


Abstract
Objectives: To first describe the epidemiological data of burns, including burn types and burn-related infections, in adult and pediatric patients. Second, to determine the effect of Methicillin-Resistant Staphylococcus aureus (MRSA) on length of hospital stay and, third, to determine if the microbiological profile differs in patients with severe and non-severe burns.
Methods: This is a retrospective chart review in which medical records of all burn patients admitted to Al-Noor Specialist Hospital, Makkah, Kingdom of Saudi Arabia between January 2016 and January 2017 were reviewed for demographic, microbiological, and burn data using a data-collection sheet. No randomization was necessary as all patients were included. Descriptive and inferential statistics were performed on the collected data.
Results: Of 250 patients, 53.6% were pediatric patients and 68.4% were male patients. The most common organism in blood and wound cultures of minor burns was Staphylococcus aureus. Methicillin-resistant Staphylococcus aureus (MRSA) frequency was 82.5%. Length of stay increased in patients with infected burn injuries.
Conclusion: The pediatric population had a high frequency of burn injuries, representing an incentive for more focused educational prevention programs in that group. Additionally, burn infections carry significant morbidity, and are associated with longer hospital stay. These data can help implement various prevention programs.
Burns are among the most devastating injuries, and lead to great mortality and morbidity. The fourth most common type of trauma worldwide, the World Health Organization (WHO) has estimated that burn injuries result in 265,000 deaths annually and roughly 11 million burn patients needed medical attention in 2004.1 Burn rates within the east Mediterranean region have increased to an annual incidence of 518/100,000 from 112/100,000, with a mean mortality rate that ranges from 5-37%, in the years from 1989 to 2006.2 However, one systematic review showed a decrease in mortality, length of stay (LOS), incidence and burn severity in burn patients worldwide.3 A systematic review of severe burn injuries showed that a common cause of death in severe burn patients was sepsis, accounting for 2-14% of deaths.4 Infections are a great source of mortality and morbidity in burn patients, with burn wounds and the bloodstream being frequent sites of infection. Various bacteria are implicated in burn-related infections. A study showed that Acinetobacter baumannii, followed by Pseudomonas aeruginosa, are the most common organisms in the burn intensive care unit (ICU). Staphylococcus aureus, followed by Pseudomonas aeruginosa, are the most common organisms in the regular burn unit.5 A systematic review of burn wound infections showed that Gram-negative organisms are the most common organisms in burn wounds, with Pseudomonas aeruginosa being the most common organism overall.6 In severe burn patients (≥40% TBSA), Acinetobacter baumannii, Pseudomonas, and Methicillin-resistant Staphylococcus aureus (MRSA) were predominant in burn-related infections.7 There is a local data of burn wound infections from Taif, Saudi Arabia that showed a predominance of Staphylococcus aureus organism, followed by Klebsiella.8
A matter of great concern is the emergence of drug-resistance in Gram-positive organisms. Methicillin-resistant Staphylococcus aureus accounts for 98% of all Staphylococcus aureus infections within the burn ICU, and 67% in non-intensive care burn unit patients. Burn ICU patients have increased rates of drug resistant strains of Gram-negative organisms when compared to those in the regular burn unit.5 Recent studies show that Multidrug-resistant organisms (MDRO) are associated with a greater number of surgical procedures, longer duration of mechanical ventilation, prolonged antibiotic therapy and longer hospitalization.9 One study; however, showed that MRSA, when compared to Methicillin-sensitive Staphylococcus aureus (MSSA), did not increase LOS or mortality. Furthermore, another study showed that multi-drug resistant Pseudomonas, when compared to multi-drug sensitive Pseudomonas, did not increase mortality and LOS.10 Due to the obvious lack of local data about the common burn infection organisms and their impact on burn prognosis, this research was conducted to illustrate the microbiological data of burn victims based on results from the largest burn unit in Saudi Arabia, and their sequelae in order to guide future research efforts in burn management.11
The objectives of this study are to first describe the epidemiological data of burns, including burn types and burn-related infections, in adult and pediatric patients. Second, to determine the effect of MRSA on length of hospital stay and, third, to determine if the microbiological profile differs in patients with severe and non-severe burns.
Methods
A retrospective chart review was conducted of all burn patients who were admitted and treated at Al-Noor Specialist Hospital, Riyadh, Saudi Arabia, between January 2016 and January 2017. The burn unit at Al-Noor specialist hospital is considered the largest in Saudi Arabia in terms of capacity.11 It contains 21 beds and has an average admission rate of 200-250 patients per year. All acute burn patients from all age groups and both genders, with or without blood or wound cultures, admitted during the specified period, were included. Patients with chronic burn wounds and patients transferred from other hospitals were excluded, in order not to affect the microbial profile. Patients with incomplete medical charts were also excluded, making the total excluded patients 13. The pediatric age group was defined as patients <14 years old. Wound cultures were only taken when there were local and systemic signs of infection, such as increasing burn wound depth, erythema, and fever. The wound was copiously irrigated with saline and a swab was taken from the burn wound, not the donor sites. With regards to blood cultures, they were only drawn when patients exhibited systemic signs of infection, such as fever, and a change in white blood cell and platelet counts. The distinction between colonized versus infected wounds on culture results depended on 2 factors. The first factor is the clinical findings of the patient, whether he or she were having an infection or not. The second factor is the quantitative microbiology of the wound swab taken. A wound swab with a microbial load of >105 CFU/g was considered infected.12 Systemic antibiotics were administered as soon as patients showed signs of infection only. The data were collected using a validated data collection form which included the patients’ demographics (age and gender) and burn-related data (type of burn, total burn body surface area, culture results and length of hospital stay). All data were reviewed, organized, and tabulated in a spreadsheet format, which were then encoded into IBM SPSS Statistics (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.).
Quantitative data were represented by mean, median and interquartile range. On the other hand, qualitative data were represented by frequencies and percentages. Comparisons among the groups were conducted using the Mann-Whitney test, student t-test and Chi-square test. Results were deemed significant when p<0.05. This study was conducted in compliance with the declaration of Helsinki and granted ethical approval by the Institutional Review Board (IRB) at the hospital.
Results
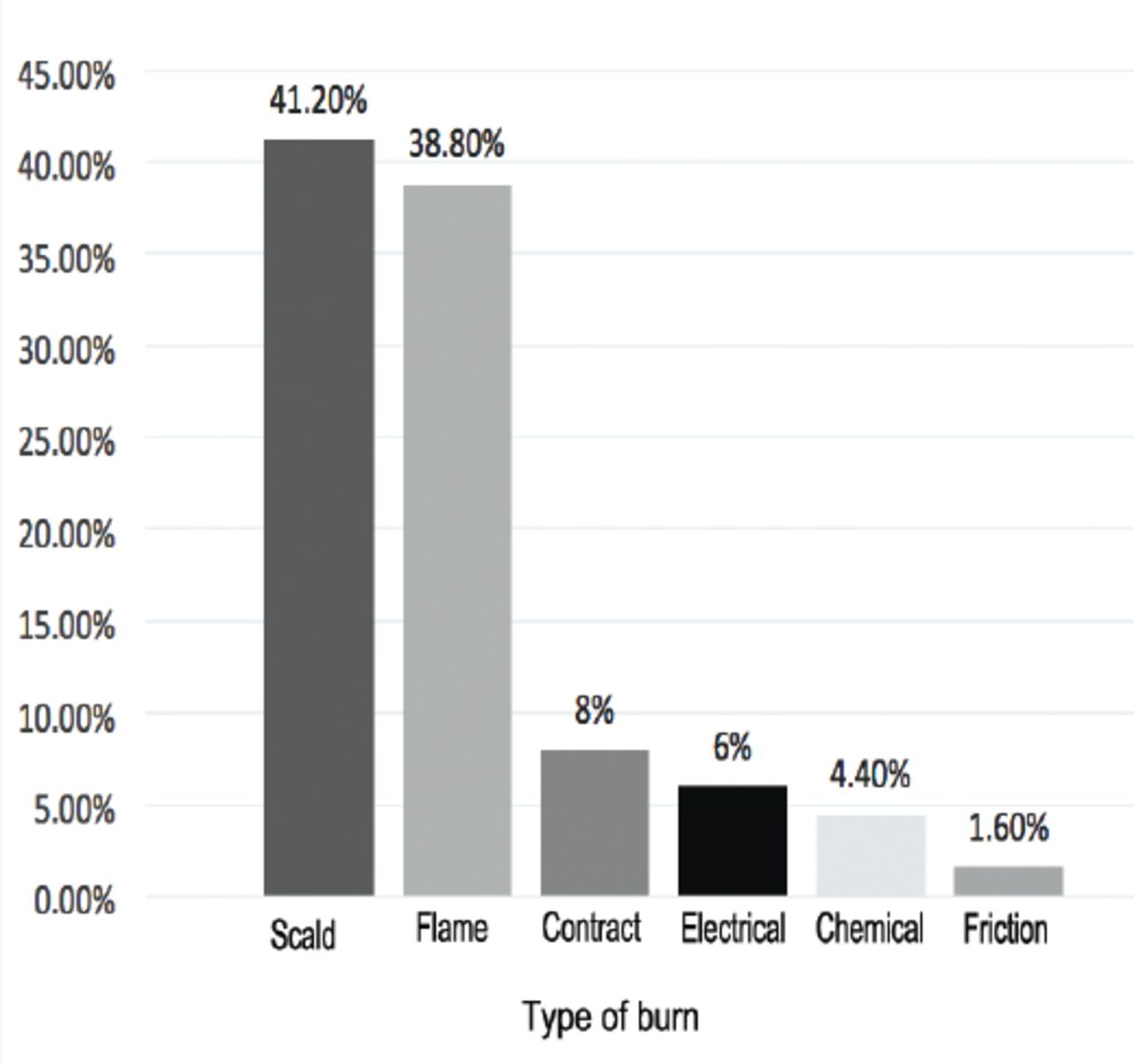
In total, 250 burn patients were included. A description of patients’ demographics can be seen in Table 1. The majority of patients were males (171; 68.4%) and pediatric (134; 53.6%). The mean age was 19.79 years. The majority of burns were scald burns in the pediatrics age group (85; 63.4%), which is statistically significant when compared to the adult age group (p<0.001). In the adult age group, flame burns were the most common (n=70; 60.3%) (p<0.001.) Overall, scald burns were the most common (n=103; 41.2%), followed by flame burns (n=79; 38.8%).
Demographic characteristics of all burn patients who were admitted and treated at Al-Noor Specialist Hospital, Riyadh, Saudi Arabia between January 2016 and January 2017 (N=250).
Figure 1 summarized the overview of burns type. The mean total burned body surface area (TBSA) was 16.5% (SD 19.98), while the mean length of hospital stay was 16.18 days (SD 16.71). A TBSA burn of ≥40% was more common in adults (19.4%) compared to pediatrics (4.1%) (p<0.001.).

Frequencies of different burn types.
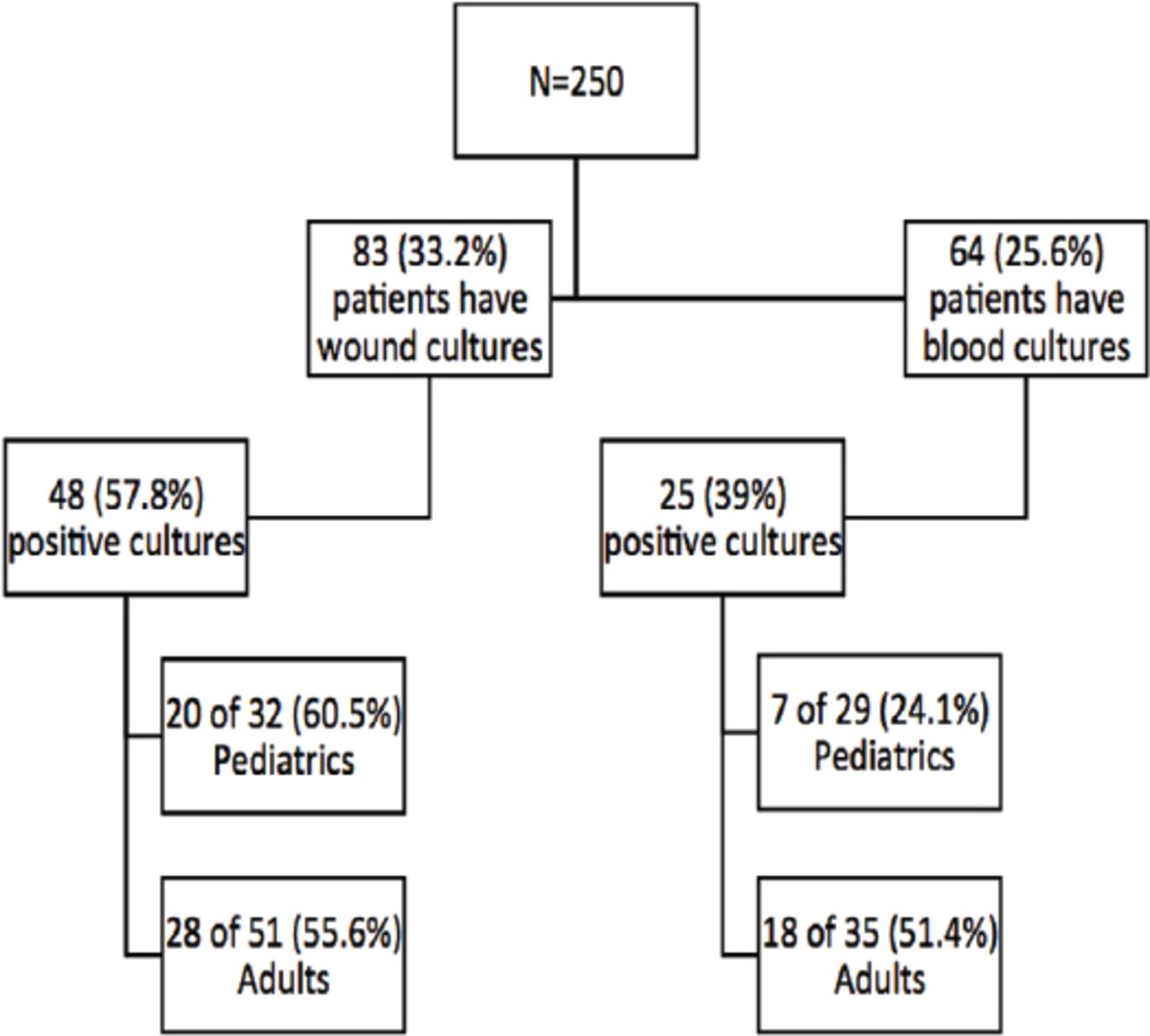
Blood cultures were drawn from 25.6% of our population, with only 39% being positive for infectious organisms. In addition, 33.2% of burn wounds were cultured with 57.8% returning positive for infection. For blood cultures, the majority were positive in adults (51.4%), whereas only 24.2% were positive in the pediatric age group. As for burn wound cultures, 55.6% were positive in adults and 60.5% were positive in pediatrics (Figure 2).
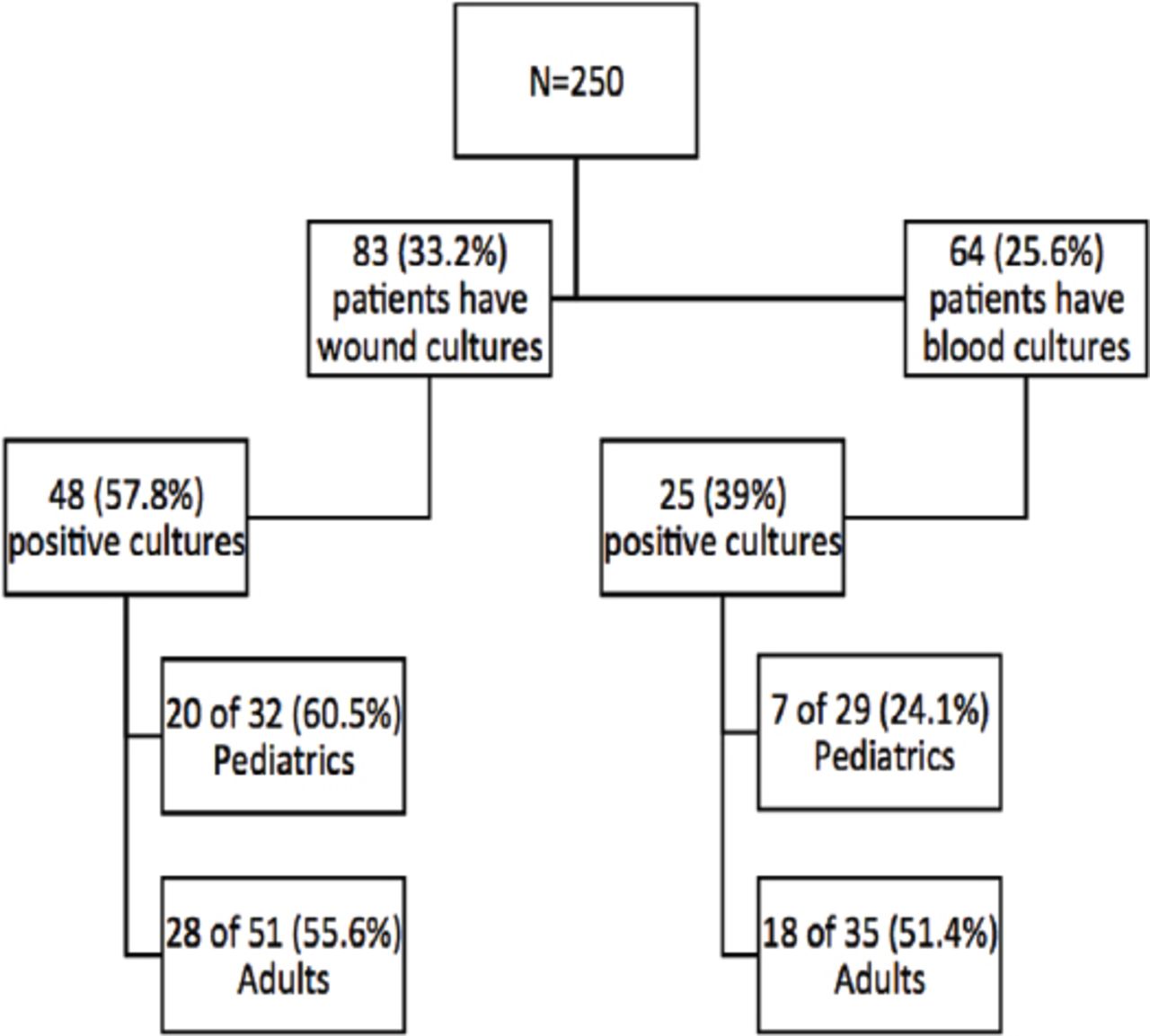
Frequency of cultures.
Blood and wound cultures in pediatrics were 100% positive when TBSA was ≥40%. A TBSA of ≥40% predicted a positive blood culture in both the adult (p<0.041) and pediatric population, (p<0.025). On the other hand, it could not predict a positive wound culture in either group (p<0.431 and p<0.486).
Table 2 highlights the organisms isolated from blood and wound cultures. The most common isolated organisms in blood cultures were MRSA and coagulase-negative Staphylococci (both 26.5%), followed by Klebsiella pneumoniae (17.7%). For burn wound cultures, the most common isolated organism was MRSA (36.4%), followed by Pseudomonas aeruginosa (22.7%). In patients with ≥40% TBSA burns, wound cultures showed Staphylococcus aureus (n=7; 33.3%) to be the most common organism, followed by Pseudomonas aeruginosa (n=5; 24%), Acinetobacter baummanii and Enterobacter cloacae (Figure 3).
Microorganism profile of wound and blood cultures.

Wound cultures based on total body surface area (TBSA).
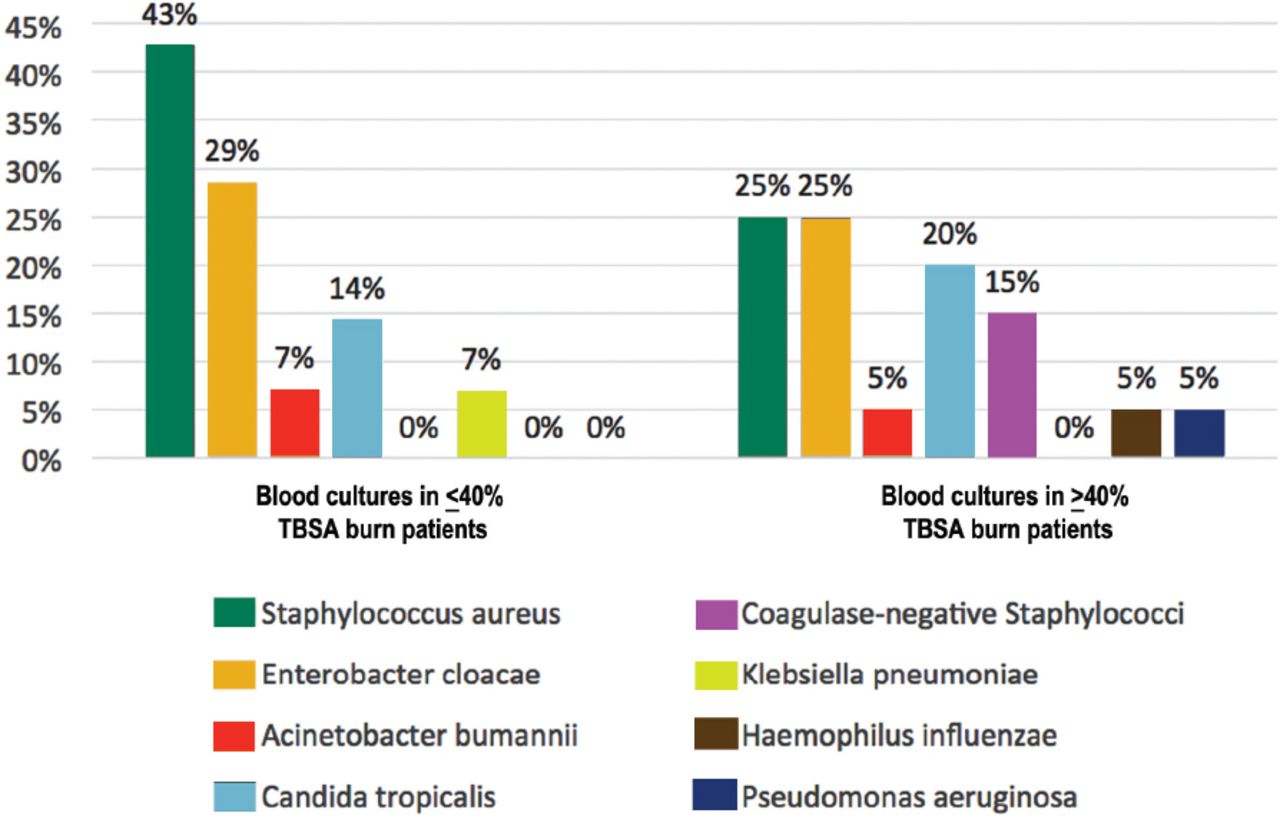
Acinetobacter baumannii was significantly more frequent in wounds in patients with ≥40% TBSA versus <40% (19% versus 2%) (p=0.005). Other organisms failed to show statistical significance. On the other hand, blood cultures in patients with >40% burn TBSA showed Staphylococcus aureus and coagulase negative Staphylococcus species to be the most common organisms (25%), followed by Klebsiella pneumoniae (20%), and Acinetobacter baumannii (15%) (Figure 4). In all cultures drawn, total MSSA was 6 (9.6%), with total MRSA being 33 (45.2%). Of all cultures positive for Staphylococcus aureus, MRSA was higher than MSSA (82.5% versus 17.5%). Positive blood cultures were polymicrobial in 16% and wound cultures were polymicrobial in 17% of the cases.

Blood cultures based on total body surface area (TBSA).
The student t-test was used to analyze the effect of positive cultures on length of stay. Patients with positive blood cultures had a significantly longer hospital stay (p<0.001) (95% CI: 12.72-33.47), as did patients with positive burn wound cultures (p=0.04) (95% CI: 0.97-19.58). In addition, the higher the TBSA the longer the hospital stay (p<0.001). Methicillin-resistant Staphylococcus aureus had no significant effect on length of hospital stay (p=0.71) (95% CI: -19.71-6.03), nor did MSSA (p=0.77) (95% CI: -15.87-25.58).
Discussion
Patients with serious burn injuries require immediate care in an exceedingly specialized burn unit to reduce morbidity and mortality. Although survival rates for burn patients have improved substantially within the past few decades because of advances in modern medical care in specialized burn centers, nosocomial infections still present a significant challenge for burn physicians treating burn patients and are known to cause over 50% of burn-related deaths.8 Burns to adult males occur mostly in outdoor or work settings, while burns to adult females occur mostly at home.13,14 In this study, more adult men (74.2%) than women (25.8%) suffered from burns. This may be due to the fact that men operate more machinery and drive cars while women did not at the time of the study. This is in concordance with a study by Al-Aali et al8 in which males represented 72.2% and females 27.7% of burn injuries. Results published by the WHO differ, showing women have slightly higher rates of burns than men.15
In the literature, the consensus is that burns remain more common in the pediatric age group than adults and our study concurs with this.16 Scald burns were the most common type of burns, followed by flame burns, contact burns, electrical burns, chemical burns and friction burns (Figure 1), slightly different in this study population than the East Mediterranean region.2 In this study, scald burns (63.4%) were the most common in the pediatric age group while flame burns (60.3%) were the most common type of burn in the adult age group. A European systematic review reported a similarly high rate of scald burns in pediatrics at 30-80%.4
Heggers et al17 mentions that burn wounds become infected due to the immunosuppressed state of the host and the wound environment, which are ideal for the proliferation of infecting organisms. Infections are a major source of mortality and morbidity in burn patients, with blood and burn wounds being common sources of infections.5 There is a directly proportional association between TBSA and positive cultures in both the pediatric and adult populations. Blood and wound culture rates were found to be higher when the TBSA was ≥40% and were positive more commonly in pediatrics (both 100%) than in adults (76.4%, 68.7% respectively). However, the percentages were lower when the TBSA was <40% with positive blood cultures in adults being 38.8% and 11.11% in pediatrics. The most common organisms isolated from burn wounds were MRSA (36.4%) followed by Pseudomonas aeruginosa (22.7%) (Table 2). Other studies also showed a high prevalence of Staphylococcus (27.6% and 20%, respectively) and Pseudomonas aeruginosa (12.3% and 39.5%, respectively) isolated from burn wounds.5,8 The most common organisms isolated from blood cultures were MRSA (26.5%), coagulase-negative Staphylococci (26.5%) and Klebsiella pneumoniae (17.7%) (Table 2). Reports from Bahemia et al8 also showed a high prevalence of Staphylococcus and Gram-negative bacteria in blood cultures. In severe burn patients with TBSA ≥40%, the most common isolated bacteria from burn wounds were Staphylococcus aureus (33%), Psuedomonas aeruginosa (24%), Acinetobacter baumannii and Enterobacter cloacae (each 19%) (Figure 3). Burn ICU patients have the same predominance of Gram-negative bacteria.5
The emergence of drug-resistant Gram-positive bacteria is a global crisis. The prevalence of MRSA infections worldwide is 13%-74%.18 A study of the prevalence of MRSA in the Gulf Corporation Council Countries (GCC), also showed that Saudi Arabia reported the highest rate of MRSA (39%) and the lowest rate was reported in Kuwait (3.3%).19,20 This study supports the previous study and reports a high rate of MRSA (82.5%). Of all cultures positive for Staphylococcus aureus, MRSA was more common than MSSA (82.5% versus 17.5%). Methicillin-resistant Staphylococcus aureus frequency in burn infections was 98% of all Staphylococcus aureus- infected patients in the burn ICU, while the frequency decreased to 67% in the regular burn unit patients which is comparable to the results of our study.5 Such high levels can be due to administering antibiotics after clinical decisions only, without further diagnostic investigations or general abuse of antibiotics.19 Similar to other literature reports, MRSA did not affect the length of hospital stay.10 There is a recent study that mentions reducing the use of fluoroquinolones and third generation cephalosporins (which have been associated with an increased rate of MRSA) as a potentially useful control measure in patient populations where MRSA is prevalent.21 Similarly, a case-control study carried out in the United Kingdom stated that the higher the number of antimicrobial agents used, the higher the risk for MRSA with fluoroquinolones having the highest risk.22
Study limitations
This study was limited by 2 points which must be noted. First, data was collected over one year only (2016). Second, cultures data were restricted to blood and burn wound cultures, since they are the most frequently taken, and no data on antibiotics usage was recorded. No data was collected on any use of invasive devices, as it was not the scope of our study. However, the center we collected data from is the largest burn center in Saudi Arabia, and the sample represented all age groups.11
In conclusion, the pediatric population has an increased frequency of burn injuries which is an incentive for more focused educational prevention programs. Additionally, burn infections carry significant morbidity, and are associated with a longer hospital stay. Moreover, this study shows that MRSA rates are significantly high in burn infections, which can be attributed to the misuse of antibiotics. This should prompt better antibiotic stewardship and limit the use of fluoroquinolones and cephalosporins in particular as resistance has also shown to develop during therapy, especially in the pediatric age group.23,24 Minimizing the use of these antibiotics can reduce the rate of MRSA infection.25 More effective prevention of transmission by enforcing strict contact precautions is also useful. This data can be helpful to implement local and national programs aimed at the prevention of MRSA infection.
Acknowledgment
The authors wish to acknowledge Yousef B. Abalkhail and Assal K. Al Amoudi for their contributions to this study, and PageCure (pagecure.com) for editing the language of the paper.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 7, 2020.
- Accepted May 30, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.