


Abstract
Objectives: To assess community pharmacists’ knowledge and practices regarding screening risk factors and providing safety information about the use of non-steroidal anti-inflammatory drugs (NSAIDs) to patients.
Methods: Cross-sectional and a self-administered questionnaire-based study was conducted over a 4-month period (May-August 2019) with selected community pharmacies in Jeddah, Saudi Arabia. The questionnaire composed of demographic data and the pharmacist’s role in supplying NSAIDs.
Results: The majority of participating community pharmacists dispense NSAIDs. However, many did not apply relevantly good communication skills such as seeking information about concomitant drugs (42.5%) or providing advice on managing any adverse side effects of taking NSAIDs (39.1%). Most of the community pharmacists also did not provide relevantly good communication about risk factors. The most common screening risk factors mentioned were a history of pregnancy and breastfeeding (84.2%) followed by being at an older age (74.5%) or a history of a gastrointestinal ulcer (71.5%).
Conclusion: Community pharmacists in Saudi Arabia need to appropriately screen their patients for adverse drug reactions and effectively communicate the risks of using NSAIDs. The Saudi Regulatory Authority could endorse several approaches to apply a good strategy for improving the dispensing practices in community pharmacies, communication and awareness of risk factors especially in high-risk patients who are taking NSAIDs.
- non-steroidal anti-inflammatory drugs
- NSAIDs
- community pharmacists
- counseling practice
- adverse drug reactions
Analgesics, such as non-steroidal anti-inflammatory drugs (NSAIDs) and acetaminophen (APAP), are the most common over-the-counter (OTC) drugs in the world used to treat fever, pain, and decrease inflammation.1,2 Non-steroidal anti-inflammatory drugs act by blocking the cyclo-oxygenase (COX) enzyme, which causes direct inhibition of the biosynthesis of thromboxane and prostaglandins from arachidonic acid. They are used for treating mild-to-moderate pain that arises from a variety of conditions such as osteoarthritis, rheumatoid arthritis, menstruation, headaches, or toothaches.
In Saudi Arabia, analgesics were one of the top 10 most used drugs between 2010 and 2015 and the NSAIDs class represented 67% of use.3 Many studies in Saudi Arabia found that the majority of people use the NSAIDs ibuprofen and diclofenac to treat headaches, colds, cramps, and fever.2,4 As well as, a recent study in Saudi Arabia (2019) found that around one-half of the participants in the study practised self-medication with these drugs primarily for pain management.5
Non-steroidal anti-inflammatory drugs are classified according to their preference for specific enzymes (example, COX-1 or COX-2). The non-selective NSAIDs like aspirin are more likely to cause adverse gastrointestinal (GI) effects while those that target COX-2 like celecoxib have a higher risk of negative cardiovascular effects.6 Although NSAIDs relieve pain, they can also cause severe side effects such as heartburn, stomach ulcers, and a tendency towards bleeding, liver or kidney problems, or high blood pressure.6
There are so many critical information that patients should know regarding the use of NSAIDs, such as they should not be taken around the time of any heart surgery. Non-steroidal anti-inflammatory drugs elevate the probability of developing an ulcer or internal bleeding in patients with a history of these issues. Advanced age, history of smoking, advanced liver disease, or chronic users of NSAIDs are more susceptible to these adverse effects. Pregnancy, asthma, and hypertension should be also taken into consideration before using NSAIDs.7
It has been reported that more than 16,500 people die annually from NSAID-related GI complications.8 Moreover, a recent study found that the most common drugs related to a need for hospital admission were NSAIDs.9 Non-steroidal anti-inflammatory drugs increased the possibility of developing adverse GI events 2.5 times.10 In addition, they can cause bronchospasms so patients with asthma may have more acute symptoms after taking NSAIDs. In addition, NSAIDs co-prescribed with corticosteroids increases bleeding risks 12-fold, which is more likely to be fatal.11 Moreover, patient knowledge and recognition of the risks of NSAIDs are inadequate and cause for concern. Many studies found that there is an overuse of NSAIDs medication among people and that the majority of them did not receive any counseling or information from health care providers about the appropriate use of NSAIDs.12,13
In Saudi Arabia, a great responsibility relies on pharmacists to improve the prescribing practice of NSAID medications. The community pharmacy is the main source for patients to seek pain relief, as NSAIDS may be dispensed without a prescription. A recent published article (2018) showed 24395 authorized pharmacists and pharmacy technicians in Saudi Arabia as of March 2017.14 They are distributed across the kingdom’s regions. The highest percentage in Riyadh region followed by Makkah region as 25% of registered pharmacist with the average age of 38 years.14 The community pharmacists represent the highest percentage (34.5%) across others pharmacy sectors. This study focus on assessing the self-reported practices regarding the performance of community pharmacists in NSAIDs dispensing, risk factors evaluation and offering appropriate advice and information about side effects and their management.
Methods
A cross-sectional study including community pharmacists was carried out in Jeddah, Saudi Arabia between May 2019 and August 2019. The study population included only pharmacists who are working in community pharmacies. There are 1182 pharmacies licensed by the Saudi Food and Drug Administration (Saudi FDA) in Jeddah, Saudi Arabia and this list was obtained from the annual statistical book from the Ministry of Health.15 Ethical approval for this study protocol was attained from the Ethics Committee for Human Research, King Abdulaziz University (PH-103-41).
We divided Jeddah, Saudi Arabia by using 5 geographical areas: north, south, west, east, and central. A convenient sample of pharmacies from different areas was selected. Pharmacy students visited pharmacies and asked the pharmacists about their willingness to participate in a study about the pharmacist’s role in supplying NSAIDs in community pharmacies. The questions in the survey were adapted from a previous study performed in Thailand.16 The questionnaire was divided into 2 parts: demographic data and the role of pharmacists in supplying NSAIDs. The second part consisted of 12 sections about the screening risk regarding adverse drug reactions (ADRs). and 8 advice on ADRs management: i) highlights the concomitant drug with NSAIDs, communicating and educating patients about potential side effects, ii) screening patients at risk factors, iii) and giving advices and information to patients using NSAIDs. Choices concerning to the prevalence of pharmacist profession in each question were recorded (as regularly, occasionally, or never). Ten pharmacists tried out this questionnaire and the content validity was subjected to a panel of pharmacist experts. The questionnaire was presented to 390 community pharmacists at their place of work. However, 190 of the community pharmacists either refused to participate in the study or forgot to return the survey back. Therefore, 200 of community pharmacists were willing to engage in the study and complete questionnaires that were included in the data analysis. The geographic breakdown of regions was northern 55, eastern 13, central 57, southern 43, and western 32.
Statistical analysis
Microsoft Excel was applied for the general data analysis and were analyzed by using the Statistical Package for Social Sciences, version 23 (IBM SPSS Inc, Chicago, IL, USA). Descriptive data were expressed as frequencies and percentages.
Results
The response rate was 51.3% since out of 390 distributed questionnaires, 200 were returned for evaluation. Most of the respondents were male (n=191, 95.5%) and were working in a chain pharmacy. The majority of respondents were aged between 25 to 34 years old and had earned a Bachelor of Science (n=130, 65%) with more than 5 years of experience in a community pharmacy (n=142, 71%). Approximately 70% of the respondents scheduled in a 10-hour or shorter shifts where less than 2 pharmacist were working at a time (n=186, 93%), but more than 70% of them had an assistant present in the pharmacy as summarized in Table 1.
Characteristics of community pharmacist respondents.
The prevalence of self-reported practice roles by community pharmacists while supplying NSAIDs is shown in Table 2. The majority of the pharmacists declare to follow best practices regularly or occasionally in screening risk factors, dealing with adverse effects, as well as checking drug-drug and drug-herb interactions with NSAIDs. More than half of the pharmacists claimed that they screened for risk factors regularly while supplying both selective (54.88) and non-selective (51.9%) NSAIDs. Similarly, approximately 50% of the pharmacists pointed out their regularity in adverse effects notify as well as counseling on managing and protecting against side effects of selective NSAIDs in a similar manner to how they discussed non-selective NSAIDs.
The prevalence of self-reported practice roles by community pharmacists in supplying non-steroidal anti-inflammatory drugs (NSAIDs).
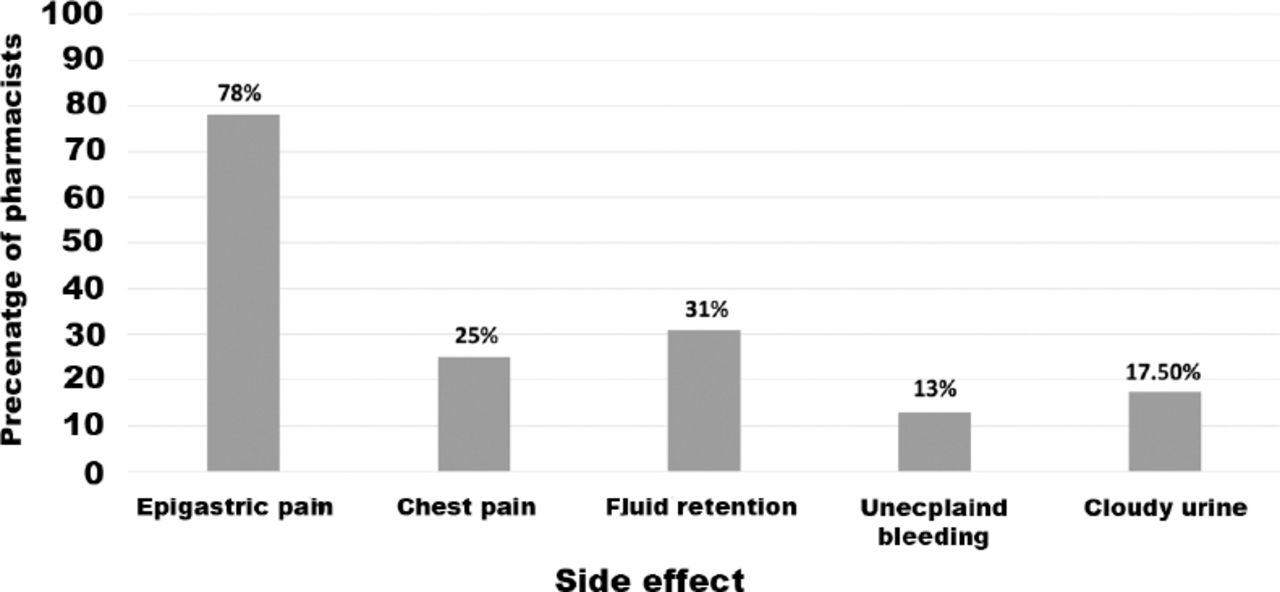
The popular side effects for NSAIDs as described by community pharmacists were epigastric pain, nausea, and vomiting (Figure 1). Therefore, Table 3 shows the descriptive data which focused on the most common frequently reported advice provides to reduce side effects from NSAIDs. The most mutual input to prevent GI complications was to use the drug after a meal; (n=173, 86.5%) for non-selective and selective NSAIDs (n=167, 83.5%). Almost half of the pharmacists pointed out they regularly guide patients to use gastro-protective agents (n=111, 55.5% for non-selective) (n=95, 47.5% for selective NSAIDs). In addition, many pharmacists also claimed that they explain when to stop taking NSAIDs (n=129, 64.5% for non-selective NSAIDs) (n=120, 60% for selective NSAIDs) and when dose reduction may be needed as well (n= 115, 57.5% for non-selective NSAIDs) (n=111, 55.5% for selective NSAIDs).

The major side effects that pharmacists included during NSAIDs: non-steroidal anti-inflammatory drugs counseling.
The most reported advices by community pharmacists on prevention against side effects from NSAIDs use.
The bivariate analysis shown in Table 4 revealed that pharmacists who have an assistant in the pharmacy were significantly more likely to counsel their patients about ADRs related to users of non-selective (odds ratio [OR] 2.966, 95% confidence intervals [CI] 1.462-6.016) and selective COX-2 NSAIDs (OR=2.142, 95% CI=1.058-4.336). In a similar manner, pharmacists with more experience (>5 years) were significantly more likely to counsel their patients about ADRs related to users of non-selective (OR: 2.629, 95%CI=1.232-5.613) and selective (OR=2.788, 95%CI=1.303-5.965) COX-2 NSAIDs. In addition, having another pharmacist working on the same shift significantly increased (4 times) the likelihood that the pharmacist would inform patients about ADRs linked with selective COX-2 NSAIDs uses (OR 4.330, 95% CI=1.980-9.471). However, there were no statistically significant differences for other factors such as age, education, or type of drug store, which influenced the discussion of ADR linked to non-selective and selective COX-2 NSAIDs users.
Factors related with frequency of side effects information provision to patients of non-selective and selective NSAIDs.
Regarding risk factors screening, the majority of the community pharmacists stated that this was performed occasionally when dispensing NSAIDs. The majority of risk factors that pharmacists discussed with patients for non-selective NSAIDs were pregnancy and breastfeeding (n=168, 84%) followed by their age (n=149, 74.5%) and history of GI ulcers (n=143, 71.5%) or bleeding. A similar observation regarding the majority of risk factors was found for selective NSAIDs (Table 5).
Frequency of non-selective and selective NSAID risk factor screening by community pharmacists.
Discussion
This study in Saudi Arabia to aims to evaluate the awareness and profession by community pharmacists with their patients regarding the use of NSAIDs. In Saudi Arabia, there is an easy access to NSAIDs in the community pharmacies. Thus, it takes a great effort by the pharmacist to ensure appropriate awareness about these drugs before dispensing them. However, patients received limited safety information about appropriate monitoring and preventing side effects regarding their NSAIDs medicines from healthcare providers.17
Many studies have been conducted worldwide to evaluate public knowledge and attitude regarding the use of over-the-counter (OTC) medications and particularly NSAIDs. These studies revealed inadequate patient knowledge about side effects which require more advice and consultation regarding appropriate management or prevention tips to mitigate the risks of NSAIDs.2,13,18-22 A study conducted in Jeddah, Saudi Arabia among NSAIDs users found that approximately 75% of them were not counselled by a healthcare provider on the risks of NSAIDs and more than 90% of them were united in the opinion that greater efforts are needed from healthcare providers in presenting information regarding ADRs.2,13,18-21 Receiving information about NSAIDs in any way other than from the authorized person may lead to inaccurate and nonspecific information. In addition, the material in the medication leaflets is not suitable for the public. Therefore, only a few patients are able to comprehend the content. Evaluation of medication inserts in Saudi Arabia reports there is a shortage of information in comparison with comparable information in the United States.18,20,23,24 Health care providers and pharmacists are a valuable source of accurate information that increases their responsibility and role as medication experts. Pharmacists should be aware of the most risk factors while dispensing NSAIDs and able to screen and monitor patients at risks to reduce NSAIDs complications.18,20,23
Regardless of the differences in patient responses and preferences, adverse effects caused by NSAIDs use have been observed and more evaluation about patients’ knowledge concerning these risks is needed. The most popular adverse effects were GI side effects, which could be aggravated by age, peptic ulcer history, and multiple doses of NSAIDs. Selective NSAIDs superior the traditional NSAIDs in regard to side effects particularly GI tract side effects. Renal, hepatic, cardiovascular, and haematologic side effects have also been commonly reported with the use of NSAIDs.25
The majority of community pharmacists claimed to review patient risk factors and provide advice about the management of side effects but others indicated they did not do this for all patients. These results were consistent with a study by Babelghaith et al13 which indicated that more than 30% of the participants receive insufficient information about possible side effects from NSAIDs. However, our results cannot be generalized as we did not differentiate between the counseling or requested information from patients. Another study about counseling practice conducted in Riyadh, Saudi Arabia showed a 40% improvement in the rate of counseling due to requested information from the patients.22 It is probable that the percentage of pharmacists who delivered best practice in counseling and screening their patients may be overestimated. At the same time, previous research supports the concept that by reporting the current defect in good dispensing practices and medication counseling regarding ADRs will improve the management of adverse effects by community pharmacies in Saudi Arabia.13,23,26,27 Interetingly, pharmacists with more experience (>5 years) as well as who have an assistant in the pharmacy significantly more likely to inform their patients on ADRs which shows successfulness in improving the quality of drug dispensing. Having more experience gives pharmacists a level of professional confidence and knowledge to be proactive in providing advice to their patients. Also, having an assistant provides more time for pharmacists to interact with patients and provides high quality patient care.
The main risk factors for NSAIDs ADRs as reported were for pregnancy and breast-feeding, older age, and history of GI bleeding. Many studies indicated that patients should be screened for the existence of GI and cardiovascular side effects before using NSAIDs, and should undergo GI-prevention therapy when risk could be an issue.28-31 In Europe, the majority of the patient using NSAIDs with one or more risk factors for GI complications received poor prevention treatments.25 Using NSAIDs regardless of COX selectivity and duration of use would increase the risk of side effects of cardiovascular and bleeding complications.32 Age is considered to be a significant risk factor for NSAIDs-related GI complications and appropriate management strategies should be applied in the elderly.33
Many studies have indicated that selective COX-2 inhibitors cause critical adverse cardiovascular effects including myocardial infarction, cerebrovascular accidents and heart failure.34,35 Thus, appropriate knowledge and awareness of the risks of adverse effects could contribute to a patient’s decision to take NSAIDS or not.36 However, it is a pharmacist’s role to improve prescribing practice by striking a balance between providing information to them while at the same time allaying worries that may affect their management plan.
Although this study showed some positive observation from pharmacists regarding good qualities associated with dispensing NSAIDs, it was found that community pharmacies still need to apply good comprehensive services in relation to dispensing these widely used medications that could result in serious ADRs.
During the current COVID-19 epidemic, there is an intense need for the public to be educated and consulted about the proper use of NSAIDs after an alarming finding that suggested a detrimental effect of NSAIDs used in patients with COVID-19.37 The FDA responded to those reports and suggested NSAIDs may worsen COVID-19 cases without any clear scientific evidence.38 Professional health care providers, especially community pharmacists, should enhance consciousness of NSAIDs risks between consumers, proper counseling and evaluate potential risk factors as well as assort safety notification to assure safe and suitable use of these drugs.13,16,22,39-42
Study limitation
This study is using a cross sectional survey of community pharmacist to evaluate the NSAIDs prescribing practice. Simulated patient method could be a robust method for assessing prescribing practice and result in more accurate assessments.22
In conclusion, the study highlights the current insufficiencies in medication counseling and proper practices at community pharmacies in Saudi Arabia. Appropriate patient counseling and conscious dispensing of medications are needed to minimize adverse effects associated with self-medication. Community pharmacists in Saudi Arabia need to appropriately screen their patients for the risks of NSAIDs complications and effectively communicate accordingly. The Saudi regulatory authority could endorse several approaches to apply a good strategy for improving the dispensing practices in community pharmacies, communication and awareness of risk factors especially in high-risk patients who are taking NSAIDs. Then, intensive research will be required in the coming years to monitor the implementation. More studies are required to evaluate the prevalence of counseling and advice among community pharmacies in other cities in Saudi Arabia. Future studies that apply simulated visits to community pharmacies are also needed to observe the actual counseling practice for robust findings and results.
Acknowledgment
The authors gratefully acknowledge Cambridge (www.cambridgeproofreading.org) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 2, 2020.
- Accepted July 12, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.