


Clinical Presentation
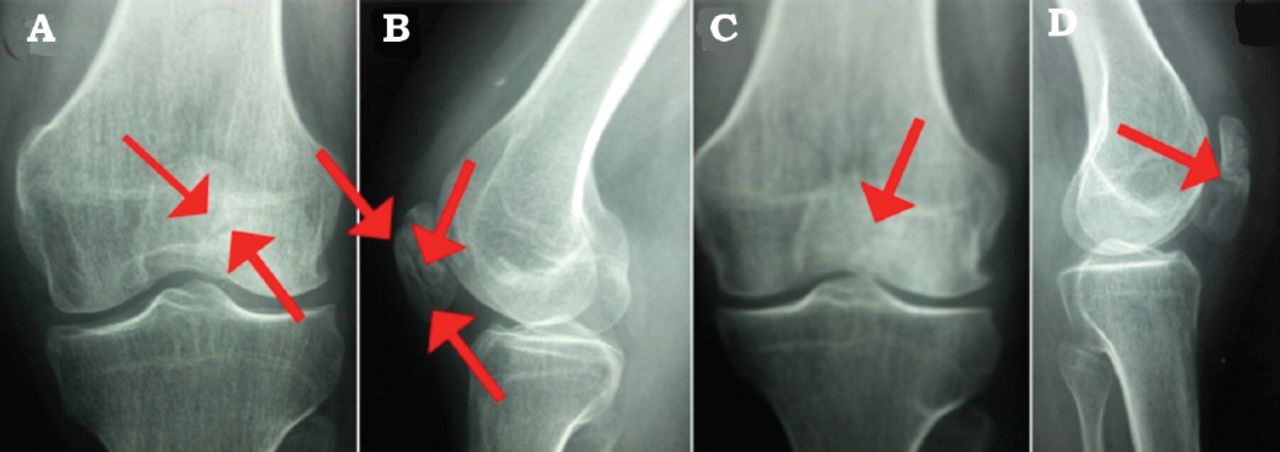
A 16-year-old male presented to us with complaint of pain in front of both knees for 8 weeks. Pain was insidious in onset and dull aching in nature initially. Severity of pain increased with time. Pain aggravated on sporting activities such as running, climbing stairs, playing cricket, and get relieved on taking rest and analgesic. There was no history of trauma, crepitations, and clicking. On physical examination, gait was normal, mild tenderness was present over the superolateral portion of patellae, no joint effusion, or swelling. Range of motion was normal bilaterally with mild pain on terminal flexion. Quadriceps strength was normal bilaterally. All the ligaments and menisci were found intact on performing various clinical tests such as anterior and posterior drawer tests, Lachman’s test, valgus and varus stress tests, McMurray test, Apley’s distraction, and compression tests. Anteroposterior and lateral radiographs of both knees were advised (Figure 1).
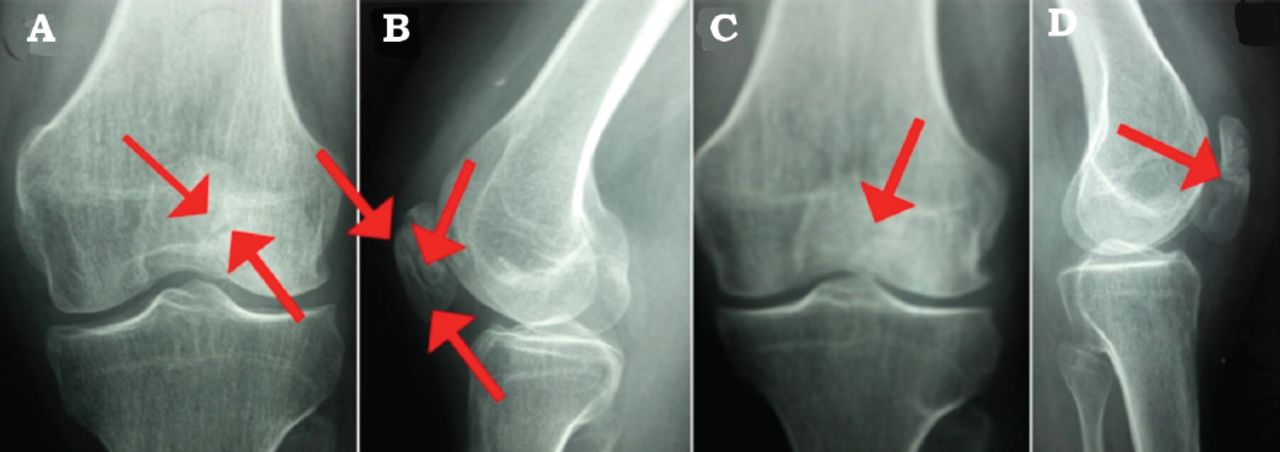
Anteroposterior and lateral radiographs of both knees.
Questions
What are the findings on plain x-ray?
What is the diagnosis?
What is the management in this case?
Answer
Anteroposterior and lateral radiographs of bilateral knees (Figures 1A & 1B) showed radiolucent line between the 3 fragments of patella and margins of fragments seem to be smooth and sclerotic. Figures 1C & 1D showed radiolucent line between the 2 fragments of patella and margins of fragments seems to be smooth and sclerotic
The diagnosis is tripartite patella right knee (Figures 1A & 1B) and bipartite patella left knee (Figures 1C & 1D). This also known as Haswell lesion and idiopathic osteonecrosis of the patella. This is a clinico-radiological diagnosis.
We have managed this patient conservatively with rest, non steroidal anti-inflammatory drugs and knee cap. We also advised quadriceps and hamstrings stretching exercises and avoid sternous activities for 2 weeks. Patient responded well to this treatment and symptoms subsided over 6 weeks of treatment. Patient gradually regains his activities and fully satisfied with outcome.
Discussion
Partite patella is asymptomatic in most of the patients and usually diagnosed incidentally. It developed due to failure in fusion of accessory ossific nucleus of patella with primary ossification centre in adolescence. This accessory ossific nucleus appears approximately 12 years of age. Patella usually develops from a single ossification nucleus which appears between 3-5 years of age and ossified from centre to periphery. Failure of fusion of these ossification centres may give rise bipartite, tripartite or multipartite patella.1 Bipartite or tripartite patella becomes symptomatic in young active individuals following direct trauma, overuse, or strenuous athletic activity.
Bipartite patella is more common in males and 50% of these occur bilaterally. In 2% to 13% patients, bipartite patellae are symptomatic and cause anterior knee pain as in present case.1 Bipartite patella is also known as Haswell lesion, and idiopathic osteonecrosis of the patella.
Partite patella has classified into four types, superolateral bipartite, lateral bipartite, superolateral and lateral tripartite, superolateral tripartite.2
Traumatic and stress fracture of patellar should always considered in differential diagnosis of bipartite or tripartite patella. These developmental anomalies can be differentiated from traumatic fractures using radiography, computed tomography, magnetic resonance imaging, or isotope bone scanning. Magnetic resonance imaging is the investigation of choice in doubtful cases. Traumatic fractures can be differentiated on the basis of fracture margin which are more ragged whereas in non-traumatic fractures, the accessory ossific nucleus likely to have sclerotic, smooth margins.1
Treatment options for symptomatic multipartite patella vary from conservative to surgical treatment. Conservatively, we can manage the patient with rest, Non-steroidal anti-inflammatory drugs, patellar braces, quadriceps and hamstrings stretching exercises, and sometimes local steroid infiltration may also required. Present case responded well to conservative treatment. Nowadays, commonly performed surgical procedure is arthroscopic excision of the painful fragment.3 Other surgical options are lateral retinacular release, vastus lateralis release, and internal fixation with or without bone grafting.2,3
In conclusion, our case is unique because the presence of tripartite patella on one knee and bipartite patella on the other knee. A thorough clinical examination and plain radiographs can diagnose ossification anomalies of patella easily, thus obviating the need for MRI, especially in a poor socioeconomic set up. We should keep the partite patella in differential diagnosis of anterior knee pain in adolescence.
Acknowledgment
We gratefully acknowledge Dr. Saifullah Khalid, Assistant Professor, Department of Radio diagnosis and Dr. Ziaul Hoda Shaan, Junior Resident, Department of Orthopedic Surgery, for valuable assistance in the management of the patient and preparing this manuscript.
Footnotes
Notice: Authors are encouraged to submit quizzes for possible publication in the Journal. These may be in any specialty, and should approximately follow the format used here (maximum of 2 figures). Please address any submissions to: Editor, Saudi Medical Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. Tel. +966 (11) 4777714 Ext. 42841.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.