


Abstract
Eosinophilic esophagitis (EoE) is an atopic disease in which eosinophils infiltrate the esophageal mucosa and may result in a variety of upper gastrointestinal symptoms. Chief among these are dysphagia, heartburn, and food bolus obstruction in adults whereas children often present with abdominal pain or vomiting. Eosinophilic esophagitis is a chronic condition that if not detected and left untreated could lead to the development of subepithelial fibrosis and esophageal stenosis. The diagnosis of EoE is confirmed in a patient presenting with characteristic EoE symptoms, classic signs on endoscopy, and biopsy results showing >15 eosinophils/hpf. A number of useful treatments against EoE are currently available with new therapeutics on the horizon. The former include PPIs, topical steroids, and elimination diet; the latter comprise novel biologics including the monoclonal antibody dupilumab. All these treatments can improve symptoms and reduce esophageal eosinophil count. This brief introductory review describes the detection, diagnosis, and management of EoE.
The chronic clinical entity known as eosinophilic esophagitis (EoE) was first described as a T-helper type 2 (Th2) inflammatory cell-mediated disease and leading cause of solid food dysphagia, chiefly encountered in children but also in adults, by Landres and colleagues in the late 1970s.1,2 Eosinophilic esophagitis has only relatively recently emerged as a distinct disorder in adults,3 but is now widely accepted as a major cause of upper gastrointestinal morbidity worldwide.4
Eosinophilic esophagitis consists of isolated esophageal eosinophilia (peak value >15 eosinophils/high-power field; hpf) in patients with immune- or antigen-mediated dysphagia that may or may not be responsive to medical therapy using acid-suppressive drugs (namely, proton pump inhibitors; PPI).5-7 Eosinophilic esophagitis is increasingly recognized as causative of a variety of esophageal symptoms such as dysphagia, odynophagia, and heartburn. However, because EoE is newly recognized, awareness of this disease among primary physicians may be limited. In particular, it is important to differentiate between EoE and gastroesophageal reflux disease (GERD), which can cause similar clinical signs and symptoms.
Eosinophilic esophagitis is strictly speaking a clinicopathologic condition comprising a spectrum of somewhat nonspecific symptoms, endoscopic evidence, and histopathologic appearance and consequently diagnosis can be challenging.5 During the past two decades, however, intense research on the etiology of EoE has elucidated its underlying molecular, genetic, and environmental predisposing factors and provided many clues to its successful intervention. This short introductory review provides an overview of the cardinal clinical features, approaches to diagnosis, and some commonly used management practices for EoE from a primary clinician’s perspective.
Pathophysiology
The esophagus is an immunologically active organ that, while normally devoid of eosinophils, rapidly recruits these inflammatory cells in response to gastric acid insults, infectious stimuli, and swallowed (food) allergens as well as inhaled (aero) allergens.2 In patients with EoE, however, the presence of esophageal eosinophilia persists as a chronic inflammatory state that causes uncomfortable or painful symptoms and may eventually lead to the development of long-term complications such as subepithelial fibrosis and esophageal stenosis.4
Epidemiology
According to the American Gastroenterological Association (AGA), EoE affects approximately 1 in every 2000 people.8 Population-based studies have calculated the annual incidence rate of EoE from as low as 2.1 per 100,000 in the Netherlands to as high as 12.8 per 100,000 in Ohio, United States of America (USA).4 Based on the number of biopsies performed at study centers over time, the incidence rate of EoE seems truly increasing faster than its mere awareness, surveillance, and detection in the community.4 A meta-analysis estimated the overall pooled EoE prevalence as 22.7 per 100,000; the estimated prevalence seems much higher in western than in Asian countries, although the reasons for this trend are unknown.4 Solid epidemiology data for adult EoE in the Kingdom of Saudi Arabia (KSA) are lacking, although in this author’s opinion the frequency is increasing with more patients presenting with EoE in daily practice.
Clinical features
Some of the more common presenting features of EoE and comorbid conditions associated with this disorder are displayed in (Table 1).2 Longstanding dysphagia, heartburn/regurgitation, chest pain, and episodes of food impaction are typical symptoms in adults.2,9 Rarely, food impaction may lead to forceful retching and cause rupture of the esophagus.10 In children, EoE may cause abdominal pain, vomiting, and failure to thrive – likely due to avoidance diets and maladaptive feeding.2,11 In the pediatric population, EoE is usually accompanied by history of atopic complications such as asthma, allergic rhinitis, and eczema.2
- Clinical features of eosinophilic esophagitis.
In both adults and children, EoE exhibits an approximately 70% male predilection. Eosinophilic esophagitis is strongly associated with allergic diseases or positive skin prick tests in up to 70% cases.12 However, patients only rarely experience food anaphylaxis, suggesting distinct mechanisms between EoE and classical IgE-mediated allergy. Indeed, omalizumab, an anti-IgE biologic treatment, is not effective against EoE.10
Endoscopic features
In patients with EoE endoscopy investigation may reveal so-called classic features of concentric mucosal rings (representative of fibrosis), furrows, and narrowed internal esophageal diameter with or without proximal esophageal stenosis (Figure 1). However, endoscopic appearance although helpful is not diagnostic without biopsy confirmation.2 Indeed, in a systematic review and meta-analysis performed by Kim and coworkers13 that included 100 published reports on 4678 EoE patients typical endoscopic features were observed in less than half the overall sample and nearly one fifth had normal endoscopic findings; results of endoscopy sensitivity were modest (range, 15% to 48%) whereas specificity was greater (range, 90% to 95%). Notably, on the other hand, nearly all EoE patients (93%) had at least one characteristic sign on endoscopy. These researchers concluded endoscopy alone is inadequate to predict EoE and biopsies should be obtained from the upper and lower esophagus to confirm the diagnosis, regardless of the esophageal appearance on endoscopy.

- Endoscopy images revealing characteristic signs in patients with eosinophilic esophagitis. A) Mild trachealization (concentric mucosal rings) and narrowing of the esophageal lumen. B) Furrows, C) whitish exudates, D) whitish exudates with furrows, E) eosinophilic abscess, F) stricture
Esophageal fibrosis and strictures
Chronic eosinophilia of EoE may ultimately lead to esophageal fibrosis and stricture formation.14 Consequences of these structural derangements include dysmotility and stiffening of the normally compliant tubular esophagus resulting in food impactions even in the absence of stricture. Extent of tissue remodeling in the damaged esophagus may be characterized using a validated endoscopic scoring system such as EoE Endoscopic Reference Score (EREFS).15 Eosinophilic esophagitis endoscopic reference score is used to determine severity of 5 endoscopic findings such as edema, rings, exudates, furrows, and strictures. This tool has been shown accurately to identify adult and pediatric patients with EoE and may be used as an outcome measure to follow their response to treatment.15,16
Histopathology
Diagnosis of EoE is dependent on eosinophilic infiltration of the squamous epithelium.2 A cell count >15 eosinophils/hpf is indicative of EoE.5–7 Eosinophilic infiltration of superficial mucosa mostly occurs in the proximal esophagus although there is usually concomitant involvement in distal esophagus.2 Biopsy samples showing increased eosinophilic infiltration in upper esophagus are more specific for EoE; contrarily, the related condition GERD may be associated with eosinophilic infiltration in the distal esophagus, albeit at a lower density (<10/hpf). Biopsy specimens often also display high numbers of dendritic cells, degranulating mast cells, and CD8+ T cells.17 Many patients with EoE present with a thickened esophageal mucosa and basal layer hyperplasia.17 Epithelial integrity is compromised as evidenced by increased intercellular spaces and, ultrastructurally, decreased junctional proteins.14
Impaired barrier function
Eosinophilic esophagitis biopsies readily reveal dilated intercellular spaces suggestive of impaired barrier function – which has been supported by ex vivo experiments looking at permeability and resistance.17 Impaired barrier function in turn promotes tissue remodeling and eosinophil adhesion, as well as increased food antigen uptake in the esophagus, propagating allergic esophageal inflammation.17 Eosinophils infiltrating the EoE mucosa release granules containing major basic proteins (MBPs) and cytotoxic matrix including eosinophil-derived neurotoxin (EDN), which activates dendritic cells to evoke a Th2 cell-mediated immune response. Eosinophils are known also to express a variety of inflammatory cytokines that modulate the localized immune response. Notably, eosinophil-derived transforming growth factor (TGF)-ß is linked with epithelial growth, fibrosis, and tissue remodeling, which are associated with fibrostenotic complications in EoE.17 TGF-ß also alters fibroblast phenotype to myofibroblast and induces esophageal smooth muscle contraction and hypertrophy, enhancing esophageal rigidity.18
T-helper type 2 activity
Several lines of evidence suggest EoE is an atopic disorder involving allergen-specific Th2 cells. Eosinophilic esophagitis is usually responsive to dietary elimination of food allergens, for example by administering empirical elimination diets or elemental diets (that is, containing amino acids), and the condition relapses on reintroduction of similar foods containing culprit antigen.10 Inhaled aeroallergens can also trigger EoE symptoms and this observation may be an artifact of cross-sensitization to food allergens.10
In individuals with EoE food allergens are believed to trigger a Th2-type reaction resulting in secretion of Th2 cytokines such as interleukin (IL)-4, IL-5, and IL-13.19 Interleukin-5 induces eosinophil production and trafficking to the esophagus whereas IL-13 induces esophageal epithelial cells to secrete eotaxin-13, which drives eosinophil chemotaxis and activation.19 Interleukin-5 and IL-13 have been implicated in the pathogenesis of EoE and treatment with monoclonal antibodies against these signaling molecules reduces numbers of esophageal eosinophils in children and adults.10,20
Diagnosis
A stepwise approach to reaching a diagnosis of EoE is represented graphically in (Figure 2). In a patient complaining of typical EoE symptoms diagnosis of the condition is confirmed by the presence of esophageal eosinophilia >15/hpf in proximal esophagus with further involvement in distal esophagus.9 Eosinophilic esophagitis endoscopic reference score may be a useful tool to supplement endoscopy investigation. Biopsy samples are examined under routine light microscopy following hematoxylin and eosin (H&E) staining.

- Stepwise approach to diagnosis of EoE. aExample target ≥3 samples from upper esophagus and ≥3 samples from lower esophagus. bTraditional hpf using optical microscopy is equivalent to 0.3 mm2 using digital microscopy.
Because EoE and GERD are likewise characterized by the presence of intraepithelial eosinophils in the esophagus,2,9 and EoE shares many clinical features that overlap with those associated with GERD, it is important to differentiate between EoE and GERD refractory to PPI. Of note, in patients with GERD eosinophilic infiltration is predominately limited to distal esophagus whereas in those with EoE eosinophilia is usually seen in both upper and lower esophagus. A PPI trial is nonetheless recommended in patients with suspected EoE since a substantial proportion of patients with clinical and histologic features of the disease may respond to these medications.17 So-called PPI-responsive esophageal eosinophilia (PPI-REE) might be considered a subtype of EoE or a different stage of the same disorder.17
Treatment
Treatment recommendations have been published in the form of guidelines by a number of professional societies.7,8 A detailed analysis of various treatment recommendations is beyond the scope of this review; herein, a brief summary of effective therapeutics is presented.
According to the British Society of Gastroenterology (BSG) and the British Society of Paediatric Gastroenterology, Hepatology and Nutrition (BSG/BSPGHAN) the aim of treatment in EoE is to induce long-term clinical and histologic remission.7 Hence the BSG/BSPGHAN treatment algorithm recommends EoE patients starting pharmacologic or diet therapy be reevaluated for response in terms of symptoms improvement and endoscopic/histologic evidence for mucosal healing 8-12 weeks post-initiation. Patients with EoE should receive consultations jointly by a gastroenterologist and an allergy specialist.7
Diet restriction therapy should be administered with support from an experienced dietitian so as to achieve nutritional adequacy. Six-food elimination diet may be more effective than 2- or 4-food elimination diet but long-term adherence to this regimen is considered problematic.7 Pharmacologic therapy using PPI or topical steroids (available as a variety of drugs, dosing, and delivery systems) may be effective at inducing histologic and clinical remission. Patients who respond to induction therapy on these agents may go on to achieve sustained remission up to 1-2 years.7
Proton pump inhibitors (esomeprazole or omeprazole both 40 mg bid, lansoprazole or dexlansoprazole both 30 mg bid) or swallowed topical steroids (fluticasone, budesonide respules mixed with sucralose, or Jorveza orodispersible tablet) may be effective alone or in combination therapy (Figure 3). For instance, in a large-scale trial carried out in active EoE patients in Europe Jorveza (budesonide oral tablet) was demonstrated significantly more effective than placebo at inducing and maintaining clinical and histologic complete remission up to 48 weeks.21,22 Encouraging phase 2b results were also published for fluticasone orally disintegrating tablet, which elicited significant histologic and endoscopic improvements as well as significant reductions of Global EoE Symptom Score at all test doses versus placebo in prior PPI-failure patients following treatment for 12 and 52 weeks.23 Clinical studies of ciclesonide and mometosone preparations for EoE are underway.24

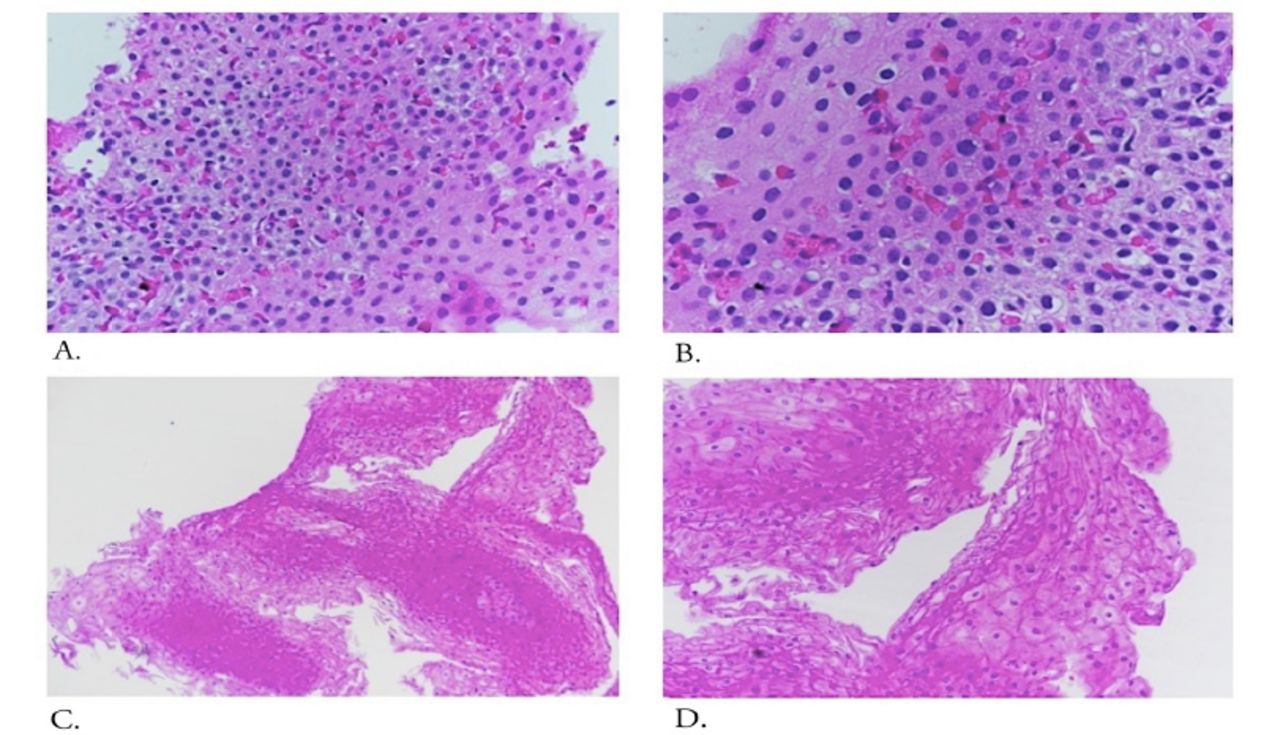
- Biopsy samples obtained from proximal esophagus of a 44-year-old male patient who was diagnosed with active EoE (marked eosinophilia [>40/hpf] associated with degranulation and basal epithelial hyperplasia; A: original magnification, x400; B: x600) and subsequently achieved complete remission following treatment (no evident pathology; C: original magnification, x100; D: x200). He was prescribed omeprazole 40 mg bid plus swallowed topical steriods (fluticasone [Flixotide] 125 μg four puffs twice daily) for 8 weeks with no adverse effects.
The British Society of Gastroenterology and the British Society of Paediatric Gastroenterology, Hepatology and Nutrition guideline does not recommend systemic steroids in EoE.7 It does, however, acknowledge early results from preliminary studies of biologic medications used in other allergic conditions such as dupilumab (anti-IL-4/IL-13), cendakimab (anti-IL-13), and benralizumab (anti-IL-5) suggesting improvements of dysphagia symptoms and reduction in mean eosinophil counts in patients with EoE. These novel monoclonal antibodies show promise as future treatment options. Indeed, following successful clinical trial,25 the United States Food and Drug Administration extended approval of dupilumab for the treatment of EoE in adults and children in May 2022.26 In that phase 3, randomized, placebo-controlled trial dupilumab administered by once-weekly subcutaneous injection led to histologic remission (defined as eosinophil count <6/hpf) in 60% patients (versus 5% on placebo; p<0.001) and was associated with significant alleviation of dysphagia severity as determined by Dysphagia Symptom Questionnaire.25 Furthermore, patients assigned to receive subcutaneous dupilumab every 2 weeks exhibited similar trends in histologic and symptomatic improvements, albeit nonsignificant versus placebo.25
In EoE patients complicated with fibrostenotic change (narrow caliber esophagus <13 mm and/or strictures) despite anti-inflammatory drugs endoscopic dilatation procedures may prove beneficial.7 Individual patients complicated with stricture may require initial dilatation to abrogate dysphagia and in those with recurrence repeat dilatation sessions could be indicated.
In a technical committee exercise reviewers from the AGA Institute collected and evaluated published evidence from the literature on the usefulness of multiple routinely applied therapeutics against symptomatic EoE in adults and children such as PPIs, topical glucocorticosteroids, systemic glucocorticosteroids, elimination diet therapy, and novel biologics.8 Using reduction of esophageal eosinophil count <15/hpf as measure of successful outcome, these researchers concluded few treatments have moderate or better certainty of producing this effect.
Topical glucocorticosteroids are associated with moderate certainty to reduce eosinophil cell count <15/hpf in the short term (4-12 weeks) but very low certainty as effective maintenance therapy beyond this timeframe.
Systemic glucocorticosteroids may exert similar efficacy as their topical counterparts but are associated with higher risk of long-term adverse events.
Over short-term treatment periods elemental diets may be efficacious with moderate certainty, 4- and 6-food elimination diets with low certainty, and diet modified based on allergy testing and that with 1–2-food empiric elimination with very low certainty.
Very low certainty was reported for effectiveness of PPIs in patients with esophageal eosinophilia.
Low or very low certainty was reported for anti-IL-5 therapy, anti-IL-13 therapy, anti-IgE therapy, monetalukast, cromolyn, and anti-TNF therapy.
Conclusion
The clinicopathologic entity known as EoE is becoming a major cause of upper gastrointestinal morbidity worldwide.4 Eosinophilic esophagitis is often associated with dysphagia, heartburn, chest pain, and episodes of food impaction in adults.2,9 Indeed, food impaction, a medical emergency, is often the first sign of EoE in this population.9 In children, EoE may cause abdominal pain, vomiting, and failure to thrive.2,11 Eosinophilic esophagitis is a chronic and potentially serious condition that may lead to esophageal fibrosis and stricture formation.14
Epidemiology figures suggest the prevalence of EoE is approximately 1 in 2000 people and seems increasing.4,8 However, awareness of the endoscopic implications of EoE among primary physicians may be limited. This brief review describes the clinical features, diagnostic criteria, and available treatments against EoE. Eosinophilic esophagitis is a clinicopathologic condition characterized by nonspecific symptoms and common endoscopy features such as rings and furrows with or without stenosis, and requires a conclusive biopsy revealing >15 eosinophils/hpf to make the diagnosis. Hence the road to elucidating this condition in daily practice can be challenging.5 In a patient suspicious for EoE endoscopy and multiple esophageal biopsies are the recommended primary investigations.9 Following diagnosis, a range of treatment options is available that may successfully induce long-term clinical and histologic remission.7 Recommended strategies include diet restriction therapy, PPI, and topical steroids. Furthermore, biologics therapy using monoclonal antibodies is emerging as a promising intervention against EoE – indeed, the anti-IL-4/IL-13 antibody dupilumab was recently approved for the treatment of EoE in adults and children in the USA.25,26
In conclusion, among affected individuals, EoE can be successfully maintained as a moderately benign condition with vigilant observation and a range of useful therapeutics available for its management. Although several traditional and newer treatments for EoE are currently undergoing clinical evaluation, there is no consensus on sequencing or guidance for switching therapy in patients who experience recurrence. Large-scale data on treatment success for patients with EoE in Saudi Arabia are lacking and deeper attention to this upsurging disease is needed.
Acknowledgment
The author thanks the patients and staff at King Khalid University Hospital and King Saud University, Riyadh, KSA. Histopathology images were kindly provided by Dr Abdulmalik Alsheikh, Pathology and Laboratory Medicine, Security Forces Hospital, Riyadh. Editing services were performed by Scribendi, Inc., Chatham, ON, Canada.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.