

ABSTRACT
Objectives: To examine the significance of neutrophil gelatinase-associated lipocalin (NGAL) and tumor necrosis factor-alpha (TNF-α) in women with gestational diabetes mellitus (GDM) and their correlation with insulin resistance and metabolic markers.
Methods: Blood samples from maternal and cord sources were obtained from 289 pregnant women, divided into GDM, prediabetic, and normal pregnancy groups. Serum levels of NGAL, TNF-α, insulin, fasting blood sugar (FBS), homeostasis model assessment-estimated insulin resistance (HOMA-IR), triglycerides, cholesterol, and so on were measured. Statistical analyses, including the Kruskal-Wallis test and Mann-Whitney U test, were used to compare NGAL levels across patient groups and ethnicities.
Results: Women with GDM showed significantly higher serum NGAL and TNF-α levels compared to prediabetic and normal pregnancy groups. The NGAL levels positively correlated with key metabolic markers such as FBS, insulin, HOMA-IR, triglycerides, and cholesterol, suggesting a link between elevated NGAL and insulin resistance. In the GDM group, there was also a positive association (r=0.366) between NGAL and TNF-α values. No significant variation in NGAL levels was observed between non-tribal and tribal women.
Conclusion: Elevated levels of NGAL and TNF-α in women with GDM are linked to increased insulin resistance, excessive gestational weight gain, and higher neonatal morbidity risk. These findings underscore the possible involvement of these inflammatory markers in the development of GDM, emphasizing the need for targeted management of both gestational weight gain and inflammation in GDM patients.
Glucose intolerance that develops or is initially identified during pregnancy is the hallmark of gestational diabetes mellitus (GDM).1 Women with a previous history of GDM are at a higher risk of adverse outcomes for both maternal health and neonatal well-being, as well as an increased chance of developing future type II diabetes, which also affects their offspring, so, placing 2 generations at risk.1
A recent systematic review and meta-analysis found that 13% of pregnant women in India have GDM.2 This represents a substantial group at high risk for adverse perinatal complications if not managed appropriately.
Human neutrophil gelatinase-associated lipocalin (NGAL), an adipocytokine, was initially discovered in human neutrophils and is expressed in various tissues, including the liver, kidneys, and adipose tissue.3,4 Obesity and diabetes are metabolic disorders intimately linked to the overexpression of NGAL in blood and multiple other tissues.5 Several studies indicate that elevated NGAL levels are strongly associated with the onset of insulin resistance and high blood sugar.6-8 Prior clinical research has shown that serum NGAL levels in individuals with type-2 diabetes mellitus were markedly elevated and were correlated with several indicators of insulin resistance, including fasting blood glucose (FBS).9 Studies have reported that individuals with type-2 diabetes mellitus have notably higher serum NGAL levels, which are positively linked to insulin resistance and diabetes progression.10 Women who later developed gestational diabetes showed significantly higher circulating NGAL levels during the first trimester compared to the control group.11 Research has indicated that NGAL expression levels in adipose tissue are significantly higher in overweight women with GDM than in those of normal weight.4
In India, the incidence of GDM is on the rise.12 There is notable variation in the reported prevalence rates of gestational diabetes in India.13 Recent National Family Health Survey data indicates that the prevalence of GDM among pregnant women in India increased from 0.53% (in 2015-2016) to 0.80% (in 2019-2020) at the national level.14 Currently, there is insufficient data on GDM cases in Tripura, India, and their correlation with other potential factors.
Tripura, a northeastern state of India, possesses a distinct population characterized by its unique socio-economic and cultural context. Exploring GDM in the current context would facilitate the assessment of its prevalence and associated risk factors in this northeastern state of India, thereby enhancing maternal and child health outcomes. With this background, the study was designed to examine NGAL levels in serum of pregnant women and cord blood samples (during the time of termination) with and without GDM at a tertiary care hospital in Tripura, India, and to evaluate its link with serum tumor necrosis factor alpha (TNF-α) among the participants.
Methods
This cross-sectional study was carried out from June 2021 to December 2023, in pregnant women attending the Obstetrics and Gynecology Department at a tertiary care hospital (Govind Ballabh Pant Hospital) in Tripura, India. The study included 3 groups: group 1 (97 pregnant women diagnosed with GDM), group 2 (96 age-matched pregnant women with normal glucose tolerance [NGT]), and group 3 (96 prediabetic pregnant women).
The inclusion criteria included pregnant women with singleton pregnancies who were nonsmokers, not on medications affecting carbohydrate metabolism, and classified as GDM, NGT, or prediabetic.
The exclusion criteria were pregnancy-induced hypertension, preeclampsia, and preterm rupture of membranes.
The ethical permission was obtained before commencement of the study from the institutional ethics committee of Agartala Government Medical College, Tripura, India (ref. No.: F.4(5-234)/AGMC/Academic/IEC Meeting/2020/783, Dated, 18/01/2021). Confidentiality was maintained at each step. All participants were included in the study after obtaining a written info informed consent.
The data was obtained in Obstetrics and Gynecology Outpatient Department, ensuring confidentiality, with a pre-designed and pre-tested questionnaire focused on fundamental demographic factors such as age in completed years, ethnicity, and so on. The GDM was diagnosed using a single-step technique, consistent with World Health Organization (WHO) standards.15 Blood samples were collected from the maternal vein prior to the caesarean section and from the umbilical vein both before placental delivery and after fetal birth. Blood samples were collected in tubes without anticoagulants, allowed to coagulate, and then immediately centrifuged at 999g for 10 minutes. The serum was stored at -80°C until analysis.6
Fasting plasma glucose and lipid profile were analyzed using an automatic biochemical analyzer (ERBA - XL 640). Fasting insulin (FINS) was measured using an enzyme-linked immunosorbent assay kit (Calbiotech, USA). The insulin sensitivity was assessed using the homeostasis model assessment (HOMA) index according to the formula.16 Estimation of serum and cord blood NGAL was carried out by using the enzyme-linked immunosorbent assay kit (Bioassay, China) according to the manufacturer’s protocol. Serum TNF-α level was quantified using a human TNF-α ELISA kit (Diaclone, France), and the detection limit was at 7.8 pg/ml.
Statistical analysis
All the collected data was entered, reviewed for consistency, and analyzed using the Statistical Package for the Social Sciences, version 25.0 (IBM Corp., Armonk, NY, USA). Mean ± standard deviation (SD) and percentage were used for descriptive statistics. Appropriate bivariate non-parametric tests examined socio-demographic characteristics and results. Group comparisons used independent t-tests. Significant differences in data comparisons were indicated by p-values of <0.05. Results were provided with a 95% confidence interval (CI). The distribution of maternal NGAL levels across the 3 study groups was analyzed by Kruskal-Wallis test. The maternal NGAL levels between non-tribal and tribal women were analyzed by Mann-Whitney U test.
Results
A total of 5370 pregnant women attended the Obstetrics and Gynecology Outpatient Department of the hospital during the study period (June 2021 to December 2023). Among them, a total of 289 patients, consisting of 97 GDM patients in the test group, 96 normal pregnant women as controls, and 96 prediabetic pregnant women, participated in this study. The mean age of the 3 study groups was not different statistically (p=0.30), as controls were selected based on age matching (Table 1). Other demographic details for all these patients are depicted in Table 1. It was observed that out of 97 GDM patients reported, only 11 (11.3%) were autochthonous pregnant women; the remaining were all Bengali, namely, non-tribal. Women with GDM were significantly overweight compared to pre-diabetic and normal pregnant women. Most of the biochemical parameters differed significantly among the 3 groups of study participants, which is depicted in Table 2. The women with GDM exhibited significantly higher FBS levels, cholesterol, and triglycerides than those of normal pregnant patients (Table 2). The HOMA-IR is extensively used as a significant surrogate indicator of insulin resistance.16 In comparison to the other 2 groups, the GDM group had significantly higher levels of FINS and HOMA-IR. In addition, it was also seen that the GDM group had a significantly lower homeostasis model assessment of beta-cell function (HOMA-beta) compared to the pre-diabetic and normal pregnant women (Table 3).
- Clinical and sociodemographic characteristics of gestational diabetes mellitus, pre-diabetic, and normal pregnant women.
- Comparison of biochemical markers in gestational diabetes mellitus, normal, and pre-diabetic pregnant women.
- Insulin indices of gestational diabetes mellitus, normal, and prediabetic pregnant subjects.
Fasting serum NGAL concentrations of maternal blood and cord blood were significantly higher in women with GDM than the other 2 groups of women (Table 4). Moreover, the serum NGAL levels of women with GDM showed a significant correlation between the biochemical parameters, like FBS, insulin, HOMA-IR, HOMA-beta, TNF-α, triglyceride, cholesterol, and high-density lipoprotein (Table 5). The results demonstrated a positive correlation (r=0.366) between serum NGAL and the level of serum TNF-α in women with GDM.
- Comparison of maternal Serum neutrophil gelatinase-associated lipocalin and cord blood neutrophil gelatinase-associated lipocalin levels among gestational diabetes mellitus, normal, and prediabetic pregnant women.
- Correlation of maternal serum neutrophil gelatinase-associated lipocalin levels with biochemical parameters.
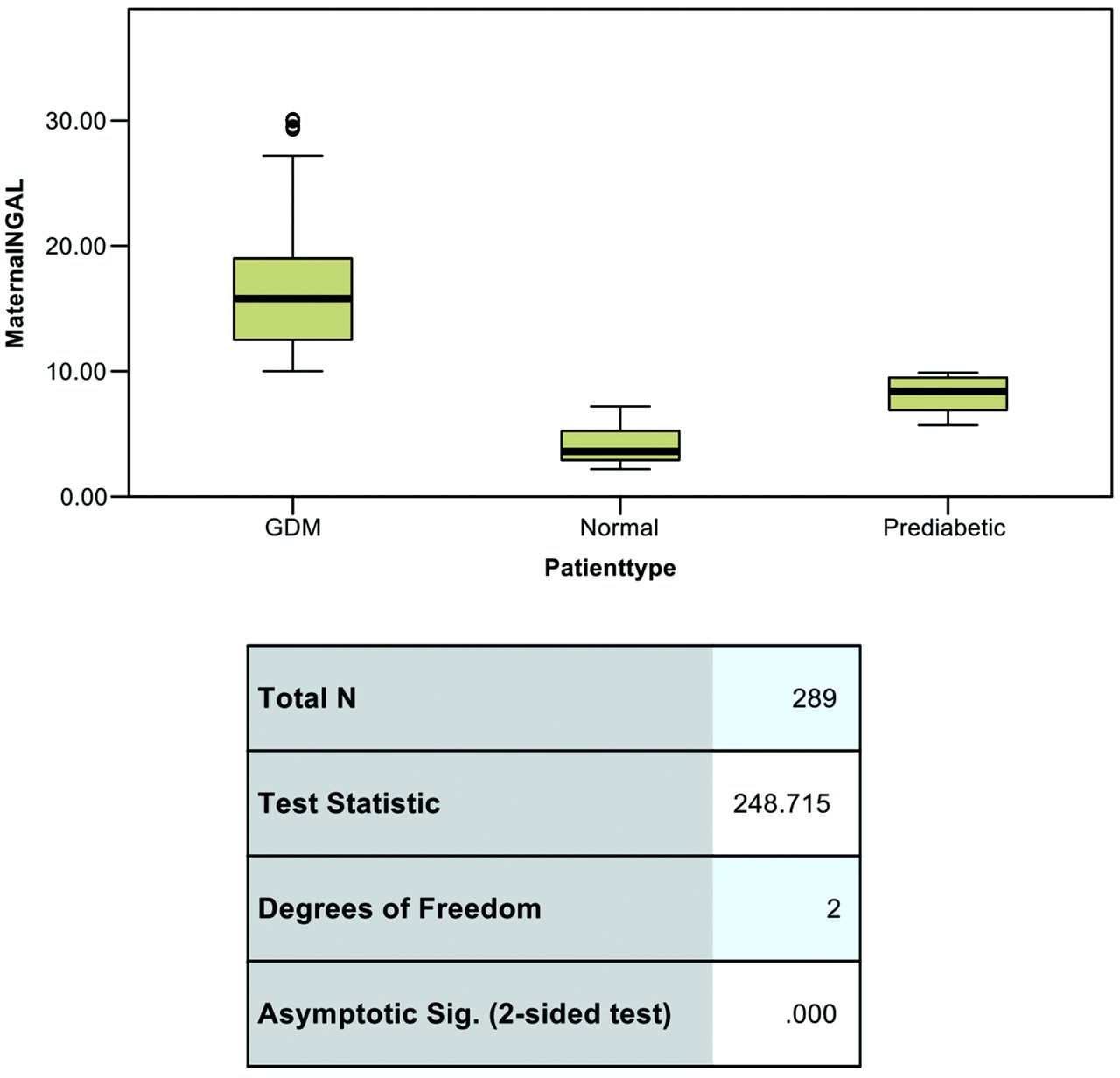
To assess the differences in maternal NGAL levels among patient groups with GDM, normal, and prediabetic conditions, a Kruskal-Wallis test was carried out. The results revealed a statistically significant difference in NGAL levels across the 3 groups (test statistics, H=248.715, p<0.001). As shown in Figure 1, the GDM group displayed the highest median NGAL levels, with some data points identified as outliers, indicating greater variability within this group. The prediabetic group had lower median NGAL levels than the GDM group but higher than the normal group, which exhibited the lowest NGAL levels. These findings suggest that maternal NGAL levels vary significantly with patient type, with GDM patients exhibiting elevated NGAL levels compared to both normal and prediabetic groups.

{kind=link}
- Kruskal-Wallis test for comparing serum neutrophil gelatinase-associated lipocalin levels among 3 groups of study participants. NGAL: neutrophil gelatinase-associated lipocalin, GDM: gestational diabetes mellitus
Discussion
Maternal and child health are significantly influenced by both weight gain prior to pregnancy and throughout the pregnancy.17 Adequate gestational weight gain reduces difficulties associated with pregnancy and the health of the fetus and infant.17 Gestational diabetes mellitus and abnormal weight gain during pregnancy, whether excessive or insufficient, are major medical concerns.17 Increased neonatal morbidity was shown to be associated with substantial pregnancy-related weight gain in mothers diagnosed with GDM.18 Compared to the prediabetic and normal control groups, women with GDM gained a significant amount of weight, according to our study. Since HOMA-IR differs significantly between normal weight and obese people, it is somewhat connected with body weight.19 Similarly, our present study demonstrated that women with higher body weight had increased HOMA-IR compared to normal as well as prediabetic pregnant women. Neutrophil gelatinase-associated lipocalin, or Lipocalin-2, is a 25-kDa secretory glycoprotein first discovered in the granules of human neutrophils and mouse renal cells.11 Numerous investigations have demonstrated that NGAL is associated with obesity by enhancing IFNg expression, which subsequently induces adipogenesis in adipose tissues.20,21 There is a well-established correlation between insulin resistance and obesity, highlighting its significant scientific and clinical importance.22 This relationship is particularly evident in pregnancy, as the risk of developing GDM is substantially elevated by obesity-associated insulin resistance.22,23 In our current study, we found that the fasting serum NGAL concentrations of maternal blood and cord blood were significantly elevated in women with GDM. So, this elevated serum NGAL level may be responsible for the excessive total weight gain and insulin resistance in our study patients with GDM. The serum NGAL levels of women with GDM showed a positive correlation with biochemical parameters like FBS, insulin, HOMA-IR, triglyceride, and cholesterol, which further reinforces the link between elevated NGAL levels in the GDM group of women with excessive weight gain and insulin resistance. The increased NGAL level in the GDM group of women compared to the prediabetic and normal control groups was further represented by the Kruskal-Wallis test, where it appears that GDM patients have significantly higher NGAL levels compared to normal and prediabetic groups. Mann-Whitney U test showed no significant difference in maternal NGAL levels between non-tribal and tribal patients. TNF-a has been reported to be involved in the development of insulin resistance.24 It serves a critical function in the disruption of insulin signaling pathways by impairing the activity of insulin receptors and associated downstream molecules.25 In our current study, we have also found that higher TNF-a levels in pregnant women are linked to greater insulin resistance, which increases the risk of developing GDM. Results also demonstrated a positive correlation (r=0.366) between serum NGAL levels and TNF-α in women with GDM.
Study limitations
A cross-sectional design limits establishing causality, focus on a single region which may reduce generalizability. More large-scale population studies are required to be carried out in this region of northeast India.
In conclusion, our findings indicate that higher serum levels of TNF-a and NGAL in women diagnosed with GDM are linked to greater insulin resistance, substantial pregnancy-related weight gain, and an increased probability of neonatal morbidity. The positive correlations between NGAL, TNF-a, and key metabolic markers reinforce their possible involvement in the onset of GDM, highlighting the importance of managing weight and inflammatory markers in pregnancy.
Acknowledgment
This study was funded by Indian Council of Medical Research (ICMR) (Grant No. 5/7/1750/Adhoc/RBMCH-2021). The authors are indebted and thankful to the Department of Health Research (DHR), Government of India for providing all logistic support and allowing to carry out the study in the Multidisciplinary Research Unit (MRU), Agartala Government Medical College (AGMC), utilizing its facilities. The authors also gratefully acknowledge Biomitra Life Sciences Pvt. Ltd. for their English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received November 29, 2024.
- Accepted March 2, 2025.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.