


Abstract
Objectives: To evaluate the anatomical variation of arterial collaterals and their prevalence in moyamoya and atherosclerosis.
Methods: Data was collected retrospectively from patients (n=46) database who underwent digital subtraction angiography between January 2010 and December 2018 at the Radiology Department, King Fahad Medical City, Riyadh, Saudi Arabia. Demographic details and clinical data of the patients such as age, gender, etiology, clinical presentation, angiographic staging using Suzuki grading for moyamoya cases, variation of arterial collaterals, and their prevalence, treatment and follow up were obtained.
Results: Four types of collaterals network were observed in atherosclerosis (n=21) and moyamoya (n=25); the leptomeningeal, durocortical, subependymal, inner-interstriatal and intrathalamic networks. More number of collaterals were observed in the moyamoya (n=534) than atherosclerosis (n=40). Leptomeningeal network (n=198, 37.1%) and subependymal network (n=170, 31.8%) were greater than durocortical and inner-interstriatal or intrathalamic in patients with moyamoya. Whereas leptomeningeal network (n=25, 62.5%) and inner-interstriatal or intrathalamic (n=7, 17.5%) were predominant in atherosclerosis. Out of 25 cases of moyamoya, Suzuki grading V was noted in 5 (20%) and grade IV in 13 (52%).
Conclusion: Understanding the dynamics that have evolved in the development of the collaterals and therefore can improve both management and prognosis.
Moyamoya is characterized by an advancing stenosis or occlusion of the terminal part of the internal carotid arteries or proximal part of the anterior and middle cerebral arteries, associated with development of intracranial arterial collaterals. The clinical presentation differs between the pediatric and adult populations, with 2 peaks of incidence at approximately 10 years and 30-40 years. The peak incidence occurs far ahead in females than in males. Adult patients mostly present with intracranial hemorrhages and ischemia, whereas transient ischemic attacks, intellectual decline, seizures and involuntary movements are more common in pediatric population in addition to brain infarctions.1 The development of new blood collaterals is crucial for perfusion of the brain and to avert cerebral ischemia.2 With progressive stenosis or occlusion of the main intracranial arteries, arteriogenesis is activated by fluid sheer stress facilitating endothelial monocyte invasion, release of cytokines and growth factors, proliferation of smooth muscle cells and a surge in the collaterals flow.3
Baltsavias et al4 in 2015, described 4 types of anastomotic networks in moyamoya. Leptomeningeal and durocortical as the superficial meningeal networks and subependymal and inner- interstriatal networks and the inner thalamic as the deep parenchymal networks. Suzuki and Takaku, listed 6 stages of moyamoya that describes the different patterns of disease progression: Grade I = narrowing of the carotid fork; Grade II = initiation of moyamoya collaterals; Grade III = Partial stenosis of the ACA and MCA with intensification of moyamoya collaterals; Grade IV = advanced steno-occlusive changes in the ICA with small portion of ECA collaterals; Grade V= predominant ECA collaterals with further reductions in ICA collaterals; Grade VI = absence of the ACA and MCA with complete disappearance of ICA moyamoya collaterals.5 The idiopathic disease is inherently common in East Asian countries such as Japan and Korea and relatively less common in the Middle East and Western countries. RNF213 is the most common susceptible gene and is often reported with the p.Arg4810Lys founder variant in East Asian patients.6 In Saudi Arabia, moyamoya syndrome constitutes a major risk for stroke in children reflecting commonly an underlying hematological disorder like sickle cell disease.7 Intracranial atherosclerosis is an important etiology for ischemic stroke that contributes to collaterals formation, where well-developed collaterals precludes the severity of cerebral ischemia and represents a prognostic role in moderate and severe stenosis.
In the present study, we intend to evaluate the anatomical variation of arterial collaterals and their prevalence in moyamoya and atherosclerosis utilizing cerebral angiographic imaging.
Methods
Approval was obtained from the Institutional Review Board in King Fahad Medical City (KFMD) (IRB No-18-466). The study was carried out according to the principles of the Helsinki Declaration.
We retrospectively analyzed the collected data of patients (n=46) who underwent digital subtraction angiography between January 2010 and December 2018 at the Radiology Department, KFMC, Riyadh, Saudi Arabia. Only patients whose pretreatment DSA examinations were of sufficient quality were included in this study. Patients with vascular malformations, dissection, vasculitis and also vascular tumors were excluded.
The diagnosis of moyamoya were adapted based on the diagnostic criteria approved by the Japanese Ministry of Health and Welfare.8
The demographic and clinical data for these patients were detailed; including the age, gender, etiology, clinical presentation, variation of arterial collaterals and their prevalence, treatment, and follow up. Angiographic Suzuki staging5 was determined for moyamoya cases. The vascular connections were classified according to the collaterals network namely; the leptomeningeal, durocortical, subependymal, inner-interastriatal or intrathalamic, and their detailed connections were noted.3
Data were entered into Excel sheet and analyzed using the Statistical Package for Social Sciences for Windows, version 22, (Armonk, NY: IBM Corp.). Descriptive statistics were calculated for demographic data as well as the collaterals networks and the detailed anatomical connections.
Results
We outlined the collateral patterns of atherosclerosis (n=21) and moyamoya patients (n=25). Females were more commonly affected than males in both groups.
Tables 1 & 2 depict demographic and clinical data and the collateral networks in the atherosclerosis patients.
Demographic and clinical data of patients with atherosclerosis (N=21).
Vascular connections tabulated according to collateral networks in atherosclerosis.
Tables 3 & 4 depict demographic and clinical data and collateral networks in the moyamoya patients.
Demographic and clinical data of patients with moyamoya (N=25).
Vascular connections tabulated according to collateral networks in Moyamoyagroup.
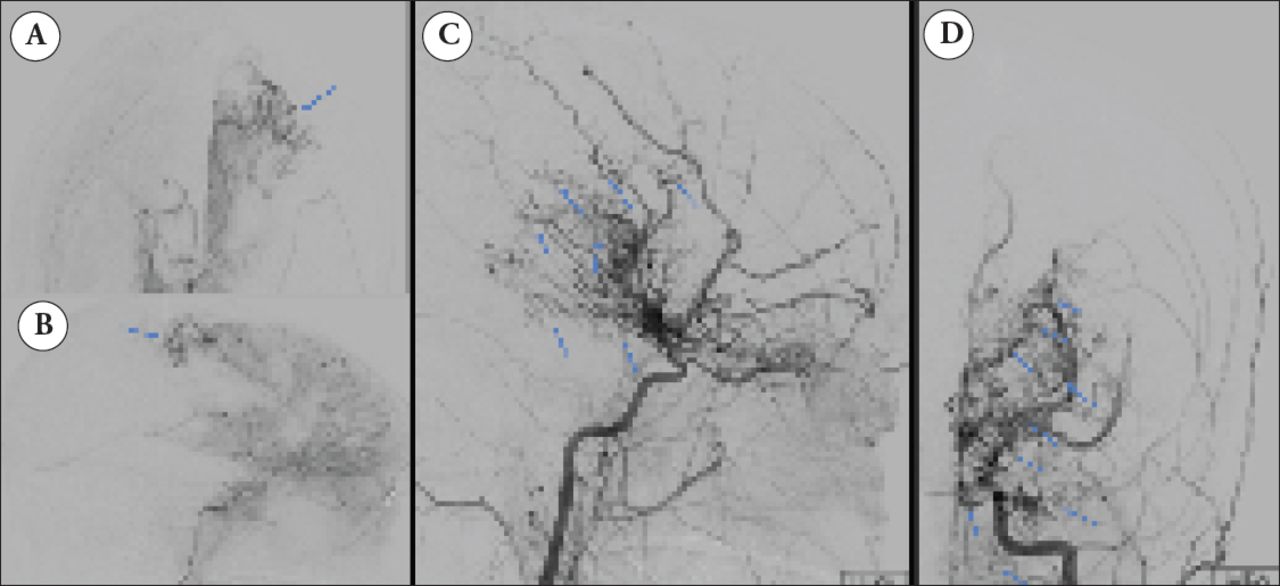
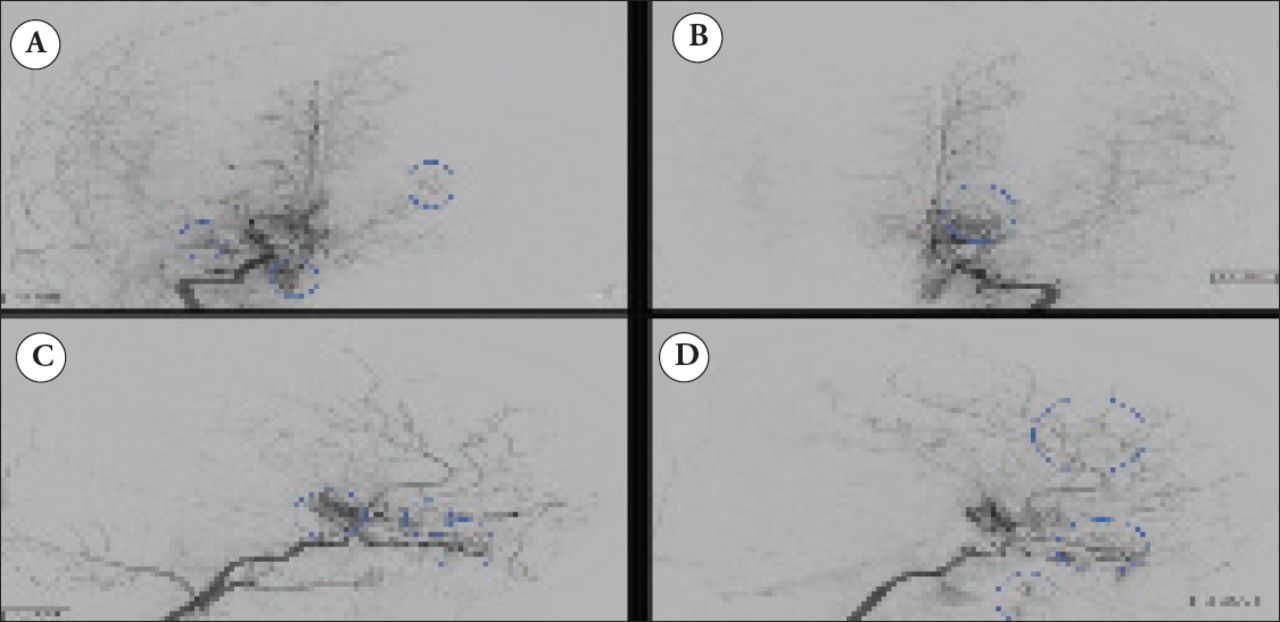
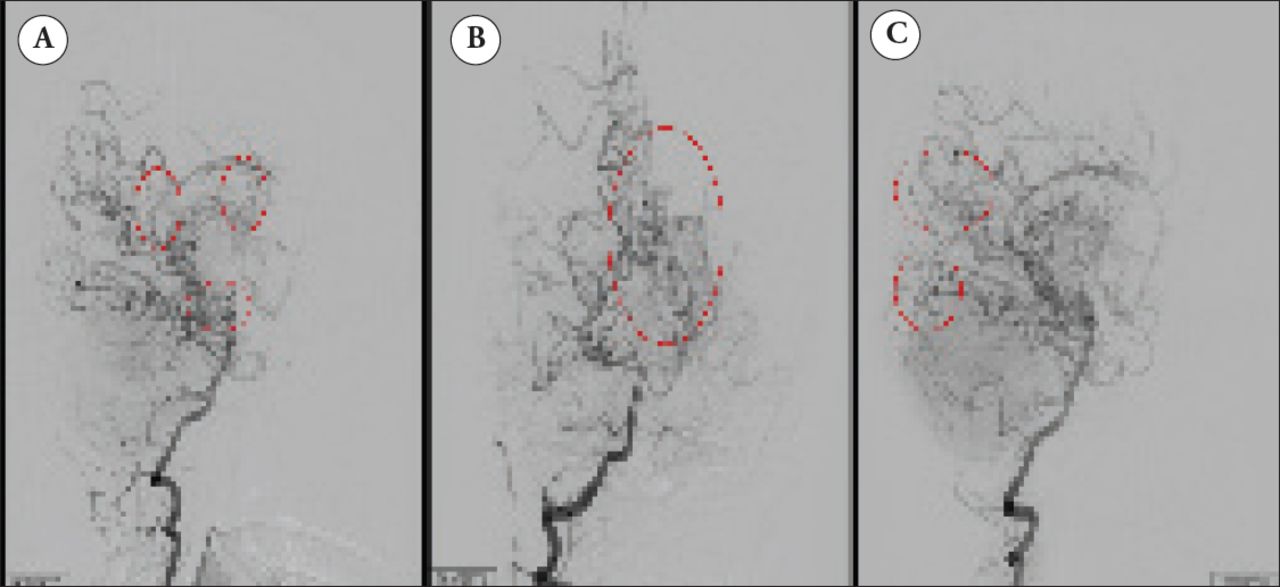
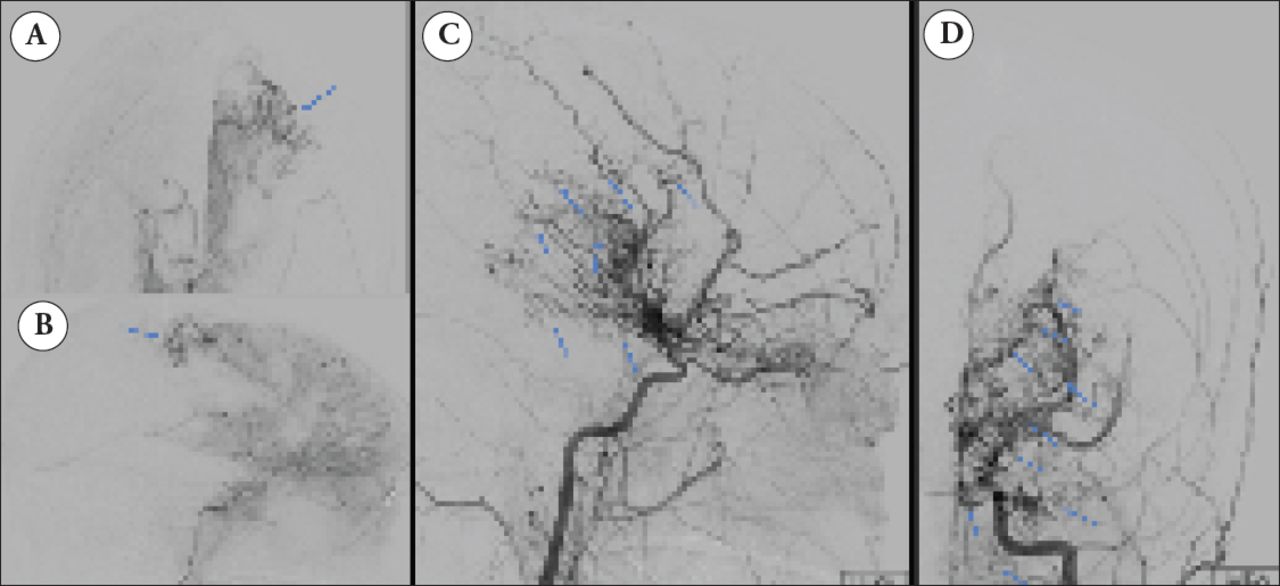
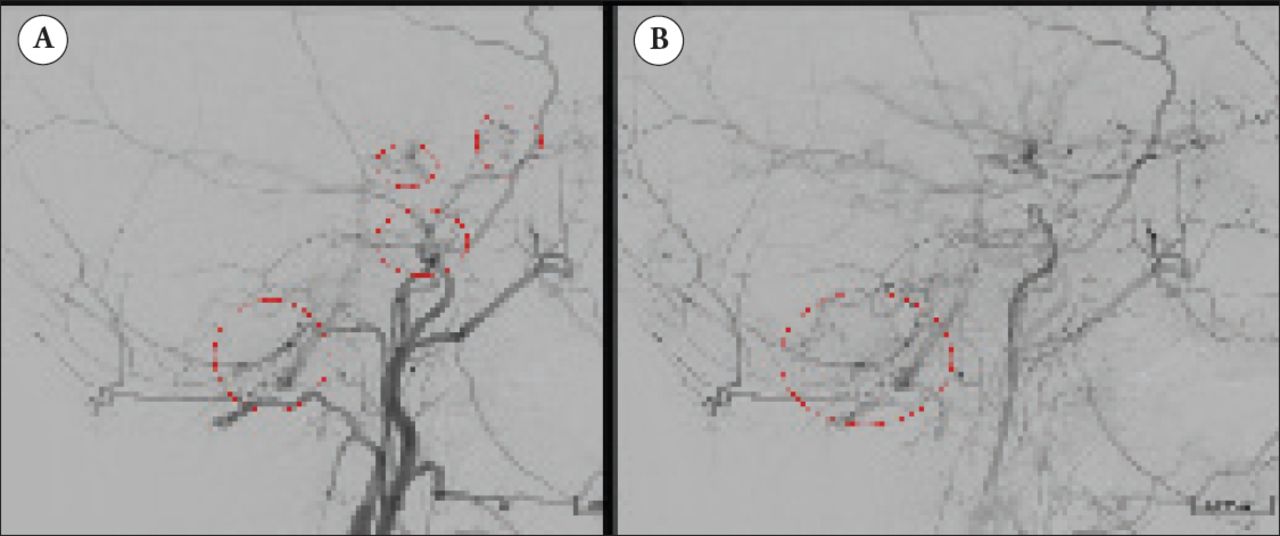
Figures 1-4 cerebral angiographic images demonstrate examples of different collateral networks and arterial variance in moyamoya patients.

Digital subtraction angiogram showing the A & B) frontal and C & D) lateral projection of after selecting the internal carotid arteries. Moyamoya collaterals originating from the lenticulostriate, anterior choroidal, hypophyseal ophthalmic and ethmoidal arteries.

Digital subtraction angiogram after selecting the A & B) right and C & D) left vertebral arteries. Moyamoya collaterals originating from the posterior communicating perforators, thalamoperforators, posterior choroidal, splenial, temporal and parieto-occipital branches.
Digital subtraction angiogram of the A & B) right internal carotid artery. The durocortical collaterals at the right parietal lobe communicating with distal anterior cerebral artery. Selective catheterization of the C & D) left internal carotid artery; extensive collaterals from anterior choroidal, hypophyseal, ophthalmic, ethmoidal, posterior communicating and posterior choroidal arteries. The durocortical collaterals from superficial temporal and middle meningeal arteries supplying the cortical branches of anterior and middle cerebral arteries.

Digital subtraction angiogram after selecting the left common carotid artery. A) The durocortical collaterals from the superficial temporal, middle meningeal and occipital arteries. B) The occipital artery collaterals are seen over crossing the mastoid process.
Different types of collaterals networks were observed in the atherosclerosis (n=21) and moyamoya (n=25). More number of collaterals were observed in the moyamoya (n=534) than in atherosclerosis (n=40). More leptomeningeal (n=198, 37.1%) and subependymal networks (n=170, 31.8%) were observed than the durocortical and inner-interstriatal or intrathalamic networks in moyamoya, whereas leptomeningeal (n=25, 62.5%), and inner-inter striatal or intrathalamic (n=7, 17.5%) networks were predominant in patients with atherosclerosis. The right cerebral hemisphere was more commonly affected in both groups, but infarct localization in the MCA territory was greater in atherosclerosis compared to the multiple anterior circulation territories in moyamoya.
The disease showed interval progression in the majority moyamoya patients on follow up angiographic studies, whereas most atherosclerosis patients improved after either thrombolysis or angioplasty.
Discussion
More number of moyamoya patients are currently being recognized due to advances in medical imaging. This includes factors for predicting disease severity, impending hemorrhages, clinical outcomes and potential complications through magnetic resonance angiography or conventional cerebral angiography.9
Peicong et al10 in 2017 reported that infarction was very common in elderly (40.2%), many patients presented with Suzuki stage 4 or 5 (51.2%), posterior cerebral artery was involved in 22 (25.3%) and post-operative infarction or hemorrhages was 6.9%.10 In our study, the majority of patients were referred for stroke workup in patients with atherosclerosis (n=21) and moyamoya (n=25). A greater number of collaterals were observed in the moyamoya group (n=534) than in the atherosclerosis group (n=40). The leptomeningeal network (n=198, 37.1%) and the subependymal network (n=170, 31.8%) were more predominant than the durocortical and inner-interstriatal or intra thalamic network in patients with moyamoya, whereas the leptomeningeal network (n=25, 62.5%) and the inner-interstriatal or intrathalamic (n=7, 17.5%) networks were more frequent in patients with atherosclerosis. Out of the 25 patients with moyamoya, Suzuki grade V was noted in 5 patients (20%), and grade IV was noted in 13 (52%) patients.
In our study, infarct localization was greater in the MCA territory in the atherosclerosis group, compared to the multiple anterior circulation territories in the moyamoya group. Although posterior circulation stroke is uncommon, PCA involvement is an independent important risk factor as the leptomeningeal collateral from PCA is a significant blood flow source of collaterals.11
In a study conducted by Robert et al,12 duro-pial collaterals from branches of the ECA to the territory of the ACA were observed in 5 hemispheres (6.8%) and perivascular collaterals were observed in 47 hemispheres (63.5%). Ophthalmic artery collaterals were noted in 35 patients (47.3%) and were most frequent in patients with Suzuki grades III-V.12 In our study, the ophthalmic artery was involved in 10% (4 hemispheres) of patients in the atherosclerosis group and 4.7% (25 hemispheres) of patients in the moyamoya group.
According to Liebeskand et al,13 collaterals circulation in atherosclerosis was satisfactorily available for analysis in 287/569 (50%) individuals with proximal arterial stenosis ranging from 50% to 99%. The extent of collateral flow correlated with the percentage of stenosis (p<0.0001), with more severe stenosis exhibiting greater compensation via collaterals. The collateral grade increased with diminished antegrade flow across the lesion (thrombolysis in myocardial ischemia) and the resultant downstream perfusion (thrombolysis in cerebral infarction) (both p<0.001). Collaterals are valuable in compensating for arterial obstruction and also serve as a marker of underlying illness. Patients with profound dynamic collaterals have smaller infarcts.13
The majority of patients in our study showed interval progression in the moyamoya group upon follow-up angiographic studies, whereas the atherosclerosis patients improved after thrombolysis and angioplasty. This difference is likely due to the progressive nature of moyamoya.
Study limitation
Our study is a retrospective study based on sequential conventional angiography.
The existence, timing/appearance of collateral circulation development can be observed in future prospective studies in order to prevent ischemia; also useful in planning the revascularization surgery.
In conclusion, identification of the prevalence of variant arterial collaterals in moyamoya and atherosclerosis is very useful in understanding the dynamics that have evolved in the development of the collaterals and therefore can improve both management and prognosis.
Acknowledgement
The authors would acknowledge the Department of Radiology, King Fahad Medical city, Riyadh for their support and the professional manuscript services of American Journal Experts.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 11, 2019.
- Accepted February 20, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.