


Clinical Presentation
A 46-year-old woman presented with a 6-month history of anorexia and loss of weight. This was associated with a 2-month history of cloudy urine. The only significant past medical history was a previous ectopic pregnancy. On examination, she was hypertensive with a blood pressure of 196/102 mm Hg. The patient was afebrile with a normal pulse and respiratory rate. Abdominal examination revealed non-tender ballotable kidneys bilaterally. Her renal function was impaired with a urea of 26.2 mmol/L (normal range: 73.4 mg/dL) and a serum creatinine of 790 umol/L (normal range: 8.94 mg/dL). Urine analysis revealed proteinuria, hematuria, and a leucocyte count of >1000/HPF. Blood count showed a normocytic anemia of 7.7 g/dl and a raised white blood cell count of 13.0 x 109/L. She was rehydrated and treated with antibiotics. Renal ultrasound showed dilated calyces bilaterally with bilateral renal calculi. An initial diagnosis of obstructive uropathy was made and bilateral retrograde pyelogram (RPG) and stenting was carried out. Plain radiograph (Figure 1) and a plain CT of the abdomen (Figure 2) were carried out to evaluate the cause of the urinary tract obstruction. As the renal function remained severely impaired in spite of this procedure, bilateral nephrostomy was performed. Culture of pus aspirated from the renal calyces yielded Proteus mirabilis and Pseudomonas aeuroginosa. The urine culture was negative. Following discussions in multiple multi-disciplinary meetings, it was decided that she requires a bilateral nephrectomy, which was carried out with no immediate complications. Hispathological evaluation of the kidneys revealed acute inflammatory exudates and mixed inflammatory cells including neutrophils, lymphocytes, plasma cells, multi-nucleated giant cells, and abundant foamy histiocytes forming xanthogranulomas. She was discharged 10 days after surgery with regular dialysis.

Plain film of the abdomen showing bilateral staghorn calculi (white arrows).
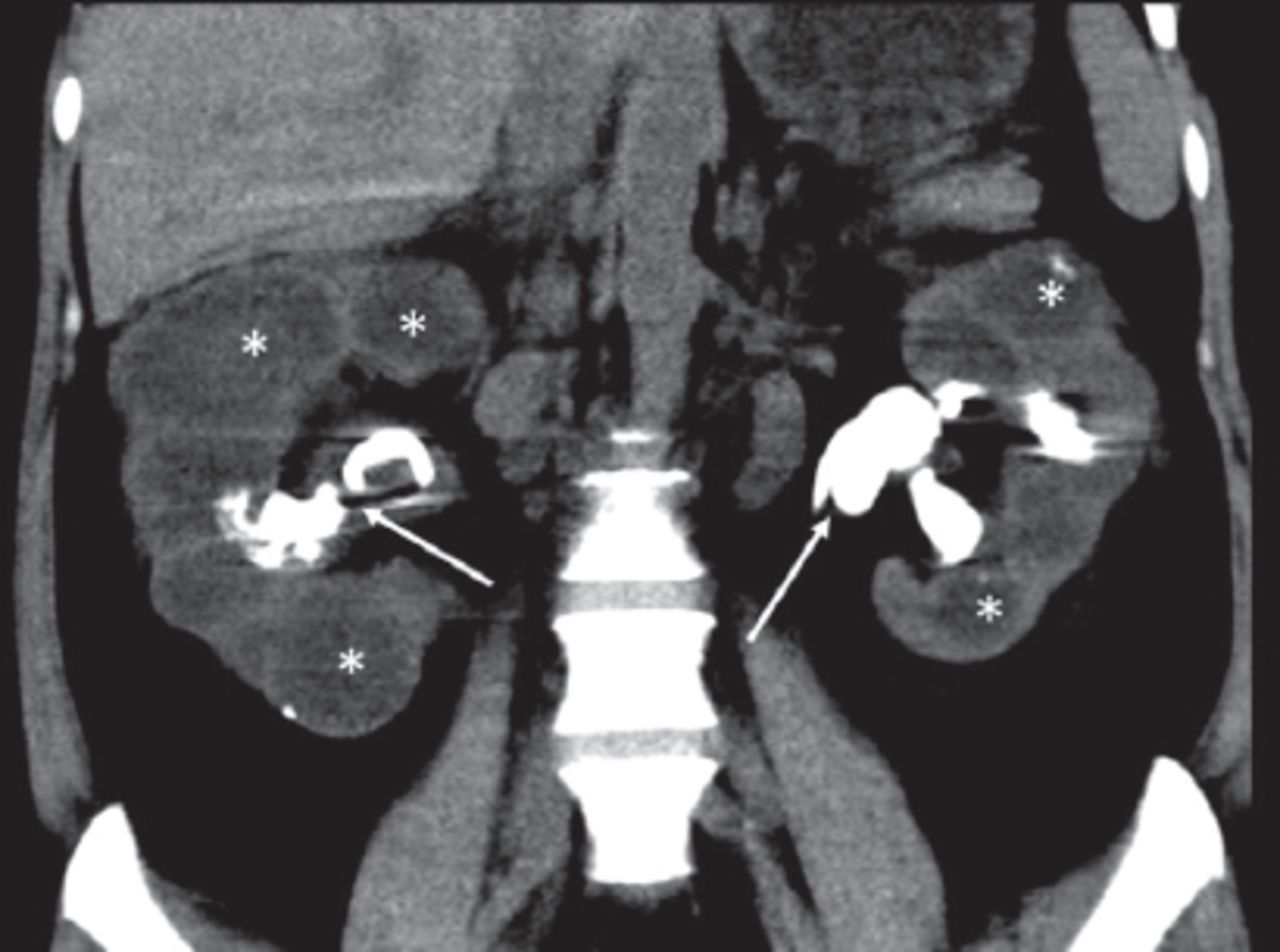
Coronal CT image showing bilaterally enlarged kidneys with bilateral staghorn calculi (white arrows), dilated calyces (asterisks) and paradoxical contracted renal pelves.
Questions
What are the findings on plain film and CT of the abdomen.
What radiological sign is seen on the CT?
What is the diagnosis?
Answers
The plain radiograph of the abdomen shows bilateral staghorn calculi with enlarged renal silhouette bilaterally. The CT shows dilatation of the renal calyces bilaterally with paradoxical contraction of the renal pelves.
Dilatation of the renal calyces with paradoxical renal pelvis contraction gives the bilateral “bear paw” sign.
Xanthogranulomatous pyelonephritis.
Discussion
Xanthogranulomatous pyelonephritis (XGP) is an uncommon form of bacterial pyelonephritis with an incidence of 1.4 per population of 100 000 per year.1 Almost all cases of XGP are unilateral. Bilateral involvement is extremely rare. Chronic obstruction of the urinary tract leads to destructive replacement of the renal parenchyma by granulomas, abscesses, and lipid laden macrophages, which is the hallmark of XGP. Diffuse XGP accounts for 90% of cases and focal XGP accounts for the remaining 10%. The typical CT findings in diffuse XGP are of dilated calyces with paradoxical contracted renal pelvis giving a ‘bear paw’ sign, with the dilated calyces resembling the toe pads of a bear’s paw.2 Focal XGP exhibits similar changes confined to an upper, or lower pole calyx. Although the CT findings highlighted in our case are typical, the CT findings in XGP have a wide range of findings such as diffuse renal enlargement, renal atrophy, hydronephrosis, focal masses and air within the urinary tract.3,4 Due to the wide range of CT findings, differentiating XGP from renal tumors and abscesses on imaging can be challenging preoperatively. The definitive treatment of diffuse XGP is complete nephrectomy and resection of any involved tissue. Partial nephrectomy has only been shown to be of benefit in focal XGP.5
In conclusion, XGP is an uncommon form of bacterial pyelonephritis with a wide range of CT findings. The bear paw sign describes the classic appearance of dilated calyces with relative sparing of the renal pelvis. Awareness of the imaging signs in XGP can lead to earlier diagnosis and appropriate treatment.
Case Reports
Case reports will only be considered for unusual topics that add something new to the literature. All Case Reports should include at least one figure. Written informed consent for publication must accompany any photograph in which the subject can be identified. Figures should be submitted with a 300 dpi resolution when submitting electronically. The abstract should be unstructured, and the introductory section should always include the objective and reason why the author is presenting this particular case. References should be up to date, preferably not exceeding 15.
Acknowledgement
The CT images were reviewed by Dr Raja Rizal Azman.
Footnotes
Notice: Authors are encouraged to submit quizzes for possible publication in the Journal. These may be in any specialty, and should approximately follow the format used here (maximum of 2 figures). Please address any submissions to: Editor, Saudi Medical Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. Tel. +966 (11) 4777714 Ext. 42841.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.