


Abstract
Objectives: To evaluate the origin, distribution pattern, branches, and neighboring structures of the iliolumbar artery (ILA) concerning the anterolateral surgical approaches to the spine.
Methods: This study was performed in the Anatomy Department of Medical School, Mersin University, Mersin, Turkey between 2014 and 2015. Pelvises of 11 male formalin-fixed human cadavers were dissected by anterior and posterior approaches under surgical microscope. The origins, distribution patterns, calibers, and distances to certain structures were measured.
Results: The ILA was found as a single trunk on 17 sides arising either from the IIA (12 sides, 70.6%) or the PT (5 sides, 29.4%). The average caliber of those originated from the posterior trunk was significantly larger (p=0.010). The ILA started as a single trunk in 17 sides, while its lumbar and iliac branches separately originating from different arteries in 4 sides. The close relation of the posterior rami of both the lumbar and iliac branches with transverse process and spinal nerve were noted.
Conclusion: Findings suggest that the ILA and its branches may have different and significant patterns, which may be crucial to consider during certain surgical procedures, such as far lateral disc herniation and posterior pelvic fixations.
The variations and branching patterns of the iliolumbar artery (ILA) and its branches are very crucial for surgeons. Iliolumbar artery has the risk of injury in pelvic trauma and regional operations.1-4 Additionally, variations in the branches of ILA may be important concerning its use as feeding pedicle in bone flaps.1,2,5 Although ILA was defined as the first branch of the posterior trunk (PT) of the internal iliac artery (IIA) in classical textbooks,6,7 it may originate from the common iliac artery (CIA),1 or the IIA.8,9 However, no data has been reported in the literature regarding the origins, branching patterns and locations of lumbar (LB), and iliac (IB) branches of ILA. No data was encountered in the literature on the course of the posterior and spinal branches (SB) related with vertebral surgery. The primary purpose this study was to evaluate the origin, branches, and distribution patterns of the ILA. The second purpose was to determine its relations with neighboring structures in order to provide proper data for surgeons to avoid complications.
Methods
Pelvises of 11 male (11 right and 10 left sides) formalin-fixed human cadavers (mean age 80 ± 18.022) were dissected under surgical microscope at the Anatomy Laboratory of the Medical School, Mersin University, Mersin, Turkey, between 2014 and 2015. This study was approved by the Dean of Mersin University, Mersin, Turkey. Vascular structures of pelvis and posterior abdominal wall were dissected. Left side of one cadaver was excluded due to the previously disrupted vascular structures. Anterior approach was performed for all cadavers. In 3 cadavers in whom the IB and LB was giving branches, which were passing deep to the transverse process, posterior approach to lumbar spine was additionally performed to detect the relation between the posterior continuations of the branches and the lumbar vertebral structures (facet joint, transverse process, pedicles). The origins, distribution patterns, calibers, and distances to certain structures, such as spinal nerve and transverse process were measured with digital caliper. We used mean, median, standard deviation, and minimum and maximum values as descriptive statistics for all parameters (Table 1). Coherence to normal distribution analysis was prepared using the Shapiro Wilk’s test. The difference between the calibers of ILA originating from the PT and IIA was tested using the Permutation test. We added 5%, 10%, and 1% confidence intervals for means as a result of Permutation test. The sample size was small; thus, distributions were highly skewed. We used Spearman’s Rank Correlation Coefficient for extracting related numerical parameters. All results were accepted statistically significant for p<0.05. Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, USA) version 7 software.
Origin and average caliber of the iliolumbar artery (ILA), lumbar (LB), and iliac branches (IB) in 17 sides.
Results
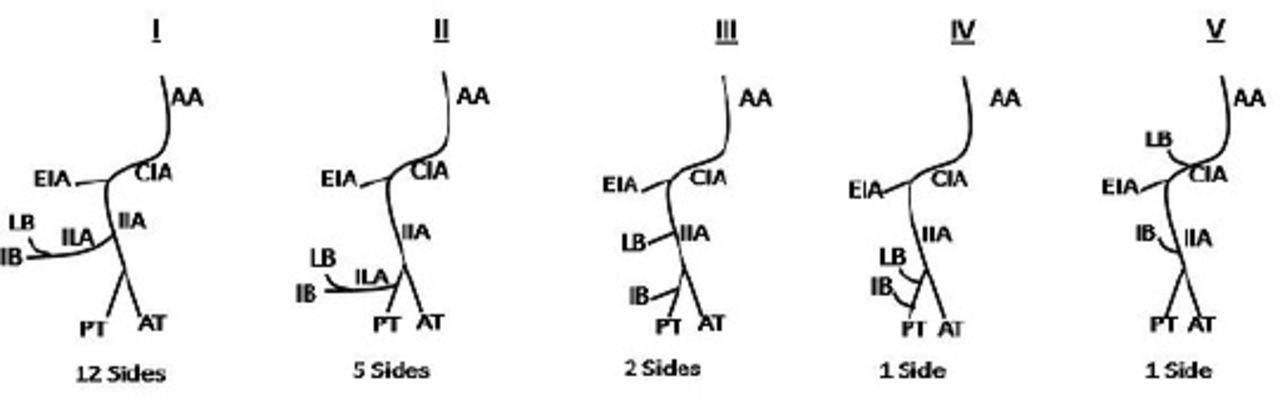
The ILA was found as a single trunk on 17 sides arising either from the IIA (12 sides, 70.6%) or the PT (5 sides, 29.4%) (Table 1) (Figure 1). On the other 4 sides, no ILA was observed; instead there were branches, which coursed similar to LB and IB. All vessel calibers were measured on their origin (Table 1). The average caliber of ILA diverging from the IIA was 3.20 mm, while diverging from PT was 3.89 mm (Table 1). Iliolumbar artery, which diverged from PT was found significantly larger than those which diverged from IIA by independent T test (p=0.010). Permutation test showed that the IB and LB calibers varied depending on their origin (p=0.048). Analysis showed that IB caliber was significantly larger than LB caliber in all sides (p=0.002). Moreover, LB and IB diverging from PT were significantly larger than those diverging from IIA (p=0.010). Spinal branches reached only to the L5-S1 disc space on 12 sides (57.1%), whereas it supplied both the L4-L5 and L5-S1 disc spaces on 7 sides (33.3%). Their average calibers on L4-L5 disc space was 0.44 mm, and L5-S1 was 0.40 mm. No spinal branch was detected on 2 sides (9.5%). Correlation between the left and right L5-S1 was 20.8%. The confidence interval of this coefficient was -75% and -18.8%. Lumbar was passing from the anterior part of the lumbosacral trunk (LT), obturator nerve (ON), and the femoral nerves (FN) on 16 sides (76.2%), while it was passing posterior to these structures on 5 sides (23.8%). In one of the cadavers, LB had anastomoses with the fourth lumbar artery on both sides and a communication with the median sacral artery (MSA) on the right side. In another cadaver, LB had 2 branches: one was coursing towards the promontorium and entered the L5-S1 disk space anteriorly. The second branch coursed to the left side and divided into 2. These 2 branches distributed on the fifth vertebral body and each of them were separately anastomosed with 2 variant branches coming from the common iliac artery. Double LB was encountered on the right side (4.8%). Another unusual pattern was the branches of LB to the first anterior pelvic foramina bilaterally. In one cadaver, IB was giving a posterior branch, which was directed towards the iliolumbar ligament to supply the iliac crest on the right side. On the left side of the same cadaver, the obturator artery was originating from IB. The LB provide a branch, which passed inferior to the fifth transverse process (TP) and continued posterior to it on 4 sides (19.1%) (Figure 2). The average distance to fifth TP was 2.6 mm and the average caliber was 1.48 mm. Similarly, in only one cadaver, IB bilaterally have a posterior branch, which passed inferior to the fifth TP, and coursed posteriorly. The average distance to fifth TP was 1.83 mm and the average caliber was 1.58 mm. A branch diverged from LB in one cadaver, and from IB in another coursed posterior to the L4 spinal nerve and unilaterally reached to the fifth facet joint.

Schematic view of the distributions of the iliolumbar artery (ILA) and its branches. The ILA was a single trunk in I-II. In III-IV-V, no ILA was observed; instead there were branches, which coursed similar to lumbar (LB) and iliac branches (IB). AA - abdominal aorta, CIA - common iliac artery, EIA - external iliac artery, IIA - internal iliac artery, AT - anterior trunk, PT - posterior trunk

The figure and schematic illustration show the course of the lumbar branch (LB): A) indicates photograph; and B) indicates schematic illustration, LB passed inferior to the 5th transverse process (L5-TP) and continued posterior to it on the left side (black arrow). L5-SN - 5th lumbar spinal nerve, * spinal branches of LB, white arrow - branch from LB to vertebral body, x - superior-inferior line, y - left-right line.
Discussion
Variations regarding the location and origin of branches of the ILA are very crucial for surgeons.1-4 Iliolumbar artery was detected arising either from the lumbar, middle sacral, and the lateral sacral arteries.6 In our series, we detected ILA in all cases; they were originating either from IIA or PT. We did not encounter any branch diverging from the common iliac or gluteal arteries. Origin of ILA has been given with various ratios: ILA may originate from the common iliac with a ratio of 3.7-11.25%.1-5 Similarly, ILA has been reported to originate from IIA with a wider range in various studies as 28.3-96.3%.1,5,8,9 Furthermore, ILA has been reported to originate from PT with a ratio of 32.5-44%.5,9. In our series, 70.6% of the cases were originating from IIA while 29.4% were originating from PT. Thus, our ratios are consistent with those of early reports for the origin of ILA from IIA.5,8,9 Comparing with the previous studies, our results show lower percentages for ILA diverging from PT.1,3,5 No data was encountered in the literature regarding the separate origin of LB and IB of ILA.
Our findings suggest that LB and IB may diverge separately (4 sides), and this information is so crucial for surgeons that work on the pelvis. Considering the diameters, distribution patterns, and neighboring structures of LB in this group, no difference was detected between them and the ones which classically arose as a single trunk. Chen et al1 reported the caliber of the ILA during its course on the medial side of psoas major as 2.7 ± 0.6 mm. Harrington2 reported this diameter as 3-4 mm, and Kiray et al3 reported the diameter of ILA at its origin as 3.7 ± 0.7 mm. Our findings show the average calibers of ILA are in accordance with those of Harrington2 and Kiray et al3 It was remarkable that the caliber of ILA, which diverged from PT was larger than those which diverged from IIA. No data was encountered in the literature regarding the calibers of LB and IB. Analysis showed that IB caliber was larger than LB caliber in all sides. Moreover, IB and LB calibers varied depending on their origin, which has not been mentioned previously in the literature. Our findings show the positional relation of ILA with the LT, ON, and FN is in accordance with literature.6 However, Teli et al10 reported that ILA coursed anterior to the LT in 30% of the cadavers (12 cases), posterior in 54% (24 cases), and cleaved in 8% (2 cases). The possibility of the anterior course of the branches of ILA around the LT and ON may be critical during anterolateral approaches. Far lateral disc herniation represents only 10-12% of all disc herniations and is most common at L4-L5 and L3-L4 levels.11
There are 3 main approaches to root decompression in far lateral disc herniation: midline, paramedian, and endoscopic. Midline approach may provide inadequate exposure to the foraminal area and can require extensive removal of a facet. Paramedian approach for far lateral disc excision has become popular. The paramedian muscle splitting microsurgical approach was found to be the most direct and favorable anatomical route to herniations lateral to the neural foramen.12 Variations of ILA may increase the risk of potential complications during extra-foraminal disc exploration.
One of the limitations of the present study is that the available number of female cadavers was restricted. Therefore, the small number of female cadavers was excluded to eliminate effects of gender differences on arterial measurements. Additionally, multiplicity in variations of branching pattern also complicated the statistical evaluations.
Anastomotic communications of LB with MSA and IIA may be significant in several surgical approaches to anterior vertebral region. No data was encountered in the literature regarding the spinal branch of LB to the L4-L5 disc space. Also, the negative correlation between the calibers of the right and left spinal branches to L5-S1 disk space is interesting, reflecting a bilateral arterial supply pattern, but the level was supplied principally by one side.
In conclusion, the ILA and branches may have different and significant patterns, which may be crucial to recognize during certain surgical procedures. Further studies in larger series will help clarify the branching and distribution patterns.
Clinical Practice Guidelines
Clinical Practice Guidelines must include a short abstract. There should be an Introduction section addressing the objective in producing the guideline, what the guideline is about and who will benefit from the guideline. It should describe the population, conditions, health care setting and clinical management/diagnostic test. Authors should adequately describe the methods used to collect and analyze evidence, recommendations and validation. If it is adapted, authors should include the source, how, and why it is adapted? The guidelines should include not more than 50 references, 2-4 illustrations/tables, and an algorithm.
Acknowledgment
The authors would like to thank the donors of the cadavers used in this study.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received November 14, 2015.
- Accepted January 25, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.