


Clinical Presentation
A 48-year-old Bangladeshi male with no past relevant medical, surgical, family, or psychosocial history, was brought in by the Red Crescent and presented to the King Saud Medical City, Riyadh, Kingdom of Saudi Arabia, Emergency Department after involvement in a high-speed motor vehicle crash as an unrestrained passenger.
On arrival, his airway was intact; a cervical collar supported his neck. His breathing was spontaneous on room air, with decreased air entry on the right side of the chest. His respiratory rate was 24 breaths/min, and oxygen saturation was 92% on room air. Circulation-wise, his heart rate was 112 bpm, with blood pressure of 105/65 mmHg and cooler peripheries. Disability-wise, he was confused and agitated, with a glasgow coma scale (GCS) of 14/15, and his pupils were equal, 2 mm, and reactive to light. On exposure, there was biparietal scalp swelling, no external bleeding, a tender right upper quadrant of the abdomen, a stable pelvis, and no abnormality found in the extremities. On log rolling, there was no spine tenderness, and the rectal digital examination was unremarkable. After an initial assessment, the patient was managed as per ATLS® guidelines. Chest radiography showed a right-sided hemothorax (Figure 1).
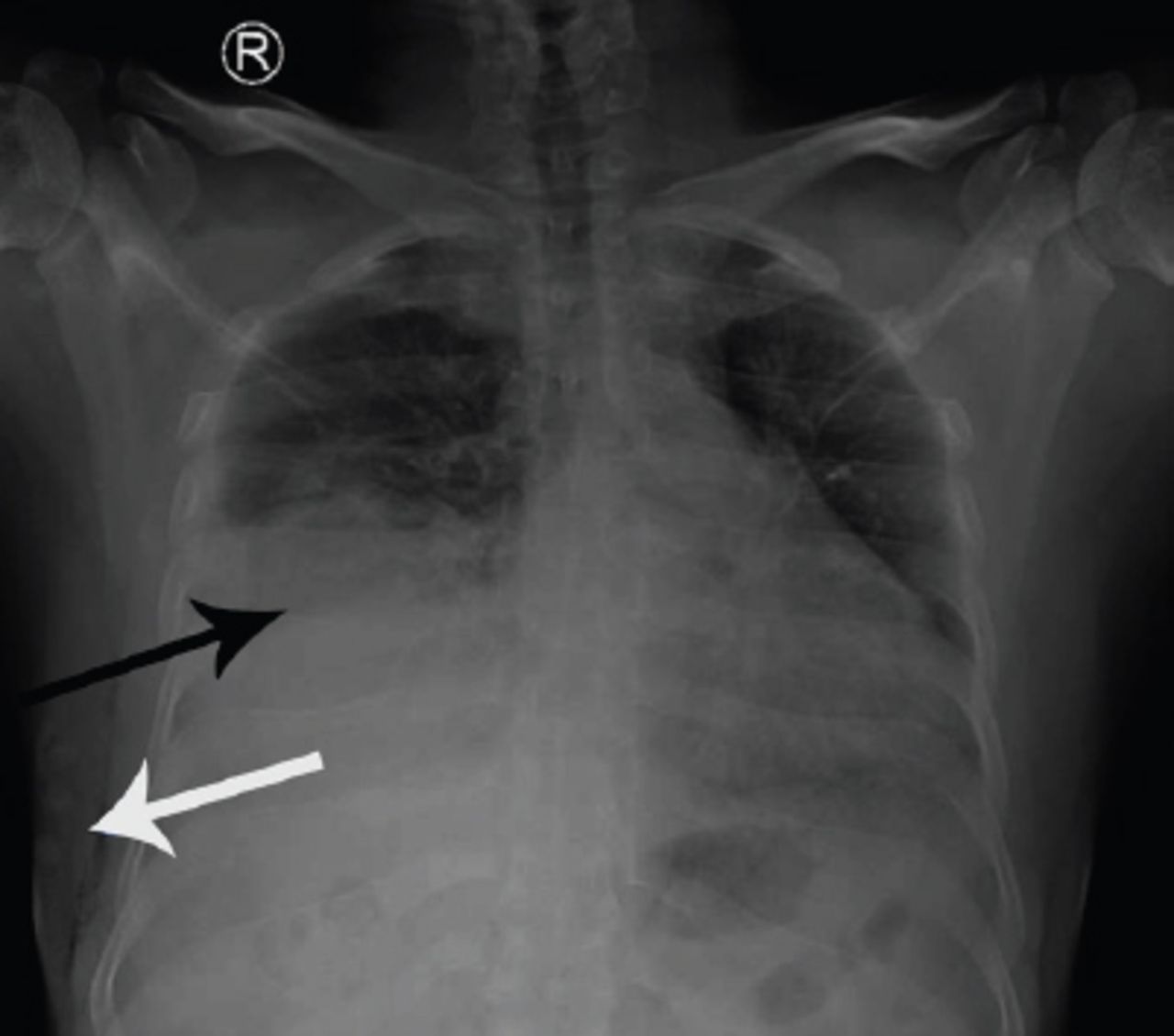
Chest radiograph during the primary survey.
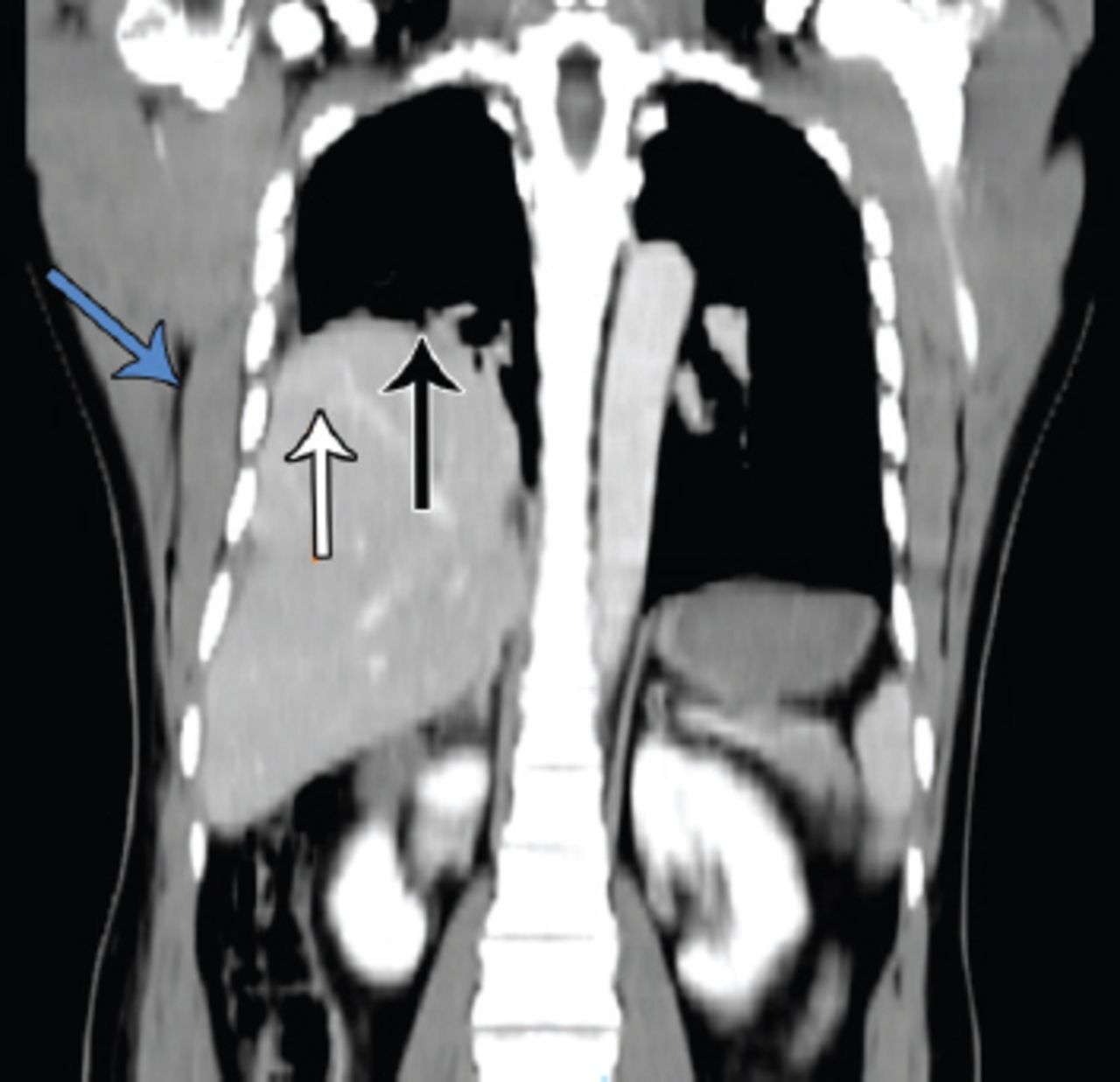
We inserted a right-sided chest tube (Figure 2), which initially drained approximately 700 ml of blood. The patient became more agitated, and his GCS was dropping, so we immediately established a definitive airway by intubation. Focused assessment sonography for trauma showed fluid in the right hepatorenal space and the pelvis. Two units of packed red blood cells were transfused, as his hemoglobin dropped to 8.0 gm/dl. Once the patient was hemodynamically stable, we obtained pan computed tomography (CT). The brain and neck CT showed a biparietal subgaleal hematoma, otherwise unremarkable. A chest CT revealed right-sided hemopneumothorax, first and twelfth rib fractures, lung contusion, and possible right-sided diaphragmatic eventration with an elevation of the right lobe of the liver (Figure 3).

Chest radiograph after insertion of the right intercostal tube.

CT chest and abdomen (coronal view).
Abdomen and pelvis CT showed a laceration, 3 cm in depth, involving segment VII of the liver, with associated parenchymal and subcapsular hematoma, suggesting grade 3 liver trauma injury with mild hemoperitoneum. We admitted the patient to the intensive care unit (ICU) and managed him conservatively. We successfully extubated him on the third day of admission and removed the chest tube on the fifth day. A follow-up chest and abdomen CT showed resolution of the right hemopneumothorax, a healing liver injury, and right diaphragmatic eventration, with no radiological evidence of a hernia. He refused to have a thoracoscopy for the definitive diagnosis of diaphragmatic eventration. Finally, we discharged him from the hospital on the eleventh day post-admission with no further complications.
Questions
Answers
The initial chest radiograph (Figure 1) shows right sided moderate to massive hemothorax (black arrow), and mild surgical emphysema (blue arrow). After the insertion of right intercostal drainage, the chest radiograph (Figure 2) shows an elevated right hemidiaphragm (black arrow), pneumothorax (orange arrow), and surgical emphysema (blue arrow) on the right side. The coronal view of chest and abdomen CT (Figure 3) shows right-sided diaphragmatic eventration (black arrow), an elevated liver (orange arrow), and mild surgical emphysema (blue arrow) on the right side.
According to the history, physical examination, and radiological investigations, the possible diagnosis is right-sided hemothorax, lung contusion, elevated right hemidiaphragm due to subpulmonic effusion, diaphragmatic eventration, phrenic nerve injury, or even diaphragmatic rupture.
During insertion of the intercostal tube, special care should be taken to avoid lung, diaphragm, or liver injury. After skin incision, one needs a careful dissection of subcutaneous tissue and thoracic and intercostal muscles. It is better not to use a metallic trocar during the introduction of the tube.
Discussion
Diaphragmatic eventration is as an abnormal elevation of the hemidiaphragm or part of it, accompanied by that of the abdominal structures beneath, without losing its continuity. This makes it different from a diaphragmatic hernia. It is a rare condition with an incidence of less than 0.05%, first described in an autopsy case by Louis Petit in 1774.1 It is much more common in the pediatric population than in adults, since congenital anomaly is a primary etiology of this condition. It is mainly asymptomatic, and the most common symptom is dyspnea, if present. Eventration can be complete or partial or left- or right-sided, but bilateral eventration is extremely rare.2-4
The diagnosis of a rare condition such as diaphragmatic eventration following a motor vehicle crash may be challenging for a physician dealing with a thoracoabdominal trauma situation. The chest radiograph may show an elevated hemidiaphragm. The radiographic diagnosis should be made by exclusion, since other conditions may resemble diaphragmatic eventration on a plane film.1,4 Acquiring an elevated hemidiaphragm may occur due to a phrenic nerve injury from a previous trauma or post-surgery. Chest trauma causing hemothorax, lung contusion, subpulmonic collection, or diaphragmatic rupture may also mimic the situation. Multiplanar CT can diagnose the condition accurately, although some authorities suggest thoracoscopy or laparoscopy as a gold standard.5 Fluoroscopy and a sniff test may be considered to diagnose diaphragmatic paralysis, and real-time ultrasonography may be useful in determining partial eventration and differentiating it from diaphragmatic nerve interruption.4
If the patient is unstable and goes to the theater for hemorrhage control, the surgeon may attempt plication of the diaphragm if the situation allows, but in a damage control situation, the surgeon can defer the procedure. Asymptomatic and incidentally diagnosed eventrations do not require surgical intervention, and conservative management is the treatment of choice.
Any significant chest or abdominal trauma may cause devastating consequences in the presence of eventration, including rupture of the diaphragm. During pleural decompression by tube thoracostomy as a part of resuscitation, one needs to take special care to avoid injury to the thoracoabdominal organ.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
Notice: Authors are encouraged to submit quizzes for possible publication in the Journal. These may be in any specialty, and should approximately follow the format used here (maximum of 2 figures). Please address any submissions to: Editor, Saudi Medical Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. Tel. +966 (11) 4777714 Ext. 42841.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.