used to analyze the data with 95% confidence interval (CI).
Results: The review included 1,885 COVID-19 patients from 7 observational studies with some degree of bias risk and substantial heterogeneity. A significant association was recorded between COVID-19 severity and the following variables: male (OR= 1.60, 95%CI= 1.05 - 2.43); current smoker (OR=2.06, 95%CI= 1.08 - 3.94); and the presence of comorbidities including hypertension (OR=2.05, 95%CI= 1.56 - 2.70), diabetes (OR=2.46, 95%CI= 1.53 - 3.96), coronary heart disease (OR=4.10, 95%CI= 2.36 - 7.12), chronic kidney disease (OR=4.06, 95%CI= 1.45 - 11.35), and cancer (OR=2.28, 95%CI= 1.08 - 4.81).
Conclusions: Comorbidities among COVID-19 patients may contribute to increasing their susceptibility to severe illness. The identification of these potential risk factors could help reduce mortality by identifying patients with poor prognosis at an early stage.
COVID-19 is a public health emergency as about 20 million laboratory-confirmed cases and about million deaths had been reported on August 2020.1-6 The disease covers wide clinical pictures including asymptomatic infection, mild upper respiratory tract illness, severe pneumonia, respiratory failure, and even death.7 Patients’ clinical manifestations include fever, non-productive cough, dyspnea, myalgia, fatigue, normal or decreased leukocyte counts, and radiographic evidence of pneumonia.8 However, as the pandemic continues, available data regarding the association between pre-existing comorbidities and the severity of COVID-19 illness is limited. Thus, investigation of the possible factors affecting the prognosis of patients with COVID-19 is needed to help clinicians identify highly susceptible individuals and those with poor prognosis at an early stage, in order to reduce mortality.
This review targeted to investigate the association between comorbidities and the severity of illness among COVID-19 patients.
Methods
The review included all the available studies, which investigated clinical characteristics, underlying comorbidities, and the severity of illness among COVID-19 patients from the beginning of the pandemic.
The inclusion criteria comprised hospitalized patients diagnosed with COVID-19 according to WHO guidance (severe acute respiratory syndrome-coronavirus 2 [SARS-CoV-2] detection in respiratory specimens by next-generation sequencing or real-time reverse transcription-polymerase chain reaction [RT-PCR] methods).9 The exclusion criteria comprised patients diagnosed with severe pneumonia without confirmation of COVID-19.
The outcome measure is the severity of COVID-19-related illness namely, intensive care unit (ICU) admission, mechanical ventilation and death. COVID-19 severity was defined based on the criteria of China’s National Health Commission as mild, moderate, severe, and critical.10
We searched Cochrane Library, EMBASE, TRIP, and MEDLINE databases. We also reviewed the primary references for additional studies. The following terms were used: Clinical features of COVID-19, OR Comorbidities associated with COVID-19 OR CORONA virus disease, OR NOVEL CORONA, OR Severe pneumonia, OR Patients infected with CORONA, and Outcome of COVID-19, OR adverse outcome, OR fatality of Covid-19, OR survivors and non-survivors of COVID-19, OR Intensive care unit for COVID-19.
Data collection and analysis
Two authors independently checked the titles and abstracts of potential articles for inclusion criteria. Then, they obtained and read all the relevant articles.
Data extraction and management
The following characteristics were extracted from the included studies11-17 (Table 1): study design, setting, duration, number and age of patients, and outcome measures including ICU admission, the need for mechanical ventilation and death. One author entered the data into the Review Manager (RevMan) 5.3.18
Characteristics of included studies.
Assessment of the risk of bias
The Newcastle-Ottawa Quality Assessment Scale for Case-Control/Cohort Studies was used to assess the risk of bias for the included studies.19 Each risk of bias was graded high, low, or unclear based on the following domains: i) adequate case definition (selection bias), ii) consecutive representativeness of cases (selection bias), iii) selection of community controls (selection bias), iv) Adequate control definition (selection bias), v) ascertainment of exposure/independent blind assessment of outcome (selection bias), vi) cases and controls comparability based on the design /independent blind assessment of outcome (comparability bias), vii) method for the ascertainment of cases and controls/Adequacy of the follow-up period (exposure/outcome bias), viii) all subjects complete follow up period/ Same response rate for both groups (exposure/outcome bias).
Assessment of the quality of evidence
The quality of evidence for each outcome measure was judged as high, moderate, low, or very low according to the GRADE approach (Grading of Recommendations Assessment, Development, and Evaluation).20
Measures of treatment effect
A random effect model of Review Manager 5.311 was used to analyze the data. Dichotomous variables were reported as odds ratios (ORs) with 95% confidence intervals (CIs).
I2 statistic was used to assess heterogeneity among the studies included in each analysis.21
Results
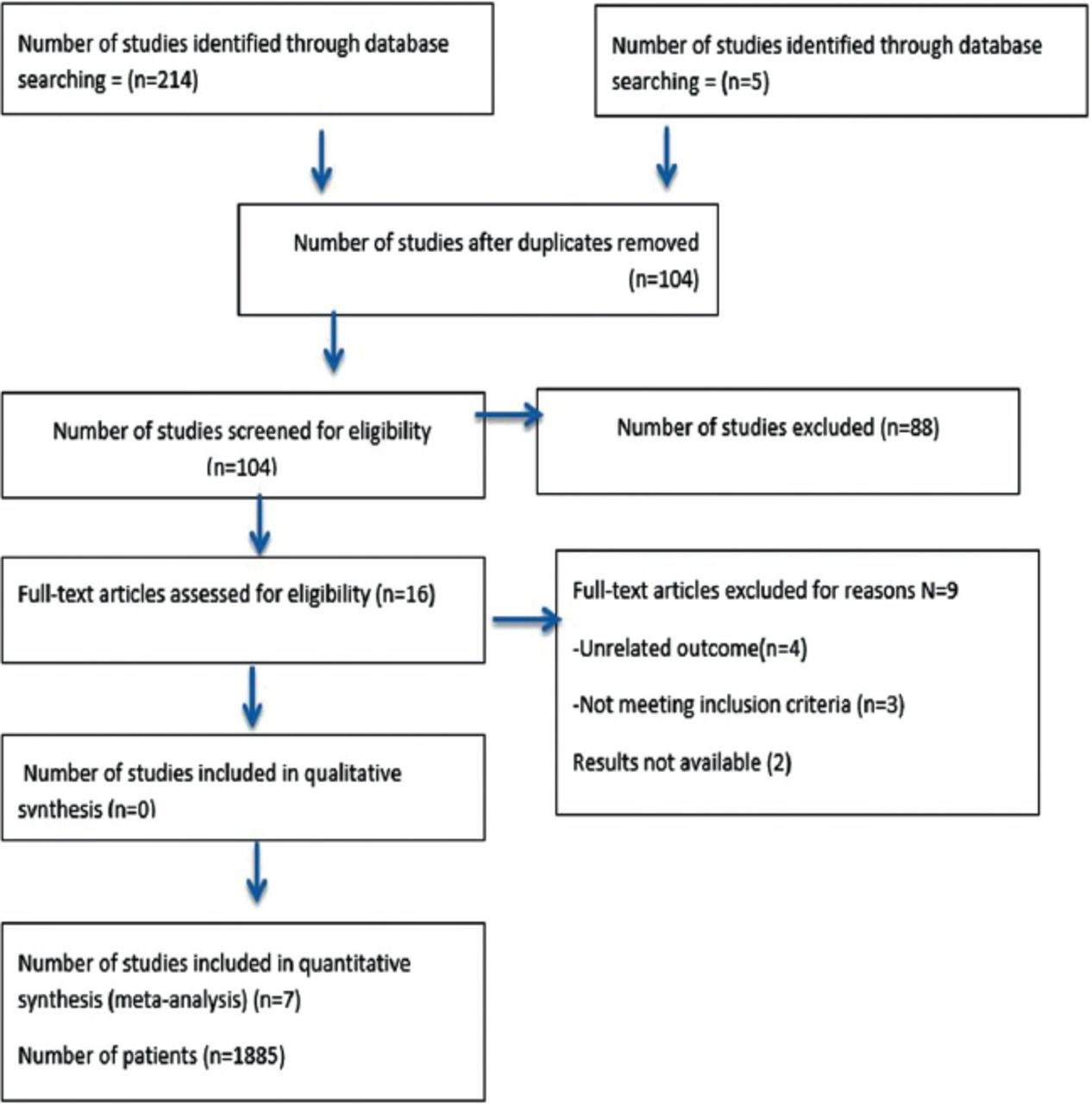
Out of 219 potentially relevant articles, 104 remained after removing duplicates. Sixteen full-text articles were assessed for eligibility; of these, 7 met the inclusion criteria. The Prisma flow diagram shows the details of the search method (Figure 1).

PRISMA flow diagram.
The review included 1,885 patients (810 females and 1,075 males) who were hospitalized and diagnosed with COVID-19. The median patient ages in years were reported as 56 (18-87) by Zhou et al,11 47.0 (35–58) by Guan et al,12 57 (25-87) by Zhang et al,15 and 56 (22-92) by Wang et al.16 Cao et al17 reported mean age of 50.1±16.3 years and Huang et al13 reported 49.0±41.58 years.
Risk of bias in the surveyed studies
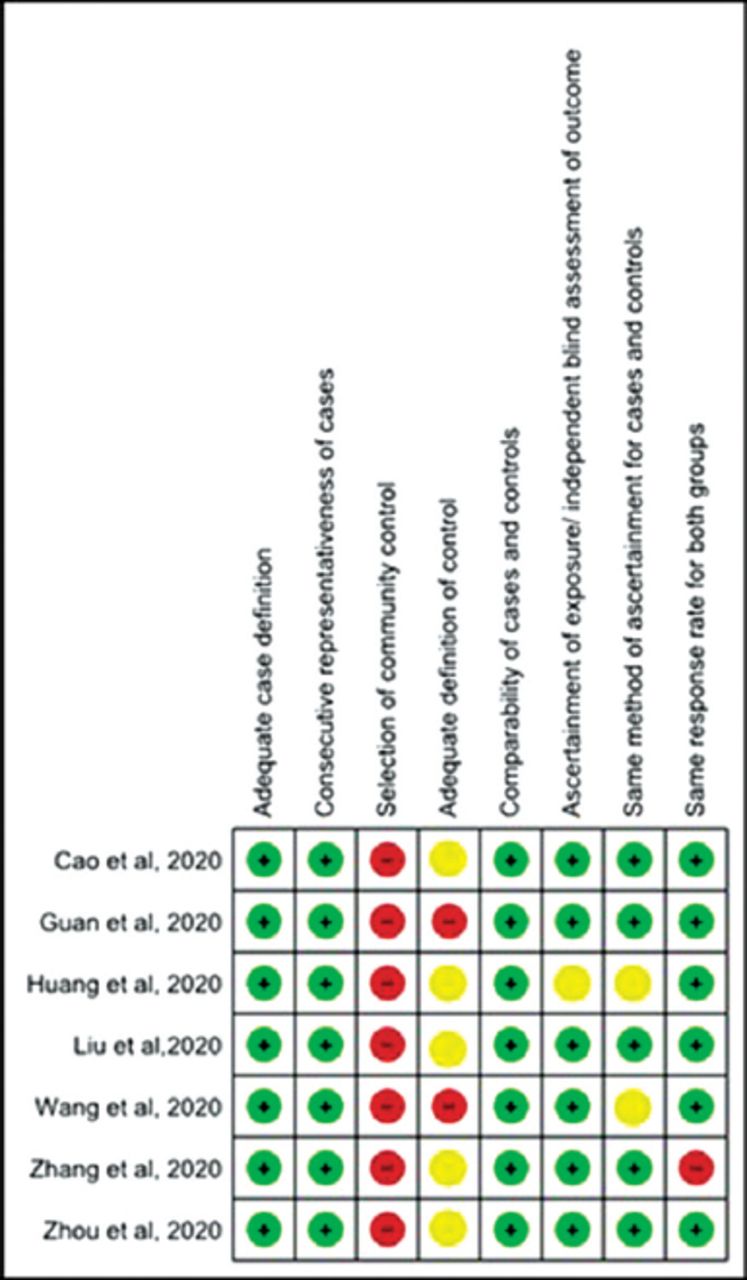
Overall, the included studies in this review had some risk of bias. All the studies recorded a high risk of bias in the selection of community controls. Regarding the adequate definition of controls, 5 studies,11,13-15,17 reported unclear bias while 2 studies12,16 reported high risk. Only the Zhang et al15 study had a high risk of bias for the same response rate for both groups (Figure 2).

Risk of bias among included trials.
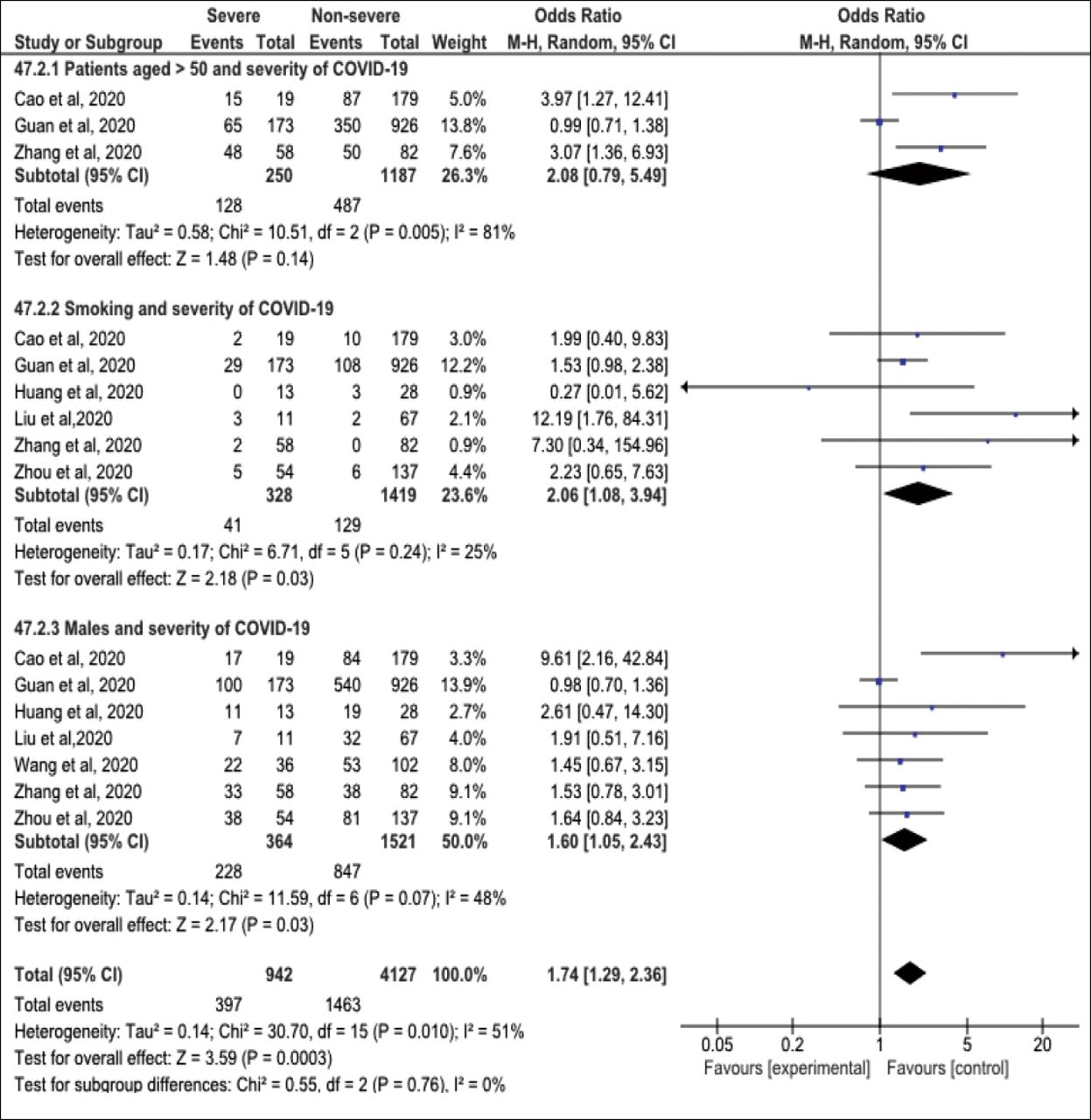
Figure 3 presents the association between background risk factors and the severity of COVID-19 illness. Male gender (OR=1.60, 95%CI=1.05-2.43) and smoking are significant risk factors for severe COVID-19 illness (OR=2.06, 95%CI=1.08-3.94). Low (I2=48%) and insignificant heterogeneity was reported in the analysis (I2=25% (p>0.05). On the other hand, no significant association was observed between patients aged >50 years and disease severity (OR=2.08, CI=0.79-5.49), with considerable significant heterogeneity (I2=81%, p<0.05).

Forest plot of background risk factors and severity of COVID-19 among studied participants.
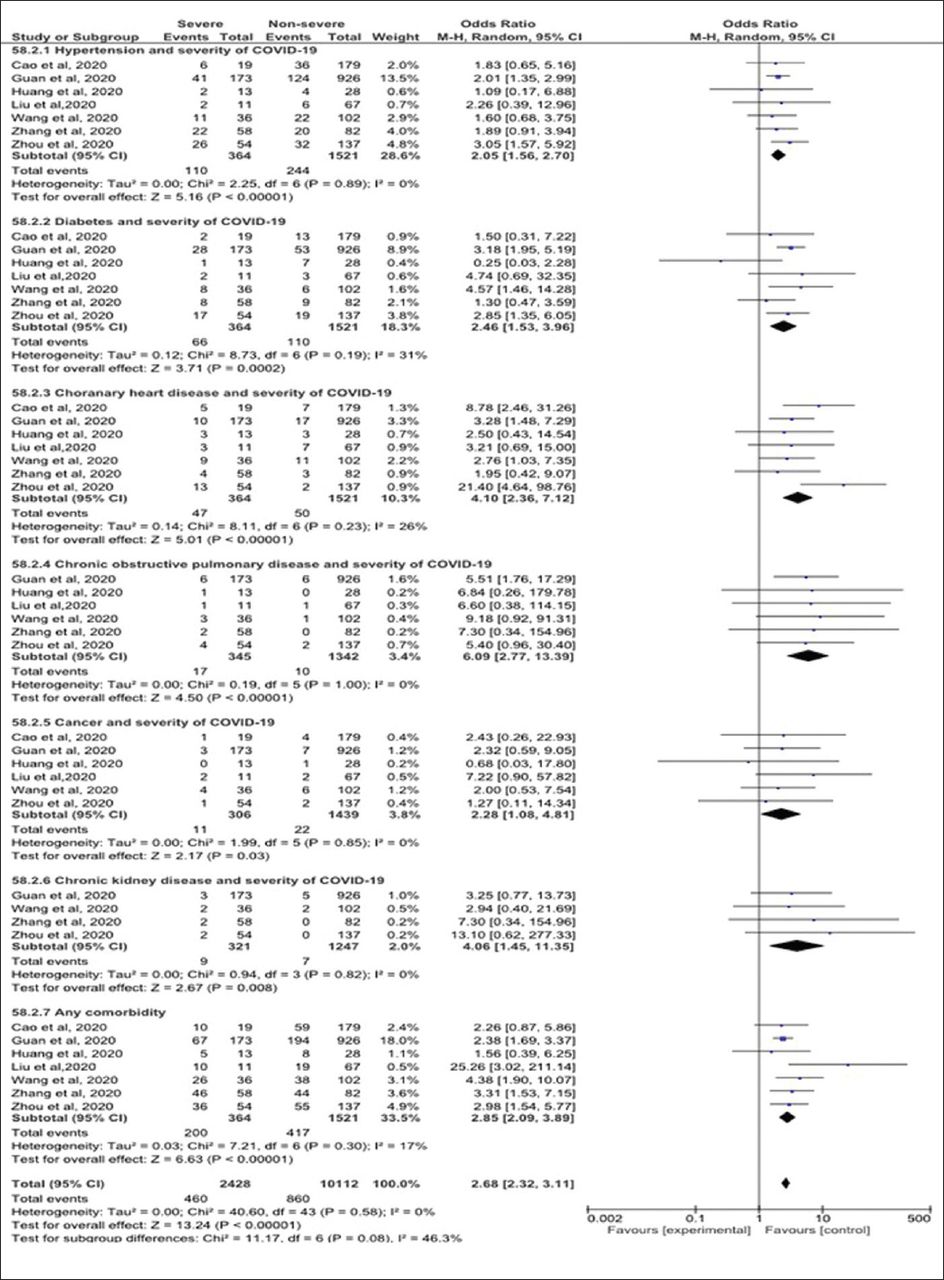
The association between comorbidities and COVID-19 severity is plotted in Figure 4. The risk for COVID-19 severity increased from two to four folds among patients with hypertension (OR=2.05, 95% CI=1.56 - 2.70), chronic kidney disease (CKD) (OR=4.06, 95%CI=1.45-11.35), chronic obstructive pulmonary disease (OR=6.09, 95%CI=2.77-13.3), and cancer (OR=2.28, 95%CI=1.08 - 4.81). No heterogeneity was detected between the surveyed studies (I2=0%). Also, a statistically significant association was detected between diabetic patients, Coronary Heart Disease (CHD) patients, and COVID-19 severity (OR=2.46, 95%CI=1.53-3.96, and OR=4.10, 95%CI=2.36-7.12, respectively). Moderate insignificant heterogeneity was detected in the analysis (I2=31%, p=0.19 and I2=26%, p>0.05).

Forest plot of underlying comorbidities and the severity of COVID-19.
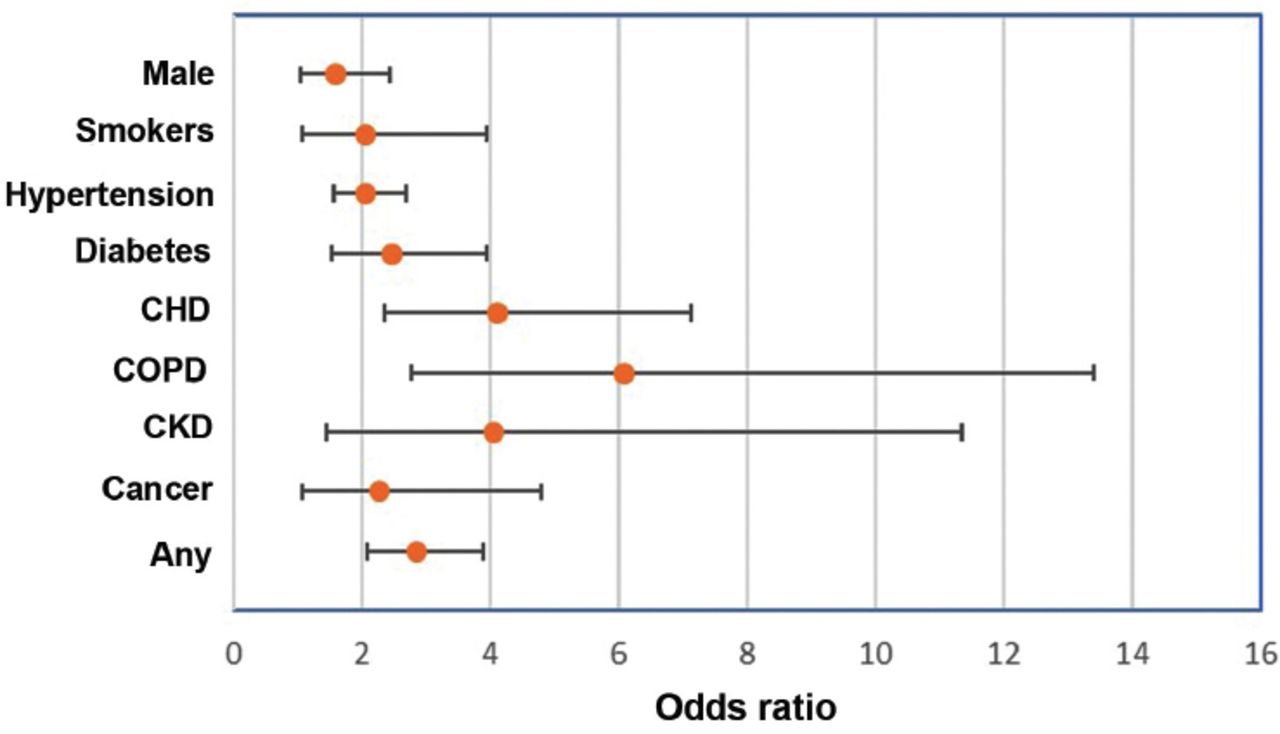
Figure 5 explains the forest plot of the pooled effects of the significant risk factors for the severity of illness among COVID-19 patients.
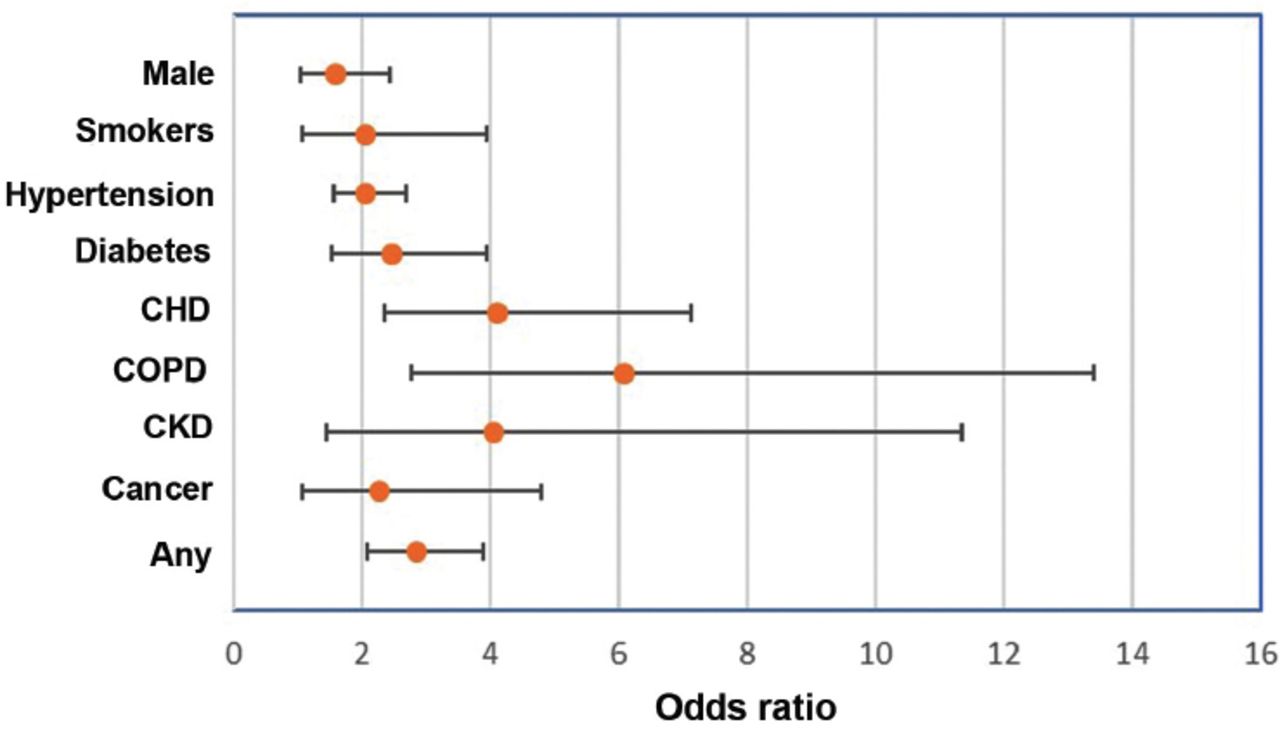
Odds ratio and confidence interval of the pooled effect of risk factors for the severity of COVID-19.
Quality of evidence
We judged the quality of evidence for each outcome measure based on the four domains recommended by the GRADE approach 13 for the evaluation of study limitations; namely, the risk of bias in each study, the directness of the evidence, consistency across studies, and precision of the pooled estimate. Overall, the surveyed studies were primarily observational with a considerable risk of bias, which resulted in downgrading the evidence by one level for all outcome measures. However, directness was not an issue, as all studies recorded the same outcome measures. Regarding the pooled estimate for the outcome measures (male gender, current smoking, any comorbidity, hypertension, diabetes, CHD, cancer), the quality of evidence was recorded as moderate. We downgraded the evidence by one level only due to the observational designs of the included studies. Imprecision, directness, and heterogeneity were not significant issues. Low and moderate heterogeneity (30-60%) was found between the outcome measures (I2=48% for the male gender, 25% for current smoking, 17% for any comorbidity, 0% for hypertension, 31% for diabetes, 26% CHD, and 0% for cancer. We judged the quality of evidence for the association between COPD and CKD was judged as low. We lowered the evidence by two levels because of the observational design and the degree of imprecision indicated by the wide confidence intervals due to the limited number of events included in the analysis. The heterogeneity between the surveyed studies could be due to differences in participants regarding geographical location, clinical features, method of diagnosis and duration of comorbidities, and treatment strategies (namely, dose, duration, route of administration, and follow-up).
Discussion
Summary of the evidence: This review investigated the relationship between comorbidities and the severity of illness among COVID-19 patients. We included 1,885 COVID-19 patients from seven studies. We found that male gender, smoking, and pre-existing comorbidities (including hypertension, diabetes, CHD, COPD, CKD, and cancer) were significant risk factors for disease progression.
Similarly, Huang et al13 and Chen et al7 reported that most COVID-19 infected patients were men (73% and 68% respectively), and a predominance of males was recorded by Li et al22 in their meta-analysis (60%, 95%CI=0.54, 0.65).
Liu et al14 found that old age was a risk factor for disease severity, which is inconsistent with our findings. Wang et al16 and Cao et al17 reported that ICU admitted patients had a higher median age than non-admitted (median age, 66 versus 51 years and 63.7± versus 48.6 ± 15.6 years) and were more likely to have underlying comorbidities (72% vs. 37%). In addition, Zhou et al11 found that the mortality rate was higher among older COVID-19 patients (OR 1.10, 95% CI 1.03, 1.17, per year increase; p=0.0043. However, in the present review, the pooled estimate of patients aged >50 years was not associated with disease severity. This discrepancy could be attributed to the older age group of the previous studies compared to our review.
The present review indicated that current smokers were twice as likely to have severe COVID-19-related illness as non-smokers (OR=2.06, 95%CI=1.08, 3.94). Our findings are consistent with those of Vardavas and Nikitara23 and Liu et al14 who investigated the pooled effect of smoking, and reported a significant association with the adverse outcome of COVID-19. Similarly, Wu et al24 and Guan et al12 reported that smokers were twice as likely as non-smokers to develop severe symptoms and higher mortality of the Middle East Respiratory Syndrome (MARS). The adverse effects of smoking on the immune system have been documented by previous studies.25-28
The present review demonstrated that the presence of comorbidities among COVID-19 patients, increases the severity of the disease by approximately 3-fold (OR=2.85, 95%CI=2.09, 3.89). This finding is consistent with the results of Liu et al,14 Zhang et al,15 and Guan et al12 who recorded comorbidities among severe cases of COVID-19 patients (25.6%, 79.3%, and 23.7%, respectively). Huang et al13 and Zhang et al15 recorded these comorbidities including mainly hypertension, diabetes, and CVD. Also, a higher fatality rate was recorded among the patients compared to those with non-underlying comorbidities.29 It is unclear whether hypertension is primarily a predictor of COVID-19 severity or a contributor to the deterioration of the disease.30 Our results showed that hypertension in COVID-19 patients was significantly associated with a 2-fold increase in the risk of disease severity (OR=2.05, 95%CI=1.56, 2.70, I2=0%). Similarly, a pooled analysis of hypertension in COVID-19 patients by Lippi et al31 showed that hypertensive patients were at a 2.5-fold risk of severe COVID-19 and mortality (OR: 2.49, 95%CI 1.98, 3.12, I2=24% and OR: 2.42, 95% CI 1.51-3.90, I2=0%). In contrast, Wan et al21 and Guan et al12 failed to find an association between hypertension and COVID-19 severity.
Cardiovascular disease is the most common underlying condition among COVID-19 patients, as reported by Zhang et al15 and Huang et al13 (OR=4.10, 95%CI=2.36-7.12). Our findings are consistent with those of Zheng et al33 and Cao et al,17 who reported increased risk for COVID-19 severity and mortality among CVD patients. The latter showed that CVDs were significantly more common in ICU COVID-19 cases compared to non-ICU cases (26.3% versus 3.9%, p<0.01). Likewise, COVID-19 diabetic patients recorded higher disease severity and mortality than non-diabetic ones.34-37 The same was documented by the current review (OR=2.46, 95%CI=1.53-3.96). The adverse outcome of COVID-19 among diabetic patients could be attributed to many factors, which include comorbidities such as hypertension and cardiovascular disease, obesity, a pro-inflammatory, glucose-lowering agents, and anti-viral treatments.38 The immune system of diabetic patients is compromised, making it harder to fight the virus and elongating the recovery period. Also, the environment with elevated blood sugar may aid the survival of the virus.37
Regarding COPD, earlier studies reported no significant increased risk for COVID-19 among COPD patients.12,39,40 A more recent study found a significant association and over a 5-fold increase in the risk of severe COVID-19 infection in COPD patients.41 Zhao et al42 recorded the pooled OR to be 4.38 (95% CI: 2.34-8.20). Nearly the same risk was observed in our review (OR=6.09, 95%CI=2.77-13.39, p<0.05). The predisposition of COPD patients to severe COVID-19 could beexplained by the increased levels of Angiotensin-Converting Enzyme 2 (ACE2) in these patients, by which SAR-COV-2 enters human cells and causes COVID-19.43,44
Consistent with our findings, a study assessed the association of COVID-19 and chronic kidney disease in over 700 patients and a higher percentage for acute kidney injury (AKI) and mortality was reported.45 Similarly, Lippi and Henry41 found a significant association between CKD and severe COVID-19 illness (OR=3.03 (95%CI=1.09-8.47). People with CKD and other severe chronic medical conditions tend to have weaker immune systems and are at a higher risk for more severe COVID-19 illness. Moreover, the anti-rejection medication given to patients with kidney transplantation suppresses their immune system, which can make it harder for the body to fight infections.46
In general, patients with cancer are more vulnerable to infection. A recent nationwide analysis in China47 reported increased risks of adverse outcomes in COVID-19 cancer patients, which is consistent with this review (OR=2.28, 95%CI=1.08-4.81). Several strategies have been proposed to offset the risks, such as delaying of required chemotherapy or surgery, and the immunocompromised status.48
Study limitations
The results of this review should be interpreted with caution as the evidence is derived from observational studies that have some risk of bias and substantial heterogeneity.
In conclusion, male gender, smoking, and underlying comorbidities were found to be significantly associated with COVID-19 severity. These pre-existing conditions could increase the susceptibility of such individuals to COVID-19. Recognizing these risk factors could help clinicians reduce mortality by identifying patients with poor prognosis at an early stage.
A systematic review of clinical trials with a lower risk of bias and limited heterogeneity is recommended to support the association of comorbidities and COVID-19 severity.
Acknowledgment
We would like to thank Editage (www.editage.com) for English language editing. “Also, we would like to thank Miss Mona Ahmed Almusawi for the Arabic translation of the abstract.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any entity.
- Received July 15, 2020.
- Accepted September 28, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Integration of functional capacity to medically necessary, time-sensitive scoring system: A prospective observational study
- Risk factors for severe COVID-19 among patients with systemic lupus erythematosus: a real-world analysis of a large representative US administrative claims database, 2020-2021
- General practice attendances among patients attending a post-COVID-19 clinic: a pilot study