


Abstract
Objectives: To evaluate the efficacy and safety of carboplatin-based preoperative chemotherapy in triple-negative breast cancer patients (TNBC).
Methods: PubMed, EMBASE, the Web of Science, the Cochrane Library, major clinical trial registries, and abstract collections from major international meetings were systematically searched for relevant randomized controlled trials. Endpoints included rates of pathologic complete response (pCR), overall response (ORR), breast-conserving surgery (BCS) and toxicity. Pooled relative risk (RR) was calculated for each endpoint using a fixed- or random-effect model depending on the heterogeneity among included studies.
Results: A total of 5 randomized controlled trials involving 1007 patients were included in the meta-analysis. Carboplatin-based chemotherapy was associated with a pooled pCR rate of 53.3%, which was significantly higher than the rate associated with non-carboplatin therapy (37.8%, RR: 1.41, 95% confidence interval [CI]: 1.23 to 1.62, p<0.00001). Compared with non-carboplatin therapy (48.1%), carboplatin-based chemotherapy increased BCS rate (59.7%, RR: 1.24, 95% CI: 1.06 to 1.46, p=0.007). Carboplatin-based chemotherapy was associated with similar ORR as non-carboplatin therapy. Carboplatin-based chemotherapy was associated with higher incidence of grade 3 or 4 anemia, neutropenia, febrile neutropenia, and thrombocytopenia than non-carboplatin therapy, while the 2 regimens were associated with similar incidence of fatigue, leucopenia, and nausea/vomiting.
Conclusion: The available evidence suggests that carboplatin-based preoperative chemotherapy is associated with significantly better pCR and BCS rates than non-carboplatin-based therapy in TNBC patients.
Breast cancer is the most frequently diagnosed cancer and the leading cause of cancer death in females worldwide.1 Triple-negative breast cancer (TNBC), a subtype of breast cancer accounting for 10-20% of all breast cancers,2-11 is characterized by absence of expression of estrogen, progesterone receptor, and human epidermal growth factor receptor 2 (HER2). The TNBC occurs predominantly in young people and is associated with higher rates of metastasis and mortality than other subtypes of breast cancer.2-5 It seems that women with TNBC do not benefit from targeted therapy or endocrine therapy. Preoperative chemotherapy, an important part of an integrated treatment approach, is increasingly used in patients with locally advanced breast cancer. Preoperative chemotherapy has been found to reduce cancer volume, improve the surgical resection rate, reduce the tumor stage, and increase the possibility of breast-conserving surgery.12 It also allows in vivo assessment of patient sensitivity to chemotherapy.13 Studies suggest that preoperative chemotherapy for breast cancer provides survival benefits comparable with those of postoperative chemotherapy, and that it is associated with significantly higher rates of overall survival (OS) in patients achieving pathologic complete response (pCR).14 Specifically among patients with TNBC who experience pCR, preoperative chemotherapy is improved 26% of 3-years OS rate.15 Maximizing the rate of pCR is widely considered the most important outcome for preoperative chemotherapy against TNBC. The 48-70% of breast cancer patients with BRCA1 mutations are TNBC.16-18 The tumor with BRCA1 mutations may suffer from defects in DNA repair pathways. Thus, platinum-based chemotherapy, although usually a second-line treatment in breast cancer, may be an effective first-line approach in TNBC. Carboplatin is preferable to cisplatin because it shows comparable antitumor activity to cisplatin but with fewer adverse effects. It is unclear on whether carboplatin-based preoperative chemotherapy is effective and safe for patients with TNBC. A small trial in Spain showed that adding carboplatin to preoperative chemotherapy did not improve pCR in patients with basal-like breast cancer,19 whereas 2 studies in USA and Germany showed that adding the drug to preoperative chemotherapy improved the pCR of patients with TN BC.20,21 Thus, we performed this meta-analysis of available randomized controlled trials.
Methods
Search strategy and study inclusion
We systematically searched PubMed, the Web of Science, EMBASE, and the Cochrane Library for randomized controlled trials published between January 2000-2015 that examined the effectiveness of carboplatin in preoperative chemotherapy against TNBC. Publications were screened initially on the basis of the title and abstract, and then on the basis of the full text.
We also searched major clinical trial registries (www.ClinicalTrials.gov, www.who.int/trialsearch) for relevant randomized controlled trials. The abstracts of annual meetings of the San Antonio Breast Cancer Symposium, American Society of Clinical Oncology and European Society for Medical Oncology were searched.
No language restrictions were applied during any searches. To be included in the meta-analysis, studies had to: 1) involve patients who had been diagnosed with TNBC based on pathology, who did not suffer any other diseases and who were undergoing their first treatment; 2) compare carboplatin-based and non-carboplatin preoperative chemotherapy; and 3) report sufficient outcomes data.
Two authors independently searched all potentially relevant publications. Discrepancies were resolved by discussion.
Data extraction
Two authors independently extracted data from the included studies using a standard form. The following data were extracted from each study: 1) basic characteristics, including authors, year of publication, and phase of the trial; 2) study characteristics, including number of subjects enrolled, patient ages, disease stages, and chemotherapy regimens; 3) outcomes of interest: pCR, overall response (ORR), and breast-conserving surgery (BCS); 4) types and incidence of grade 3 or 4 adverse events.
Assessment of study quality
The methodological quality of the included studies was assessed using Review Manager 5.3 (www.cochrane.org).
Statistical analysis
The primary endpoint was pCR rate, and secondary endpoints included ORR, rate of BCS, and rates of grade 3 or 4 adverse events. The ORR was defined as the sum of partial and complete response rates according to the guidelines for response evaluation criteria in solid tumors.22 Adverse events were evaluated according to the National Cancer Institute Common Terminology Criteria for Adverse Events 3.0 or 4.0.
Relative risk (RR) and associated 95% confidence intervals (CI) were estimated for data using the Mantel-Haenszel fixed-effect model or the Der Simonian-Laird random-effect model. The fixed-effect model was used when significant heterogeneity was absent across the pooled studies; significant heterogeneity was considered to exist when the Q test gave an associated p-value <0.05 and I2 was >60%. Otherwise, the random-effect model was used.
All statistical analyses were performed using Review Manager 5.3. All p-values were calculated for a 2-tailed distribution.
Results
Characteristics of included studies
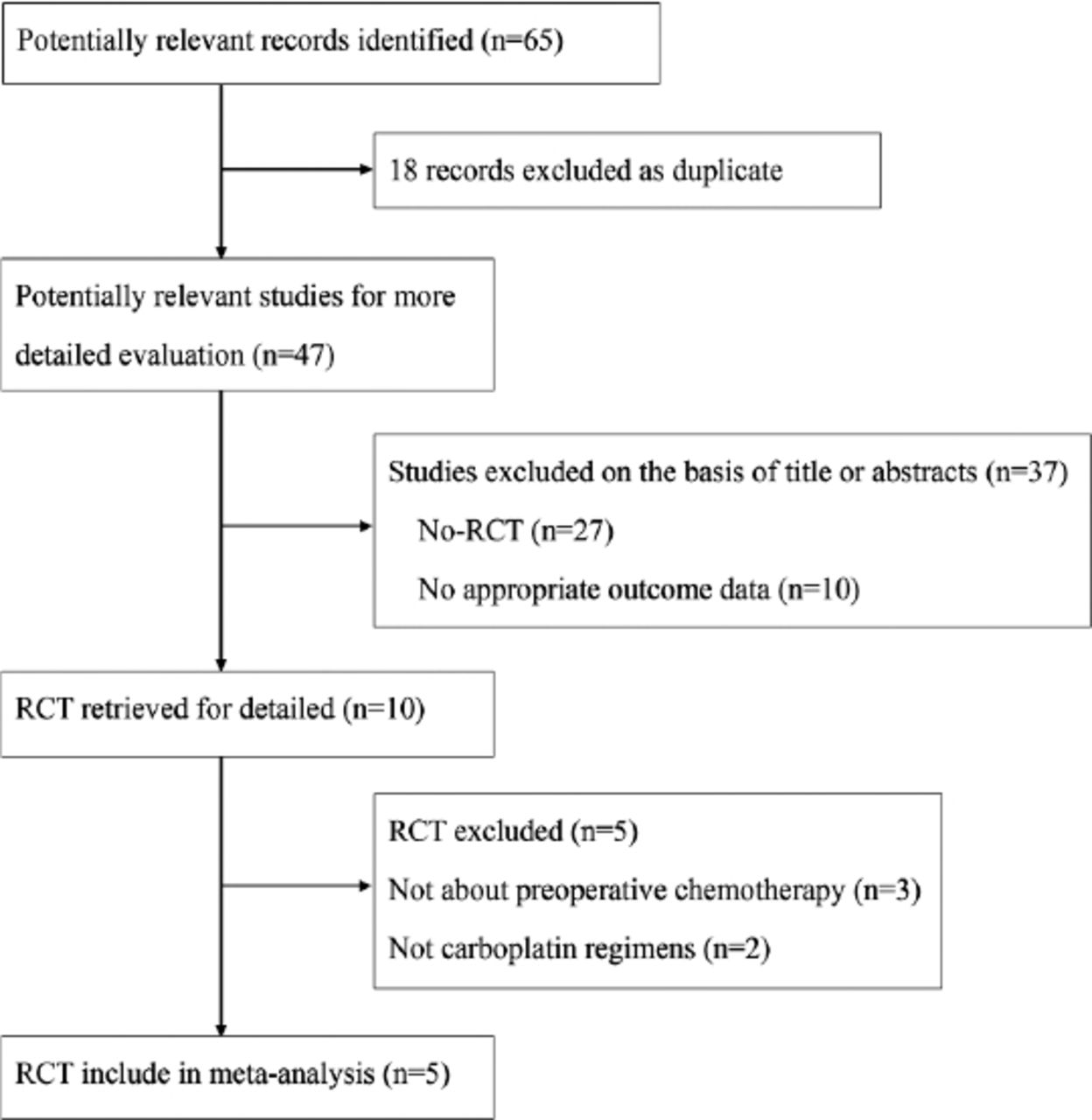
A total of 65 potentially eligible trials were screened. Finally, 5 independent trials, involving altogether 1007 patients, were included in the meta-analysis19-21,23,24 (Figure 1, Table 1). The 5 randomized controlled trials included between 91 and 595 TNBC patients in stages I-III; 3 trials involved Caucasians, and the other 2 involved Asians. All 5 studies examined preoperative chemotherapy comprising a combination of carboplatin with another taxane chemotherapeutic, including paclitaxel and docetaxel. We evaluated the quality of 4 publications with full-text. All 4 studies completely described the randomization procedure, adequate allocation concealment, and complete results.
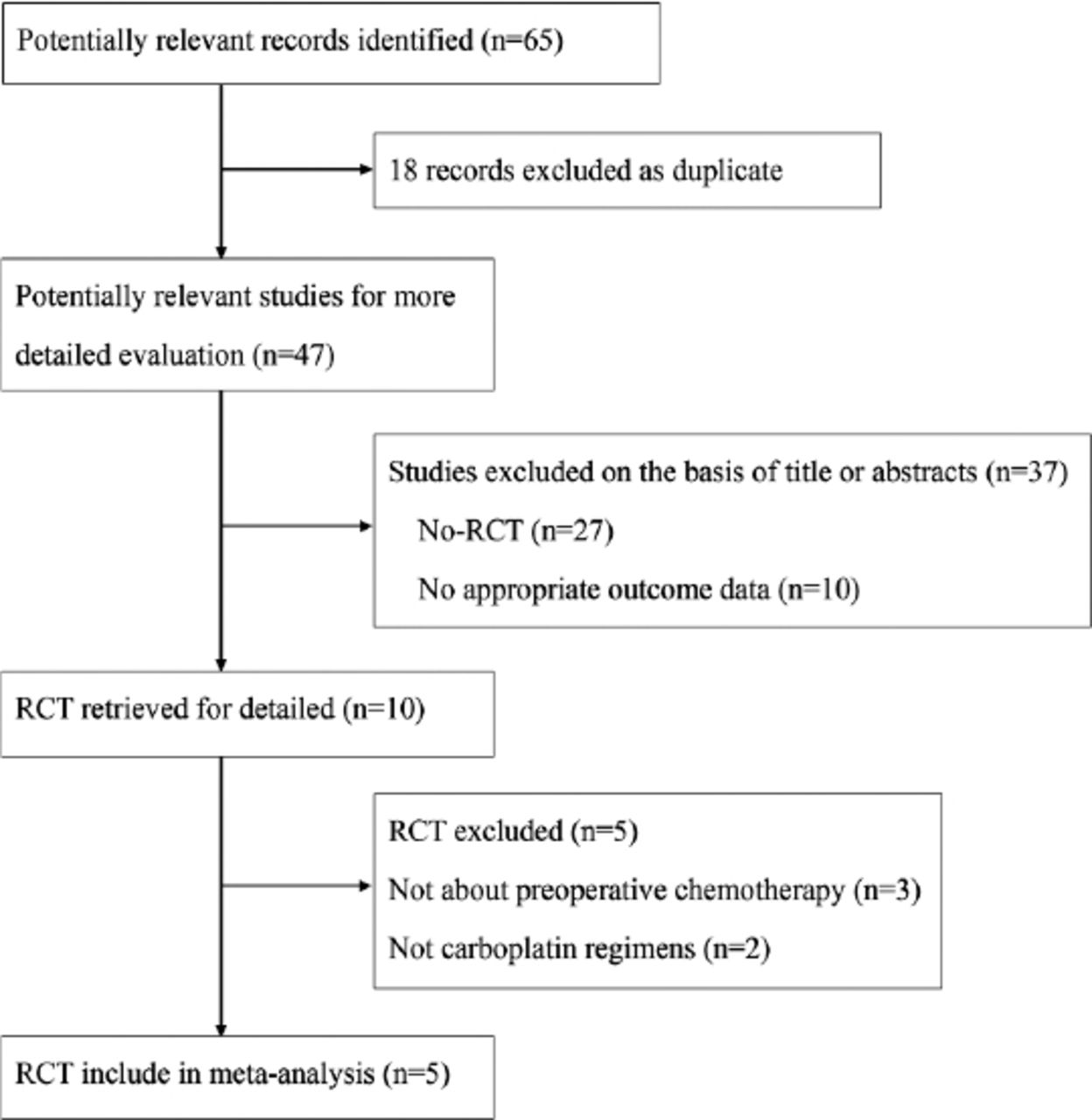
Flow chart diagram of study selection. RCT - randomized controlled trials
Characteristics of randomized controlled trials in the meta-analysis.
Pathologic complete response
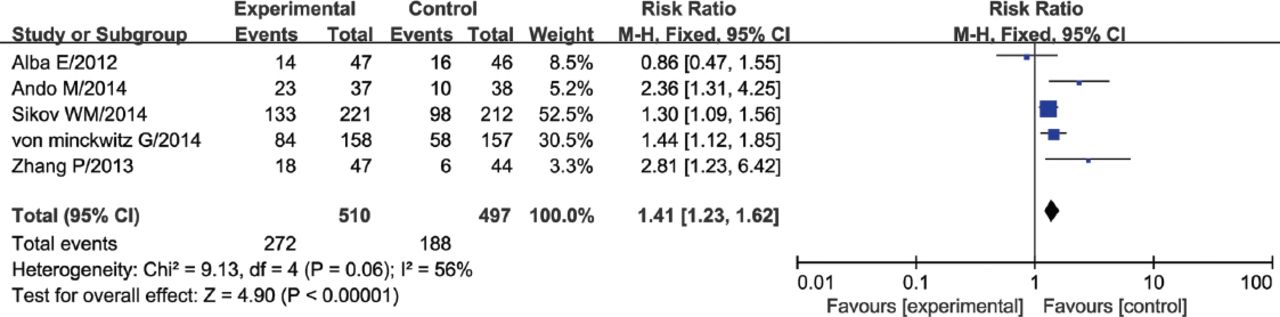
All 5 trials described data on pCR. The absolute pCR rate was 53.3% (272/510) in patients receiving carboplatin-based therapy and 37.8% (188/497) in patients receiving non-carboplatin therapy. No significant heterogeneity in pCR rate data was detected among studies (I2=56%, p=0.06). This RR indicated a significantly better rate for carboplatin therapy (RR: 1.41, 95%CI: 1.23 to 1.62, p<0.00001) (Figure 2).
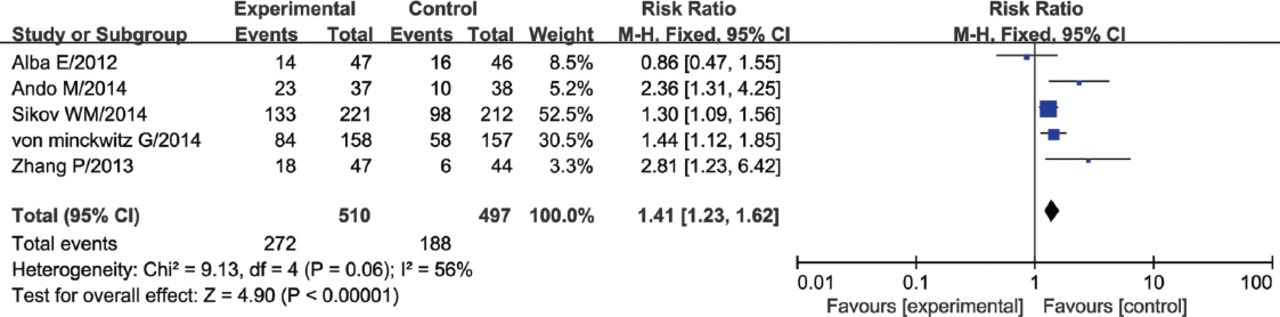
Forest plot of pathologic complete response rate for carboplatin-based relative to non-carboplatin-based preoperative chemotherapy. M-H - Mantel-Haenszel test, CI - confidence interval
Overall response
Two of the 5 studies reported ORR data.19,24 No significant heterogeneity was observed for this outcome among the 3 studies (I2=0%, p=0.89). The RR showed a slight benefit of carboplatin-based preoperative chemotherapy over non-carboplatin therapy, but the difference in ORR was not significant (RR: 1.11, 95%CI: 0.96 to 1.29, p=0.16) (Figure 3).

Forest plot of overall response for carboplatin-based relative to non-carboplatin-based preoperative chemotherapy. M-H - Mantel-Haenszel test, CI - confidence interval
Breast-conserving surgery
Breast-conserving surgery data were reported in 2 of 5 trials.19,20 No significant heterogeneity was observed among studies (I2=27%, p=0.24). The absolute BCS rate was 59.7% in carboplatin-based chemotherapy comparison with 48.1% in non-carboplatin therapy. The RR showed significant difference in BCS rate between carboplatin-based and non-carboplatin-based therapy (RR: 1.24, 95%CI: 1.06 to 1.46, p=0.007) (Figure 4).

Forest plot of breast-conserving surgery rate for carboplatin-based relative to non-carboplatin-based preoperative chemotherapy. M-H - Mantel-Haenszel test, CI - confidence interval
Safety
Patients who received carboplatin-based therapy showed significantly higher incidence of the following adverse events than patients who received non-carboplatin therapy: grade 3 or 4 anemia (p=0.01), neutropenia (p<0.00001), febrile neutropenia (p=0.03), and thrombocytopenia (p<0.00001). In contrast, both types of preoperative chemotherapy were associated with similar incidence of grade 3 or 4 fatigue (p=0.52), leucopenia (p=0.09), and nausea/vomiting (p=0.35).
Publication bias
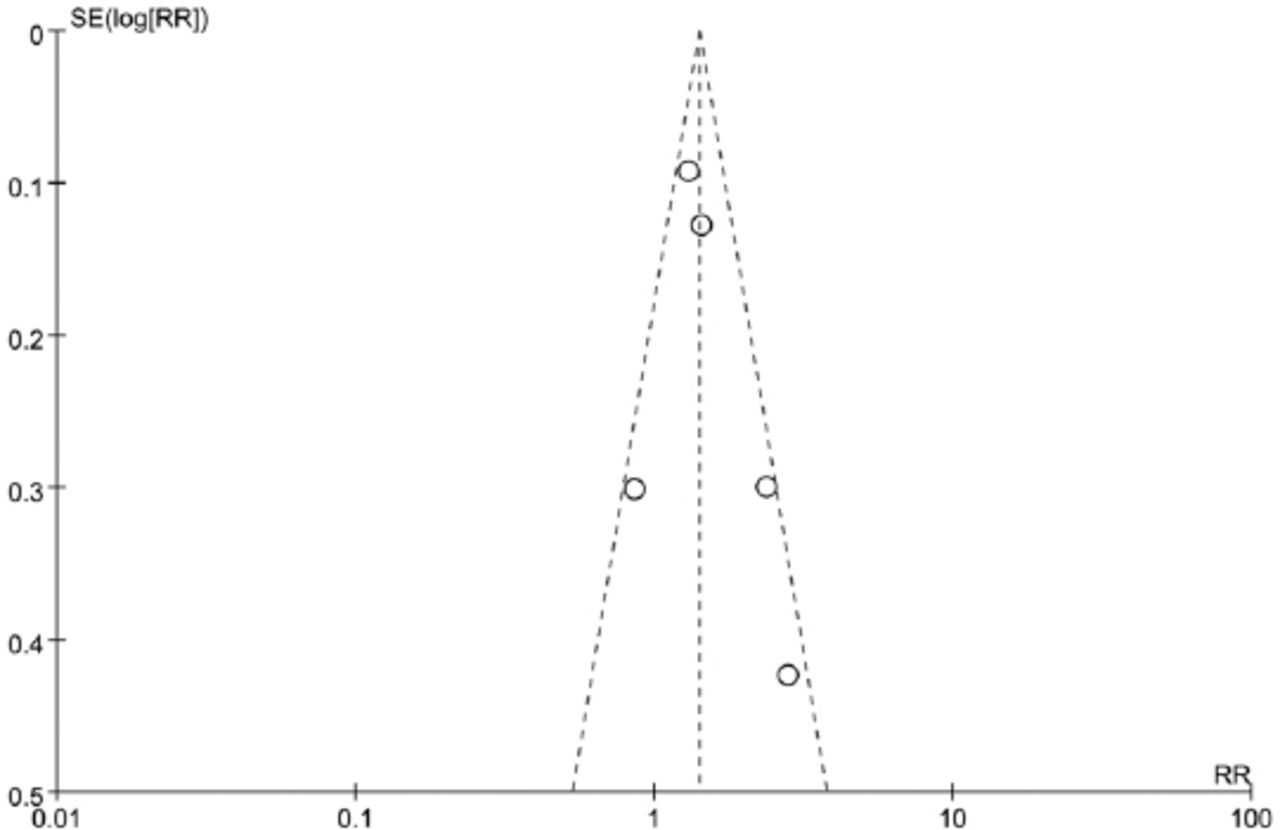
Publication bias was not found according to funnel plot for pCR (Figure 5). For ORR, BCS and safety analysis, it was inappropriate to evaluate the publication bias, since the lack of data provided.
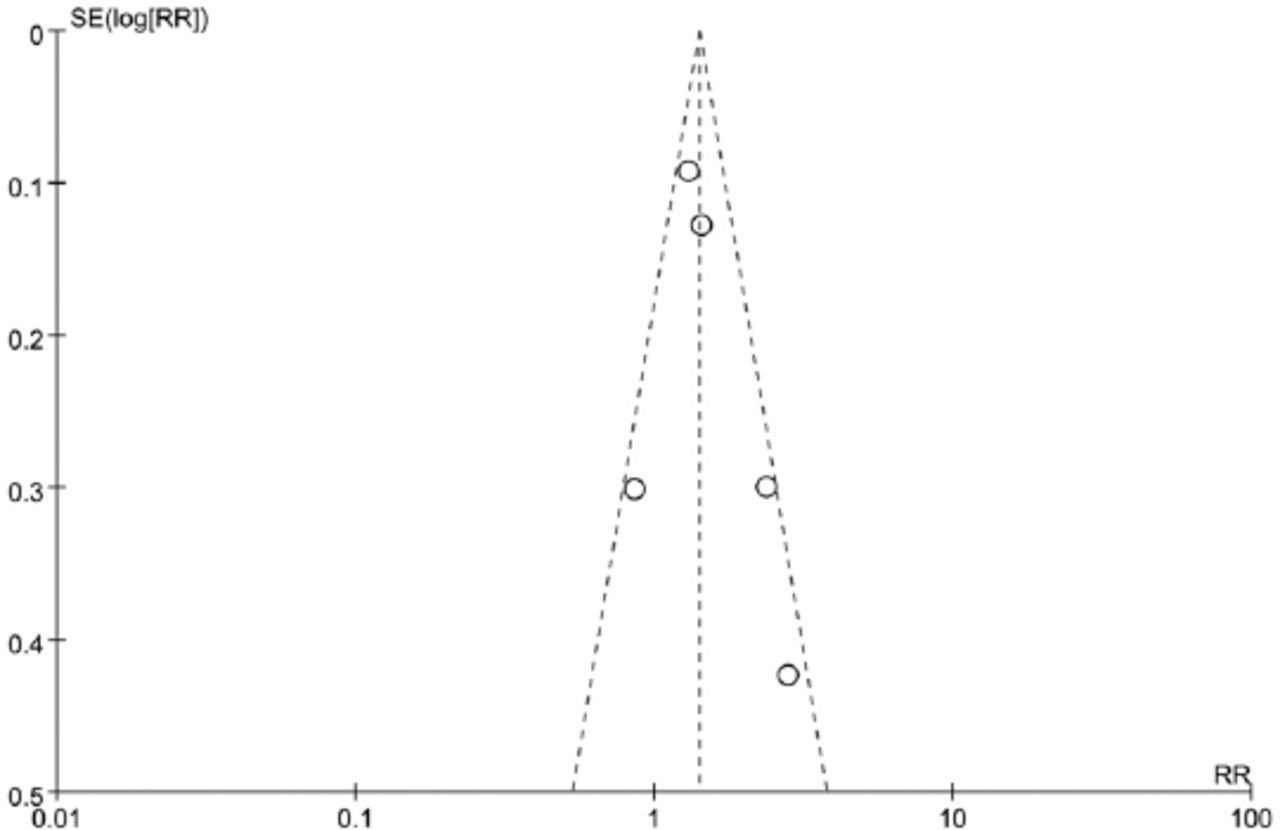
Funnel plot for publication bias in pathologic complete response analysis. SE - standard error, RR - relative risk
Discussion
Our meta-analysis aimed to assess evidence available from randomized controlled trials, suggest that carboplatin-based therapy is associated with significantly greater pCR and BCS rate than non-carboplatin therapy. To our knowledge, this is the first meta-analysis to evaluate the efficacy and safety of carboplatin-based preoperative chemotherapy for patients with TNBC. One meta-analyses while evaluated the value of platinum-based chemotherapy in TNBC, revealed that platinum-based preoperative chemotherapy significantly increase pCR rate in TNBC patients compared with containing no platinum drugs.25 The results of our meta-analysis further demonstrated that the addition of carboplatin to the preoperative chemotherapy regimen significantly increased pCR rate in TNBC patients. The conclusion on pCR of another meta-analyses26 regardng carboplatin and bevacizumab is in agreement with us. However, we newly found carboplatin can improve the BCS, but we evaluate the safety.
Preoperative chemotherapy for TNBC may be even more effective when conducted in the presence of antiangiogenic chemotherapy. In the GeparQuinto trial, while the pCR was evaluated in TNBC after neoadjuvant chemotherapy with or without bevacizumab; pCR was higher in adding bevacizumab (p=0.003).27 In another study, the addition of bevacizumab to neoadjuvant therapy was found to increase pCR rate in patients in early stages of triple-negative and HER2-positive breast cancer.21 At the same time, preoperative chemotherapy with bevacizumab may affect surgical incision healing. None of the studies in our meta-analysis examined bevacizumab, highlighting the need to assess this treatment in TNBC patients.
Preoperative chemotherapy may be used to slow tumor growth and thereby facilitate surgical resection. At the same time, such chemotherapy perhaps increases the risk of surgical complications. Our meta-analysis suggests that adding carboplatin to such chemotherapy significantly increases the incidence of grade 3 or 4 anemia, neutropenia, febrile neutropenia, and thrombocytopenia. We conclude from the available evidence that the toxic effects of preoperative chemotherapy exert only minor effects on the subsequent surgery.
This meta-analysis suffers from several limitations. First, the small number of randomized controlled trials and study subjects may affect the statistical power and reliability of our meta-analysis. In addition, not all trials reported data on all relevant outcomes. Second, our meta-analysis was based on aggregate rather than individual patient data, which can lead to higher efficacy estimates.28 Third, our meta-analysis evaluated the efficacy of carboplatin combined with taxanes, so the findings may not be relevant to other chemotherapy regimens. This meta-analysis cannot answer the question of which chemotherapy regimen is the best choice for TNBC. Fourth, the pCR definition in the included studies was completely the same, which may lead to certain heterogeneity.
In conclusion, our meta-analysis of available evidence from randomized controlled trials suggests that carboplatin-based preoperative chemotherapy leads to significantly higher pCR and BCS rate in TNBC patients than non-carboplatin therapy. Further large-scale, prospective, randomized, controlled clinical trials are required to investigate the survival benefits from carboplatin-based preoperative chemotherapy in TNBC patients.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received March 3, 2016.
- Accepted October 18, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.