

ABSTRACT
Objectives: To establish reference values for peripheral oxygen saturation levels in children using pulse oximetry. Pulse oximetry to assess peripheral oxygen saturation is widely used in pediatric care as part of vital signs monitoring. Although readings between 95% and 100% are often considered normal in clinical practice, recent studies suggest that the normal peripheral oxygen saturation range should be between 97% and 100%.
Methods: This cross-sectional study included children aged ≤18 years attending pediatric clinics and not having respiratory distress or acute illness during their visit. Vital signs and anthropometric measurements were recorded. Oxygen saturation and pulse rate were measured using the Masimo Radical-7 pulse oximeter with age-appropriate saturation probes.
Results: A total of 973 participants were enrolled in the study. The median oxygen saturation was 99%. Most participants (75.9%) exhibited oxygen saturation levels between 99% and 100%, while 24.1% had values between 97% and 98%. Importantly, no participant had an oxygen saturation below 97%. Additionally, statistical analysis showed no significant differences in oxygen saturation across age groups or genders.
Conclusion: The findings highlight the importance of vigilant monitoring in pediatric care, particularly when peripheral oxygen saturation values measured by pulse oximetry fall below 97%. Such readings, especially when consistently observed, should not be dismissed, as they may indicate potential underlying health issues or impending emergencies that warrant further evaluation and intervention.
Oxygen saturation (SpO2) indicates the percentage of hemoglobin in the blood that is bound to oxygen in relation to unbound hemoglobin.1 It is commonly measured using a pulse oximeter, a cost-effective and non-invasive optical device that uses a dual-wavelength photoplethysmography system for continuous blood oxygen level monitoring.2 Pulse oximetry plays a crucial role in pediatric care, where SpO2 is routinely measured as part of vital signs assessments to evaluate the severity of a child’s condition. The World Health Organization (WHO) highlights its importance in detecting hypoxemia, a key indicator of severe illness associated with respiratory, systemic, and post-surgical conditions. WHO guidelines recommend the use of pulse oximetry for all children with emergency or respiratory symptoms, emphasizing its role in early identification of hypoxemia and effective oxygen therapy management.3,4 Additionally, SpO2 is an important screening tool for congenital heart disease in newborns, as consistently low readings may indicate potential heart defects and prompt further evaluation.5
In clinical settings, pulse oximetry readings at sea level are typically regarded as normal within the 95% to 100% range.2 However, some studies propose that the normal SpO2 range should be between 97% and 100%.6-10 Studies have shown that school-aged children with SpO2 levels between 95% and 96% tend to have higher respiratory and heart rates, as well as increased hospitalization rates, compared to those with readings between 97% and 100%.9 Additionally, a persistent SpO2 reading in this range may indicate an underlying pulmonary or cardiac condition that has not yet been identified.6
While previous studies have explored this issue, expanding the data within Saudi Arabia is necessary, highlighting the importance of region-specific research. This study aims to establish reference values for SpO2, as measured by pulse oximetry in apparently healthy children in Jeddah, Saudi Arabia. This contribution will provide valuable insights to enhance clinical practices within the region.
Methods
This non-interventional, cross-sectional study was conducted from November 2023 to September 2024 at the pediatric outpatient clinics of King Abdulaziz University Hospital, Jeddah, Saudi Arabia, a tertiary care center offering weekly outpatient services across thirty specialized pediatric clinics and 3 well-baby clinics. The study mainly targeted children who were apparently healthy and aged 18 years or younger. These children were either patients or companions visiting the clinic. Patients presenting with known cardiac, respiratory, or hematological conditions or those displaying signs of abnormal acute illness, which could influence SpO2, were excluded from the study.
At enrollment, parents or guardians were informed about the objectives of the study, and informed consent was obtained. Vital signs and anthropometric measurements were recorded. The study used the Masimo Radical-7 pulse oximeter (Masimo Corp., Irvine, Calif.) to measure SpO2 and pulse rate in pediatric patients using an age-appropriate saturation probe. Sensors were placed on the index finger, thumb, or first toe. To ensure accurate and consistent SpO2 measurements, strict protocols were followed. Parents were asked to keep the child still during the measurement to minimize motion artifacts that could affect the readings. Measurements were only recorded when the plethysmography waveform signal appeared steady. For SpO2 readings below 97%, measurements were repeated 3 times before recording the final reading. Fingers with nail polish or henna were avoided to prevent interference. Trained individuals were responsible for data collection, and all measurements were either validated or directly carried out by investigators to ensure precision. The sample size for this study was predetermined based on a suitable sample size formula to achieve a 95% confidence level with an acceptable margin of error of 5%.11 Consequently, the determined minimum sample size required for the research was 369 children.
Statistical analysis
Statistical analysis was conducted using IBM SPSS Statistics for Windows (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp). Normal distribution was assessed using histograms and the Shapiro-Wilk test. Descriptive statistics were presented using means and standard deviations for variables with a normal distribution and median (interquartile range [IQR]) for non-normal variables. Categorical variables were presented as numbers and percentages. The Mann-Whitney test was conducted to evaluate differences in SpO2 between genders, and the Kruskal-Wallis H test was used to examine differences in heart rate and SpO2 across various age groups. A p-value of <0.05 was deemed statistically significant.
The study’s protocol and procedures obtained ethical approval from the Unit of Biomedical Research Ethics at the Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia. Prior to enrollment, parents or guardians were fully informed about the study’s objectives, and written informed consent was obtained.
Results
The study enrolled a total of 973 children. Table 1 presents the demographic characteristics of the study population. Males made up 55.2% of the participants, with Arabs being the predominant ethnicity, representing 98.6% of the population. The most common age group amongst the participants was school-aged children (7–12 years), accounting for 37.6%. The mean age of the study population was 7 years.
- Participants’ characteristics (N=973).
Heart rate distribution
Table 2 presents the mean and median heart rate values across different age groups. The overall mean heart rate for all participants was 103 bpm. A statistically significant difference was observed between the age groups, with the mean heart rate decreasing as age increased (p<0.001).
- Mean and median heart rates across age groups.
Oxygen saturation distribution
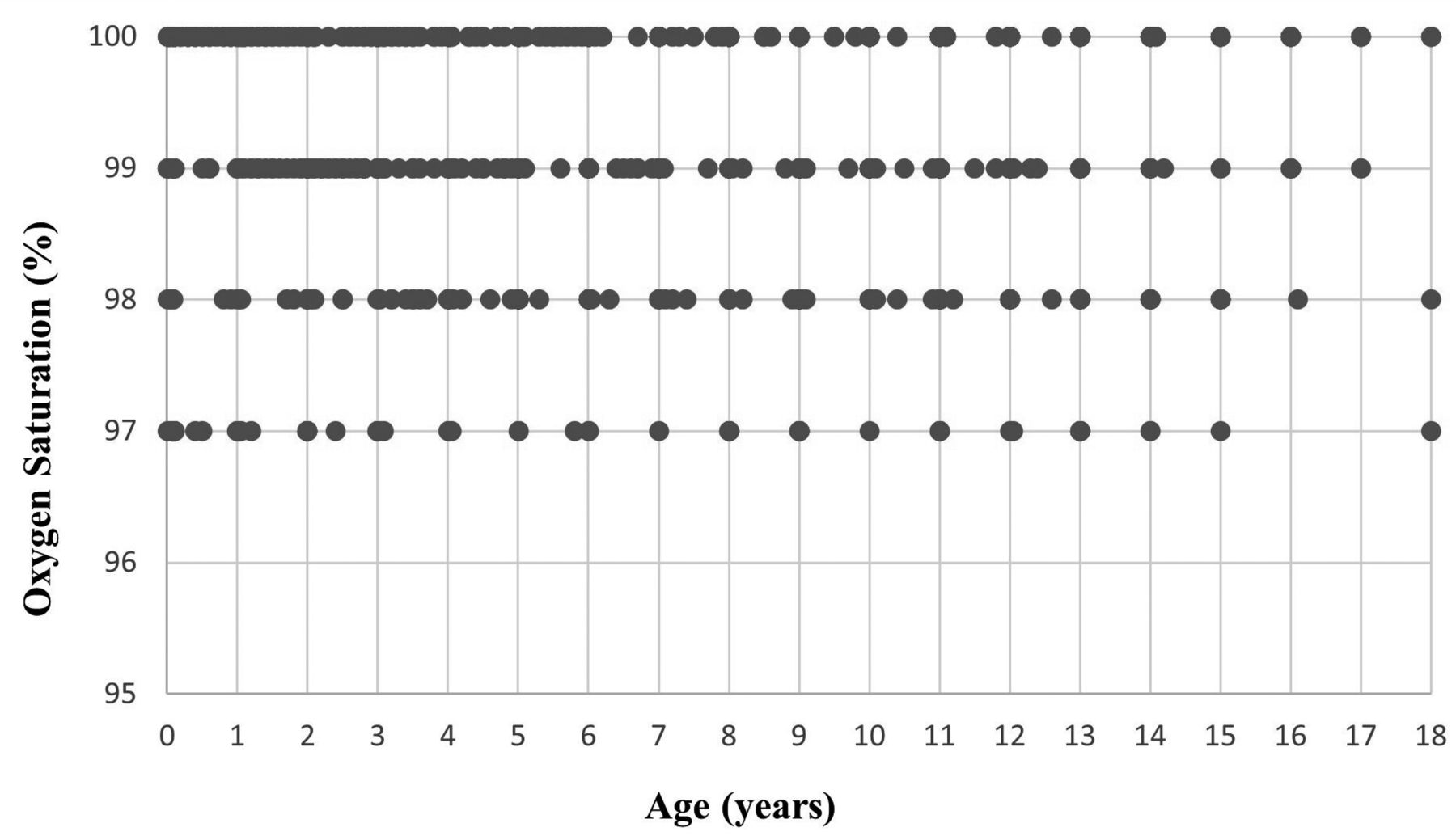
Table 3 summarizes the mean and median values of SpO2 across different age groups. The mean SpO2 for participants was 99.2%, while the median value was 99%. Figure 1 illustrates the distribution of SpO2 values across different ages. The analysis revealed no statistically significant variations in SpO2 among the various age groups (p=0.622). Additionally, no gender differences were observed (p=0.071).

- Scatter plot illustrating the relationship between age (years) and oxygen saturation (%) in a pediatric population. Each dot represents an individual data point. The x-axis represents age in years, ranging from infancy to 18 years, while the Y-axis represents oxygen saturation (%) measured via pulse oximetry. Oxygen saturation values predominantly cluster at 100%, with some variation observed between 97% and 99%. A correlation analysis showed no significant association between age and oxygen saturation (r=0.036, p=0.259)
- Mean and median oxygen saturation values across age groups.
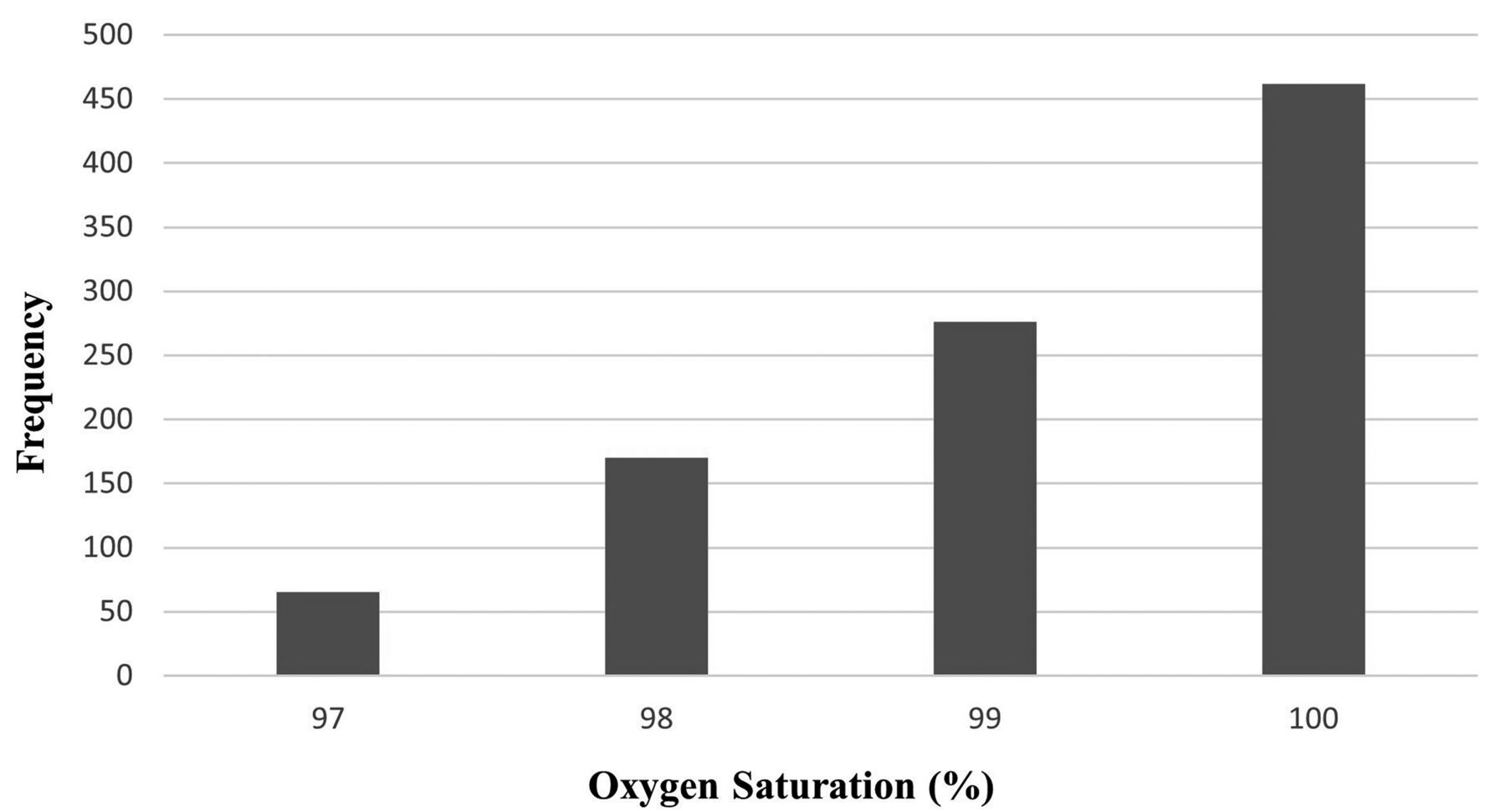
Among the study participants, SpO2 values ranged from 97% to 100%. Notably, 462 children (47.5%) demonstrated saturation levels of 100%, while 276 children (28.4%) had levels of 99%, 170 children (17.5%) exhibited levels of 98%, and 65 children (6.6%) displayed levels of 97%. There were no SpO2 values below 97%. The distribution of SpO2 values in healthy children is shown in Figure 2.

{kind=link}
{kind=link}
- Distribution of oxygen saturation values in healthy children (n=973).Bar chart illustrating the frequency distribution of oxygen saturation values (%) among the study population.The X-axis represents oxygen saturation levels (%) measured by pulse oximetry, while the Y-axis represents the frequency of occurrences for each saturation level. The majority of subjects have an oxygen saturation of 100%, followed by 99% and 98%, with a smaller proportion at 97%.
Discussion
Our study analyzed SpO2 values in healthy children. Traditionally, normal SpO2 levels in children, as measured by conventional pulse oximetry, range from 95–100%.2 However, several studies have suggested redefining what constitutes “normal” SpO2 values.6-10
Since pulse oximetry is now commonly included as the fifth vital sign in emergency departments, it is essential to understand the standard values regarded as normal. We investigated a large cohort (n=973) of pediatric patients attending the outpatient clinic at our tertiary care center using reliable pulse oximetry (such as, Masimo Radical-7 pulse oximeter). Most patients had SpO2 levels of 99–100%, some at 97–98%, and none below 97%. This is consistent with the findings of Mau et al7 who concluded that most patients had SpO2 over 97%, particularly older children. A prospective observational study by Elder et al6 suggested that SpO2 levels of 95–96% could potentially be abnormal.
Other global studies found pulse oximetry results vary with altitude and age. For example, a study by Balasubramanian et al8 determined an average SpO₂ reference of 98.5% in children aged one month to 5 years. Their findings showed a gradual increase in SpO₂ levels with age, reporting values of 98.5% for infants aged one to 3 months, 98.8% for those between 3 months and one year, 98.9% for children aged one to 3 years, and 99.1% for those between 3 and 5 years. Another study12 examined the correlation between age and SpO₂ levels, revealing a direct relationship in children under 5 years, with values ranging from 93% to 100%. This range was slightly lower than reported in previous studies and differed from our findings.
In our cohort, the median SpO₂ level was notably high at 99%, aligning with findings from studies conducted in coastal regions. This may be attributed to the seaside location of our study, as previous research suggests that children living at sea level generally have higher SpO₂ levels than those at higher altitudes.13,14
For instance, a study in eastern India, situated 62 meters above sea level, reported a median SpO₂ of 99.7% in children aged one month to 14 years.10 Similarly, Balasubramanian et al8 examined children up to 5 years of age in Chennai, a coastal city, and found a median SpO₂ of 99%, consistent with our findings.
Moreover, a Japanese study emphasized that SpO₂ levels of 95–96% in school-aged children should not be readily assumed as normal but may have clinical significance in pediatric emergencies.9 These findings highlight the importance of considering environmental factors such as altitude and geographical location when interpreting SpO₂ levels in pediatric populations, as these variables can influence regional variations in oxygen saturation measurements.
Regarding heart rate variations, our data demonstrated a significant decline in heart rate with increasing age, decreasing from a median of 140 bpm (range: 130–150 bpm) in the youngest age group (<1 year) to a median of 92 bpm (range: 83–102 bpm) in the oldest age group (13–18 years). This trend is consistent with existing literature.15
Clinically, SpO₂ measurement through pulse oximetry offers rapid, reliable, and valuable information in various conditions, including respiratory diseases such as asthma exacerbations, chronic lung disease of prematurity, acute bronchiolitis, and pneumonia, as well as cardiovascular conditions, particularly for assessing hemodynamic stability and neonatal screening for congenital heart disease.5,16
SpO₂ plays a crucial role in pediatric monitoring, especially in emergency department triage.4 Patients with SpO₂ values below 97% require thorough evaluation and close monitoring. A retrospective, population-based observational study of school-aged children found that those with SpO₂ levels of 95–96% had significantly higher respiratory rates, heart rates, and hospitalization rates compared to those with SpO₂ levels of 97–100%.9 These findings underscore the importance of not dismissing SpO₂ levels of 95–96% as non-urgent. Instead, a comprehensive assessment of heart and respiratory rates is essential to ensure timely and appropriate intervention.
Study limitations
Our study does have certain limitations. The first is the inherent limitations associated with pulse oximetry itself, such as potential interference from ambient light, motion artifacts, poor perfusion, skin pigmentation, nail polish, artificial nails, and irregular heart rhythms. Secondly, assessing vital signs in children can be challenging due to their tendency to become emotional and restless during measurements. To account for these limitations, we followed a standardized protocol and utilized a modern device specifically designed to minimize interruptions and enhance accuracy.
In conclusion, our study evaluated SpO₂ levels in a diverse cohort of 973 participants, providing valuable reference data for healthy children living in a coastal city. We found a high median SpO₂ of 99%, with no recorded values below 97%. Additionally, no significant differences in SpO₂ were observed across age groups or between genders. These findings highlight the importance of SpO₂ monitoring in pediatric patients, as levels below 97% should not be overlooked but instead carefully assessed for potential underlying health concerns. Our study contributes to the existing literature on pediatric SpO₂ levels and reinforces the vital role of pulse oximetry in clinical practice.
Acknowledgment
We would like to thank American Manuscript Editors (www.americanmanuscripteditors.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 1, 2024.
- Accepted March 20, 2025.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.