


Abstract
Objectives: To determine the frequency and distribution of mumps-specific IgG antibodies among the healthy adult Saudi population in Al Madinah Al Munawarah, Saudi Arabia, where mandatory vaccination against measles-mumps-rubella (MMR) has been implemented for 30 years.
Methods: Qualitative and quantitative indirect enzyme-linked immunosorbent assay was performed to determine the mumps IgG antibody levels in sera collected from 429 individuals, including 224 men and 205 women. Participants were stratified into 3 age groups according to vaccination history (<20, 21-30, and >31 years).
Results: The overall seroprevalence of mumps antibodies in our population was 79.0%. The highest proportion of individuals with IgG antibody seropositivity, at 87.8% (95% confidence interval (95% CI): 84.7%-90.8%), was observed among the <20 years age group, who received 2 doses of vaccine. No significant relationships were observed between mumps seropositivity and age group or gender. The multivariable analysis identified the male gender and the age group >31 years as factors associated with an increased likelihood of seronegativity. Al Madinah Al Munawarah has achieved increased anti-mumps antibody seroprevalence since the implementation of the 2-dose MMR vaccination schedule.
Conclusions: Based on our study findings, we recommend that serological screening be performed to assess the need for mumps vaccination among adults at high risk for exposure and transmission.
Mumps is an acute viral illness caused by the mumps virus, a single-stranded, enveloped, RNA virus in the Paramyxoviridae family.1 Mumps is endemic worldwide, and disease outbreaks emerge in unvaccinated areas approximately every 5 years. The mumps virus is highly contagious and spreads through direct contact with respiratory droplets or saliva produced by an infected individual.2 The clinical presentation of mumps is vary from asymptomatic or non-specific symptoms to complications that include hearing loss, orchitis, mastitis, oophoritis, encephalitis, pancreatitis, and meningitis. Incidents of nephritis, myocarditis, and other associated symptoms have also been reported in mumps patients. The rate of complications is higher among patients older than 15 years.1,3 Because mumps in older patients is associated with the potential for sterility, mumps outbreaks continue to represent a clinical concern.4 Immunization is the optimal strategy for evading this viral illness, and treatment has remained conservative. Unvaccinated postpubertal males who are diagnosed with mumps virus commonly present with complications such as mumps orchitis.5-7 In general, natural viral infection provides lifetime protection against the virus for most individuals; however, repeated mumps attacks have been reported.8 Immunity against mumps is associated with the presence of specific anti-mumps IgG antibodies in serum. Whether lifelong immunity is associated with an enhanced immune response to the circulation of wild viruses among the population remains unclear.9 A previous study examining 45 naturally infected individuals reported that 91% demonstrated persistent, long-lived antibody responses that lasted for up to 26 years.10
In modern countries, infant vaccination programs, the size to maintain high levels of vaccination coverage for measles and rubella vaccinations, and the goal of reducing the incidence of mumps, routine mumps vaccination is recommended.9 Two doses of the measles-mumps-rubella (MMR) vaccine can provide long-lasting antibodies against mumps. Between 74% and 92% of individuals had detectable anti-mumps antibodies, as detected by enzyme-linked immunosorbent assay (ELISA), up to 20 years after the second dose of the MMR vaccine was administered.1,11 However, evidence of mumps outbreaks among individuals who have received 2 doses of the MMR vaccine has challenged the effectiveness of the vaccine, despite the perception that compliance with the vaccine schedule would confer lifelong immunity against the mumps virus.12
Outbreaks of mumps cases in vaccinated populations have recently occurred in many countries, suggesting the potential waning of vaccine-induced immunity.13-20 Cases of mumps re-infection during recent outbreaks among previously vaccinated individuals have been reported, including those who received 2 doses of the vaccine.13 Because of waning immunity over time, the recurrence of mumps outbreaks may be associated with secondary vaccine failure.21 Many of the people associated with new mumps outbreaks received their second vaccine dose at least 10 years prior to the outbreak, suggesting that secondary vaccine failure may be a potential cause for the recurrence of mumps and may indicate that individuals require re-immunization to achieve an adequate immune response to defend against infection.22
Saudi Arabia has made huge advances in its childhood immunization program since the first uniform expanded immunization program (EPI) was implemented in 1991. The mumps vaccine is typically administered as a component of the MMR vaccine. The vaccination schedule has been modified several times with the goal of maintaining high levels of immunity and coverage.23-25 Despite the recent global resurgence of mumps cases, including among highly vaccinated populations, relatively limited attention has been paid to mumps research in Saudi Arabia. Very limited data are available from studies examining the virological, clinical, and seroepidemiological status of mumps in Saudi Arabia.
The aim of this study was to evaluate the humoral immunological memory of IgG antibodies against mumps among the healthy adult population in Al Madinah Al Munawarah, Saudi Arabia, where mandatory vaccination for MMR has been performed since 1991.
Methods
A cross-sectional study was performed from August 2019 to August 2020. A total of 429 serum samples from healthy Saudi individuals were collected at University Health Care Center in Al Madinah Al Munawarah, Saudi Arabia, which were stratified into 3 age groups based on the history of MMR vaccination in Saudi Arabia, as follows. 1) Persons born before 1991 (before mandatory MMR vaccination); 2) persons born between 1991 and 2000 (who received one dose of the MMR vaccine); and 3) persons born after 2001 (who received 2 doses of the MMR vaccine).
The subjects were included in the current study based on walk-in clinic to the primary health care center and agreement to participation and have been randomly chosen. Thereafter, the sample size was adjusted upon inclusion and exclusion criteria during the study conduction time.
All Saudi adults’ healthy individuals were welcomed and included at the time of conducting in the study. Participants with a history of recent infection or MMR vaccination were excluded.
This study was approved by the Research Ethical Committee of Taibah University (IRB No.2020/65/112/MLT) and was conducted in obedience with regulations and official policies and the creeds of the Helsinki Declaration.
Laboratory methods
Blood samples were collected and stored in 5-ml vacutainer serum tubes after informed consent was obtained from each individual. Blood samples were immediately transported to the research laboratory of the College of Applied Medical Sciences, Taibah University, for further analysis. Samples were centrifuged for 15 minutes at 1500g within one hour of collection. Sera were then quickly transferred to plastic vials and preserved at -20°C until use.
Qualitative and quantitative indirect enzyme-linked immunosorbent assays (ELISAs) were performed concurrently for the determination of mumps IgG antibodies using commercial Human ELISA Kits (Human, Wiesbaden, Germany), according to the manufacturer’s guidelines. As quality control procedures, blanks and negative and positive controls were included on each plate. A semi-automated ELISA washer and reader (Biotek, Winooski, US) was used for all washing steps, according to the product’s user manual. The assay specificity and sensitivity was 95% and 99%, respectively according to the manufacturer.
Initially, serum samples were diluted 1:100 with dilution buffer and were properly mixed. The cut-off values for anti-mumps IgG antibodies were calculated, then the results were determined qualitatively as positive, negative, or equivocal. According to the manufacturer’s instructions, samples with optical density values above or equal to the cut-off value + 15% were considered positive, values below the cut-off value − 15% were considered negative, and values within 15% above or below the cut-off value were considered equivocal. The IgG antibody concentration values were estimated from the measured optical density values by means of an equation and are expressed in human units per millilitre (AU/ml).
Statistical analysis
Data were analyzed using the Statistical Package for Social Sciences version 25 (IBM SPSS Statistics, Armonk, NY, USA) with a significance level set at p≤0.05, and 95% confidence intervals (CIs) were obtained. Study participants were divided into 3 age groups (younger than 20 years, 21-30 years, and older than 31 years). Qualitative variables were described using frequency and percentage. Quantitative variables were described using descriptive statistics, and the mean ± standard deviation (SD) were calculated. Chi-square analysis was used to test independence among qualitative variables. The Mann-Whitney U test was used to detect significant differences between 2 independent groups, whereas the Kruskal-Wallis test was used to assess significant differences in non-normally distributed quantitative variables between more than 2 groups. Correlations between age and IgG antibody concentrations were analyzed using Pearson’s correlation coefficient and scatter plots. To examine the effects of age group and gender on mumps serostatus, logistic regression analysis was performed.
Results
In this study, 429 healthy Saudi individuals were recruited, which included 224 (52.2%) men and 205 (47.8%) women. The mean age of all study participants was 31.9 ± 9.8 years and ranged from 18 to 66 years. Men were slightly older, with a mean age of 32.4 ± 10.3 years, compared with a mean age of 29.5 ± 6.5 years for women. Based on changes in the mumps vaccination policies in Saudi Arabia, the participants were divided into 3 age groups: <20 years (n=41, 9.6%), 21-30 years (n=171, 39.9%), and >31 years (n=217, 50.6%) (Table 1).
- Demographic characteristics of the study participants (N=429) and their vaccination status.
Distribution of anti-mumps IgG antibodies among age groups and gender
The analysis showed that significantly more individuals were categorized as anti-mumps antibody seropositive (79%, n=339, p<0.001) compared with those categorized as seronegative (13.1%, n=56) and equivocal (7.9%, n=34).
The distribution of mumps IgG antibody seropositive individuals in every age group is shown in Table 2. The highest proportion of IgG antibody seropositive individuals, 87.8%, was observed among the 2-dose vaccinated age group (<20 years; 95% CI: 84.7%-90.8%). Among participants in the 21-30 years age group, who received one dose of the MMR vaccine, 78.4% (95% CI: 74.5%-82.3%) were seropositive. In the age group older than 31 years, 77.9% (95% CI: 74.0%-81.8%) were seropositive for the anti-mumps IgG antibody. No significant association was perceived between age group and mumps seropositivity (p=0.247).
- Distribution of serological status for mumps IgG antibodies by age (N=429).
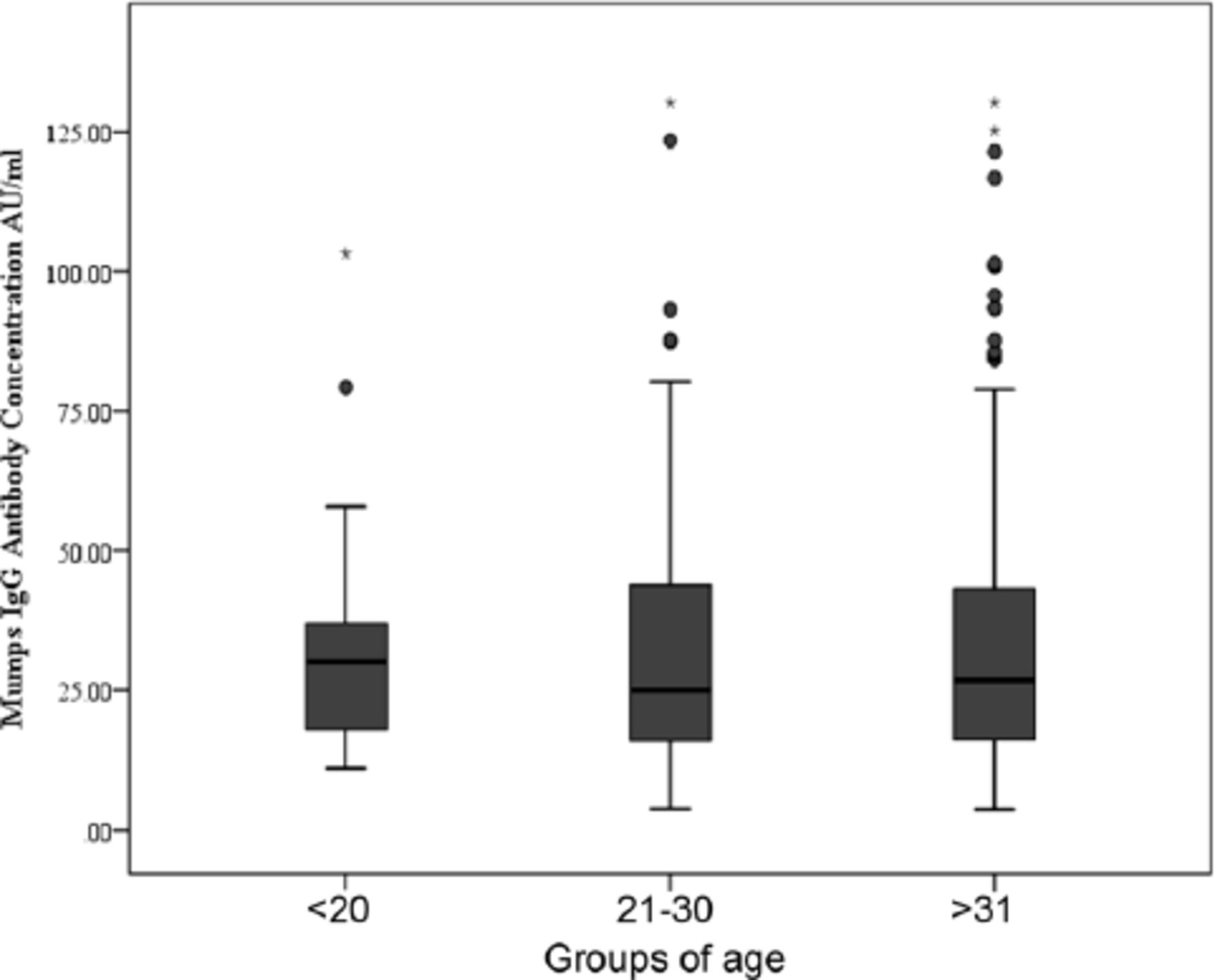
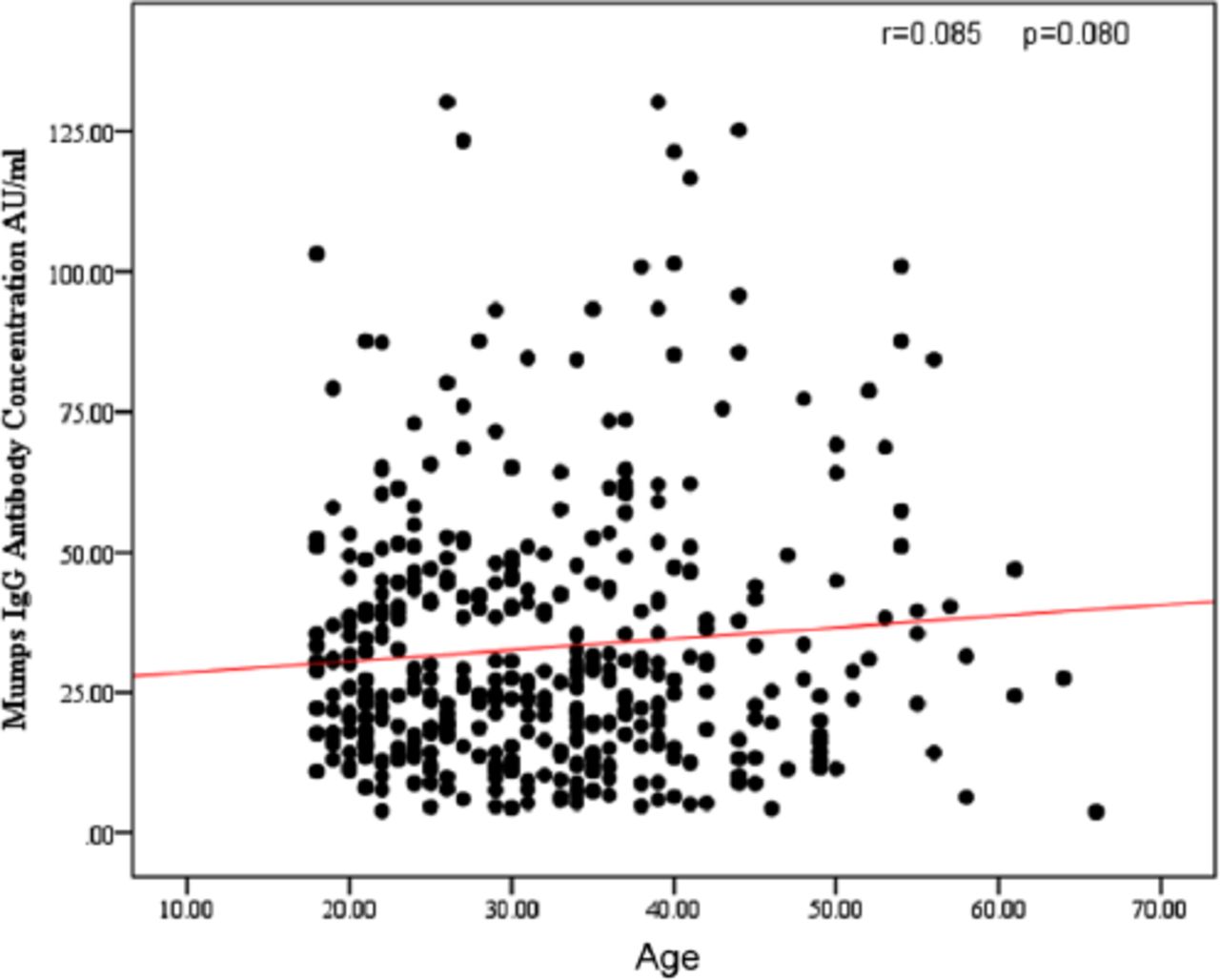
The anti-mumps IgG antibody levels were also quantitatively evaluated, and the anti-mumps IgG antibody concentrations were compared across age groups (Figure 1). The median anti-mumps IgG antibody concentration in the 2-dose vaccination age group (<20 years) was 30.08 AU/ml, which was higher than those in the 21-30 years (24.96 AU/ml) and >31 years (26.91 AU/ml) groups. However, no significant difference was determined across age groups (p=0.921). Furthermore, we identified a non-significant correlation between age and anti-mumps IgG antibody concentrations using the Pearson correlation coefficient (r=0.085, p=0.080, Figure 2). Analysis of anti-mumps IgG antibody and gender shows the distribution of mumps serological status according to gender. Among men, 77.1% (95% CI: 73.2%-81%) were seropositive for anti-mumps IgG specific antibodies, whereas 85.2% (95% CI: 81.9%-88.5%) of women were found to be seropositive for antibodies against the virus. No significant difference was observed between gender (p=0.270).

- Concentrations of anti-mumps IgG antibodies among the 3 age groups. The median for each age group is shown by the horizontal line inside the box, which represents the 50% percentile. The 25% and 75% percentiles are indicated by the lower and the upper ends of each box, respectively. The distance between the 2 percentiles represents the interquartile range (IQR), which reflects the distribution of the values. The ends of the whiskers represent one and a half times the IQR. Extreme values that occur outside of the box and whiskers are considered outliers. Age group frequencies: <20 years (n=41), 21-30 years (n=171), and >31 years (n=217).

- Scatterplot showing age and anti-mumps IgG antibody concentrations.
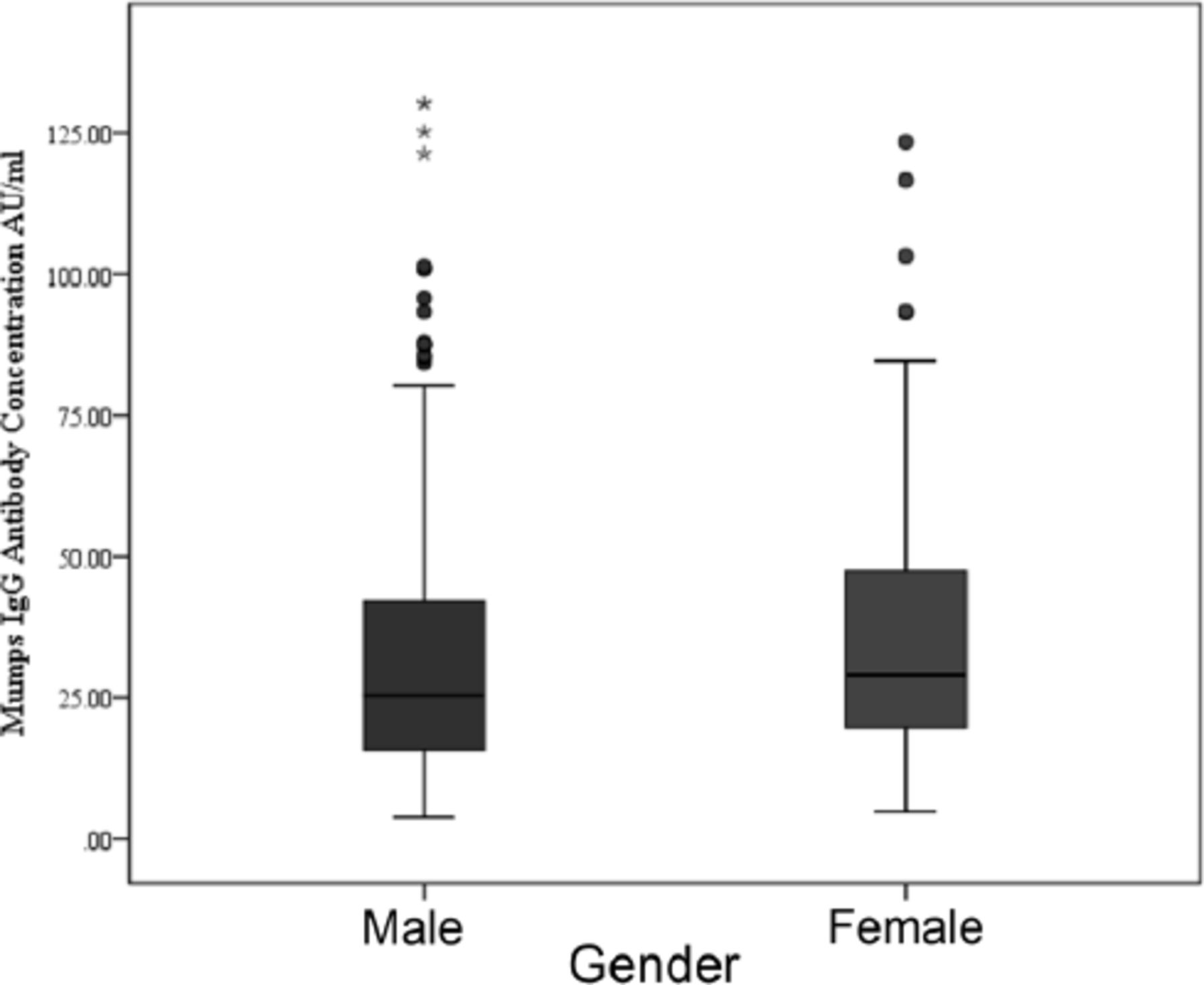
The quantitative measurements (min, median, and max) of anti-mumps IgG concentrations among women were higher than those among men (28.95 vs. 25.41 AU/ml, p=0.056). In addition, the median anti-mumps IgG concentration was higher in women than men in all 3 age groups (Figure 3).

- Box plot showing differences in the concentrations of anti-mumps IgG antibodies between men and women. Whiskers and box bands represent quartiles. Extreme values that occur outside of the box and whiskers are considered outliers. Gender frequency: men (n=224) and women (n=205).
Effects of age group and gender on mumps serostatus
Seropositive status was set as the reference category, men were compared to women, and age groups were compared against the greater than 31 years group. Compared with individuals in the age group older than 31 years, individuals in the age group younger than 20 years had lower odds of being seronegative (OR=0.276; 95% CI: 0.063-1.202, p=0.086). Similarly, individuals in the age group 21-30 years had lower odds of being seronegative than those in the age group older than 31 years, with an OR of 0.742. A higher risk of being seronegative was observed for men compared with women (OR=1.629; 95% CI: 0.705-3.764). The model also showed that men had a higher probability of being equivocal than women (OR=1.745; 95% CI: 0.594-5.130) and that the age group 21-30 years had a higher probability of being equivocal than the age group older than 31 years (OR = 1.531; 95% CI: 0.729–3.219).
Discussion
Mumps is a vaccine-preventable viral infection.12 Although the clinical picture of mumps is generally mild, mumps can cause serious complications, particularly among older patients.26,27 Long-term outcomes can include paralysis, deafness, seizures, hydrocephalus, and cranial nerve palsies.28 Because this disease is rarely fatal, it has been somewhat overlooked related with further infectious diseases, such as measles. However, in recent years, several mumps outbreaks have occurred in many countries, including those with long-established vaccination programs. These mumps outbreaks represent large resource burdens for the departments of public health. Consequently, mumps disease continues to represent a global public health issue. Unpredictably, a decade ago in the USA, several mumps outbreaks have been described in close contact, high-density locations, such as academies, with an extraordinarily high rate among immunized young adults.29 Outbreaks have also commonly been reported at colleges and in close-knit societies, and these have generally been reported in vaccinated individuals. Similar incidences have also been recounted in the Netherlands, Canada and other countries.30 In recent years, a growing number of mumps cases have been stated in Saudi Arabia, a substantial number of which have been reported among the adult population, many of whom have received 2 doses of the MMR vaccine. Herd immunity against mumps must be continued above 75%-86% to fall disease incidence and protect from disease transmission among the population.31 Recently, the World Health Organization (WHO) recommended >95% MMR vaccine coverage to achieve herd immunity.12 However, a Spanish study suggested that the herd immunity threshold was 84%-90% in terms of serious commonness of positive results on the basis of serological assessment.32 Starting in 1991, the administration of a single dose of the MMR vaccination became mandatory for all children in Saudi Arabia. Consequently, vaccination coverage in this country increased to more than 90%. Vaccination with 2 recommended doses of the MMR vaccine was implemented in 2001, and the number of mumps cases began to gradually decline until 2009 when the numbers began to rise again.33 This increase in cases prompted health authorities to implement a large vaccination campaign in 2011 and 2013.34,35 In 2013, a significant increase in mumps cases was reported, but the number of cases decreased in the following 2 years.33
In mumps serostatus studies using ELISA to compare antibody titre levels 6 months and one year after vaccination, antibody titre levels decreased by approximately 70% after 8 years and by 75% or more after 15-20 years following the second dose.11,36 In another study, people who were vaccinated with their second dose more than 8 years ago were 76% more likely to be seronegative than those who were vaccinated with the second dose less than 2 years earlier.37
Our results showed that the overall seroprevalence of mumps antibodies was low (79%), much lower than the 90% required to protect from disease.18 No mumps IgG antibodies could be detected in 11.7% and 15.7% of individuals in the 21-30 years and over 31 years age groups, respectively. This low level of immunity to mumps may explain the appearance of sporadic, small disease outbreaks during recent years. These findings may indicate the loss of immunity due to waning antibody levels over time, even after 2 doses of the MMR vaccine, due to reduced immunogenicity induced by the mumps vaccine component of the MMR in the absence of natural boosting.11,38,39 These data could also be interpreted as insufficient vaccination coverage, which may result in an epidemiological move of disease frequency to older age groups, increasing the rates of severe disease and problems.38 However, this finding could also be associated with the low sensitivity of the ELISA assay that was used to assess the antibody titre.40 The highest proportion of individuals with seropositivity against IgG antibodies was 87.8%, which was observed in the twice-vaccinated age group (<20 years). This result was expected, and previous studies have indicated the importance of the 2-dose mumps vaccine regimen for the prevention of clinical mumps, with an efficacy of approximately 88%.41,42 These data, therefore, provide a good indication that the currently established vaccination regimen is effective for the prevention of potential mumps outbreaks in the future. Nevertheless, our data also indicated that older individuals might be susceptible to mumps virus infection. Serological screening to determine the necessity of mumps immunization should be conducted to decrease the rates of serious disease and complications among high-risk adults.
Consistent with reports by other researchers, our data showed no significant change in the mumps seropositivity rate among men and women.38,43,44 Similar to several previous studies; however, a higher mumps seronegativity rate was reported among men than among women.20,38 Interestingly, we showed in a previous study, a significant association between age as well as measles seropositivity.45
Our results showed that the median anti-mumps IgG concentration was higher in women than in men for all age groups. Unfortunately, these differences did not reach the threshold for significance. Our results agree with those reported by other studies, which showed a similar trend.44,46
Our results showed that male gender and age >31 years were associated with an increased risk of being seronegative for anti-mumps antibodies, which agrees with previous studies that reported a significant male gender bias and an enlarged incidence among the older age group (>30 years old).44,47
Study limitations
Small sample size and vaccination history of the participants. Additionally, lack of samples from different cities in Saudi Arabia to get a conclusive figure about the seroprevalence of anti-mumps IgG antibody in country.
In conclusion, the immunity levels against mumps in Al Madinah Al Munawarah population is likely sufficient to prevent large outbreaks. The current vaccination regimen appears to be efficient; however, to prevent all outbreaks and adequately control mumps, extensive 2-dose vaccination coverage is likely necessary to maintain seroprevalence levels above the herd immunity threshold for the entire population, and serological screening may be necessary to assess the needs for supplemental mumps vaccination among adults at high-risk for coverage and transmission.
Acknowledgment
We would like to thank Cambridge Proofreading Worldwide LLC (https://proofreading.org/) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 21, 2021.
- Accepted June 27, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.