


Abstract
Objectives: To evaluate the horizontal and vertical location of the mental foramen (MF), as well as the relationship of lower premolars to buccal and lingual cortical plates using cone beam computed tomography (CBCT).
Methods: Retrospective cross-sectional study conducted using CBCT scans that were obtained between early 2014 and late 2016 from King Saud University Dental hospital database in Riyadh, Kingdom of Saudi Arabia; 94 patients (53 males and 41 females) were included. Three examiners independently performed one-sided measurements for each patient. Data analyzed statistically and a p<0.05 was considered significant.
Results: The mean distances from the outer boundary of the buccal cortex to the first and second premolars (R1) were 1.55 mm and 1.98 mm. The mean distances from the outer boundary of the lingual cortical plate to the first and second premolars (R2) were 4.06 mm and 4.73 mm. The respective mean total bone thicknesses, including the roots of the first and second premolars (R3), were 9.32 mm and 10.08 mm. The mean distance between the MF and the mandibular second premolar apex was 3.13 mm.
Conclusion: Mandibular premolars are in close proximity to MF especially mandibular second premolar. Presurgical assessment is essential when surgical treatment is planned at this area.
The positions of the inferior alveolar canal (IAN) and mental nerve, in relation to mandibular premolars and adjacent structures, are important for planning surgical procedures, including tooth extraction, implant placement, and endodontic surgery. Although it varies, the most commonly reported location of the MF is apical to the mandibular second premolar.1 Notably, this position may be affected by ethnic differences.2 Several studies have evaluated the position of the mental foramen in Saudi populations. In a study utilizing panoramic radiographs, the most common position of the mental nerve was parallel to the mandibular second premolar (45%), and between the premolars in (42%).3
Most studies evaluating the mental nerve and foramen have been performed with cadavers, panoramic radiographs, ultrasonography, and (more recently) CBCT.3-6 Cone beam computed tomography is currently the radiographic technique of choice for imaging hard tissues in the oral cavity because it shows anatomical structures without superimpositions and distortion, which are observed in conventional imaging modalities, such as panoramic imaging, at low radiation doses compared with multi-detector computed tomography (CT) imaging.
We aimed to evaluate the vertical and horizontal positions of the mental foramen, as well as the relationship of lower premolar teeth to buccal and lingual cortical plates by using CBCT.
Methods
Retrospective cross-sectional study conducted using CBCT data of patients who underwent scans between early 2014 and late 2016 were retrieved from the oral and maxillofacial radiology database in King Saud University, Dental Hospital in Riyadh, Kingdom of Saudi Arabia, after ethical approval from the College of Dentistry Research center (CDRC) at King Saud University in Riyadh, Kingdom of Saudi Arabia. The inclusion criteria were patients of Saudi origin who exhibited first and second premolars in both right and left sides, and who were 18 years of age or older. Patients who had any of the following conditions were excluded: presence of any lesion at the region of interest (ROI), history of orthodontic treatment, bone loss or defect in ROI, external or internal root resorption, radiographic evidence of skeletal/dental malocclusions, abnormal anatomy of roots, or endodontic treatment on teeth in the ROI.
All CBCT scans were acquired by using Promax 3D Max (Planmeca, Helsinki, Finland) with an isotropic voxel size between 0.2-0.4 mm. Assessment of anatomical structures and measurements were performed on Planmeca Romexis® 3.6 software (Planmeca, Helsinki, Finland). Images were viewed on a 30.4-inch TFT AM Color LCD Dual Domain IPS medical display Coronis Fusion MDCC-6130 (Barco, Belgium) at a resolution of 3280×2048. All measurements and analyses were performed by an oral and maxillofacial radiologist and 2 general practitioners who were trained by the maxillofacial radiologist.
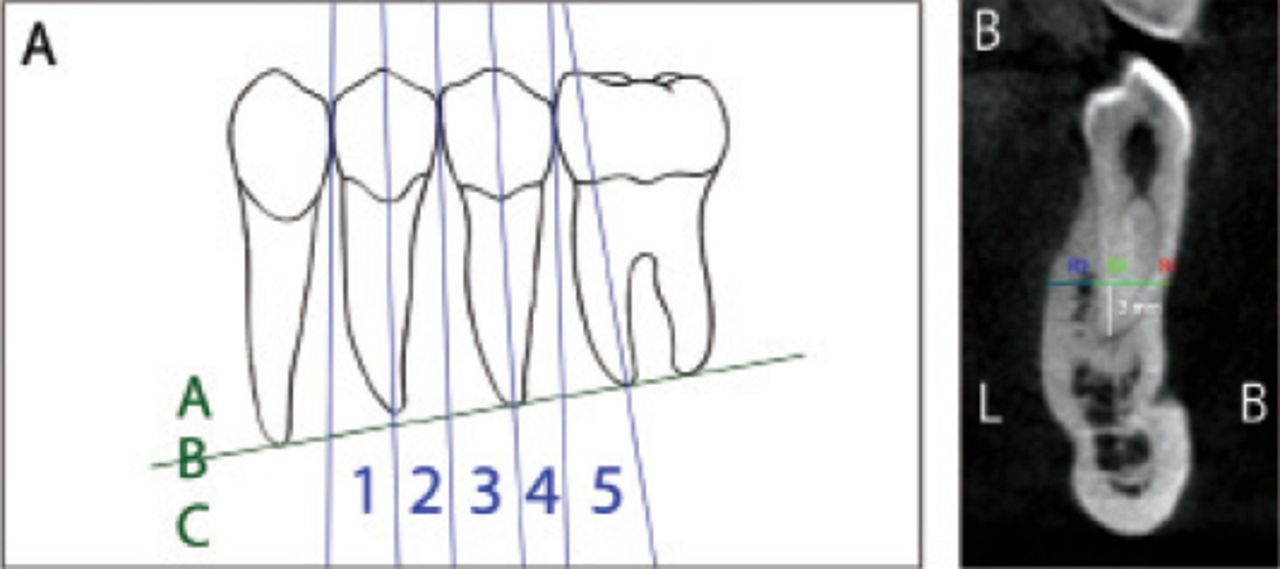
Panoramic reconstruction views were used to assess the horizontal and vertical relation of the MF to adjacent teeth (Figure 1A). For the horizontal position, it was designated as one of 5 areas as follows: H1) anterior to the first lower premolar; H2) distal to the first premolar and anterior to the line dividing the interproximal area between the first and second premolars; H3) distal to the line dividing the interproximal area between the first and second premolar, and mesial to the second premolar; H4) distal to the second premolar and mesial to the line dividing the region between the first molar and second premolar; H5) Posterior to the line dividing the interproximal area between the second premolar and first molar. Vertically, the MF position was compared to the root apices of both premolars and first molar and was considered to be: A) superior to the root apices level; B) in line with the root apices level; C) inferior to the root apices level.

The mental foramen position in relation to teeth and determinations of mandibular bone thickness. X - axis: vertical position, Y-axis: horizontal position
The shortest distance between the outer rim of the MF and the nearest root surface was measured by using oblique sections that intersected both points. After aligning the sagittal and coronal sections to the root long axis, thickness of the mandibular bone at 3 mm above the root apex for the first and second premolars was measured on paracoronal sections. We measured the bone thickness: R1) buccal to the root, R2) lingual to the root and R3) the whole bone thickness including the root. (Figure 1B)
Eight double-blinded random cases were selected as pretest cases to determine the accuracy and reliability of measurements. Measurements were performed for the selected cases twice, separated by one week. Inter- and intra-examiner reliability was tested using interaclass correlation coefficient and it showed excellent reliability (ranging from 0.942-0.997). Descriptive data analysis was performed and independent t-tests were used to compare means between the groups. P-values<0.05 were considered significant and using SPSS 20 software (IBM Corp., Armonk, NY, USA).
Results
Of the 208 reviewed CBCT scans, 94 patients met the inclusion criteria; these 94 patients included 53 males (56.38 %) and 41 females (43.62%). The mean age of the patients was 33.5±14.79, ranging from 18-78 years. No significant difference was found between the right and left sides in all measurements for each patient (p>0.05). The respective mean distances from the outer boundary of the buccal cortex to the first and second premolars (R1) were 1.55±0.87 and 1.98±1.21. The respective mean distances from the outer boundary of the lingual cortex to the first and second premolars (R2) were 4.06±1.67 and 4.73±1.48. The respective mean total bone thicknesses, including the roots of first and second premolars (R3), were 9.32±2.01, and 10.08±1.97. There was a significant difference between male patients (10.5±1.94) and female patients (9.52±1.87) in the total intercortical bone thickness (R3) at the second mandibular premolar (p=0.016).
Vertically, the MF was located apical to mandibular premolars in 80 patients (85.1%), at the same vertical plane of premolar root apices in 13 patients (13.8%), and coronal to the root apices in one patient (1.1 %). A statistically significant difference between genders was found: more females (24.4%) exhibited the MF at the level of the premolar apices (B), compared with males (5.7%; p=0.025); more males exhibited the MF apical to the root apices (92.5%), compared with females (75.6%).
Horizontally, the MF was located in areas posterior to the long axis of the first premolar and anterior to the line dividing the interproximal area between premolars in 7 patients (7.4%). However, it was located posterior to the line dividing the interproximal area between the premolars and anterior to the line along the second premolar in 64 patients (68.1%), and posterior to the line along the long axis of the second premolar and anterior to the line dividing the interproximal region between the first molar and second premolar in 23 patients (24.5%). The mean distance between the MF and the mandibular second premolar apex (the nearest tooth), was 3.13±1.69 mm, no significant difference was found between genders (p>0.05).
Discussion
Knowledge of the bone shape and thickness, as well as vital structures near the root apex of a tooth planned for endodontic surgery, is essential for successful treatment. Cone beam computed tomography provides a better tool for linear measurements, compared with conventional imaging methods.7
The bucco-lingual mandibular bone width is known to increase from the premolar area to the molar area.8 Chinoa et al,9 reported that bone width, buccal to mandibular premolars and molars, at 3 mm coronal to the root apex, and they discovered that the width of the buccal bone increases from the first premolar to the second premolar. Notably, they found that the bone width lingual to the roots is similar for both premolars. Our study showed that the bone width, both lingual and buccal to the root of the second premolar, is thicker than at the first premolar. Males had thicker bones at the area of premolars, compared with females; however, this difference was statistically significant only at the level of the second premolar. Talaat et al,10 measured cortical and cancellous bone width buccal to the roots of mandibular teeth in 80 CBCT scans at the level of the mid-apical third; they discovered that the mean bone width at the first premolar was 2.74±0.8 mm and at the second premolar was 3±0.62 mm. The difference in our measurements is likely because Talaat et al,10 obtained their measurements at an area that is more apical than where we obtained our measurements. However, buccal bone width noticeably increases when moving from the first premolar to the second.
Al-Mahalawy et al,11 studied the location of the MF and frequency of anterior loop in the CBCT data of 302 Saudi patients; they found that the MF was located apical to the second premolar in 52%, and between the premolars in 27% of their study population. Other studies revealed that 50-60% of MFs were located between the first and second premolars and 30-40% were located apical to the second premolar.6,12 Our results are consistent with those of previous studies and show that the MF is found in close proximity to the root of the second premolar, with 68.1% of MFs located at H3 and 24.5% at H4; both locations are very close to the root of the second premolar. Only 7.4% of MFs were located at H2, which is closer to the root of the first premolar.
Several studies have evaluated the vertical location of the MF in relation to the crest of the alveolar bone and the inferior border of the mandible.6,13 Few studies have compared the vertical location of the MF relative to the apices of adjacent teeth, which is clinically more relevant for apical surgery.14 In the current study, the MF was commonly found apical to the root apices of posterior teeth (85.1%). However, more females (24.4%) exhibited the MF at the apices level, compared with males (5.7%); this difference could be because females have smaller mandibles than males.
To avoid injury to the mental nerve, it is essential for the practitioner to know the proximity of the MF to the root apex, prior to endodontic treatment or endodontic surgery. We found that the mean distance from the nearest tooth root apex, most commonly the second premolar, to the MF was 3.13 mm. Our results are in agreement with a study by Al-Mahalawy et al,11 who reported the mean distance from the nearest tooth apex to the MF to be 3.1 mm. Interestingly, Kalender et al,12 examined 386 sites in 193 Turkish patients and found that the mean distance from the nearest root apex to the MF was 4.2 mm; this disparity could possibly be attributed to racial/ethnic differences.
A limitation of the current study is its small sample size, where its results cannot be generalized on the whole population. Further studies with a multi-center design that includes larger sample size and a comparison of different ethnicities of Saudis and non-Saudis is recommended to have better understanding of measurement differences.
In conclusion, dental practitioners treating Saudi patients must be familiar with the location of the MF and its relation to neighboring teeth. Mandibular premolars are in close proximity to MF especially mandibular second premolar. Presurgical assessment is essential when surgical treatment is planned at this area.
Acknowledgment
The authors gratefully acknowledge Prince Naif Bin Abdulaziz Health Research Center, King Saud University, Riyadh, for reviewing the manuscript; and the College of Dentistry Research Center and the Deanship of Scientific Research, King Saud University, Riyadh, Kingdom of Saudi Arabia for their support on this research project. We also thank Editage for English language editing on the current research.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 20, 2018.
- Accepted January 3, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.