


Abstract
Objectives: To determine pattern and impact of physical rehabilitation on dependency and functional performance of patients.
Methods: This retrospective chart review was carried out between July and August 2012 at King Abdulaziz Medical City, Jeddah, Saudi Arabia. Data were collected using demographic, clinical, and dependency assessment checklists.
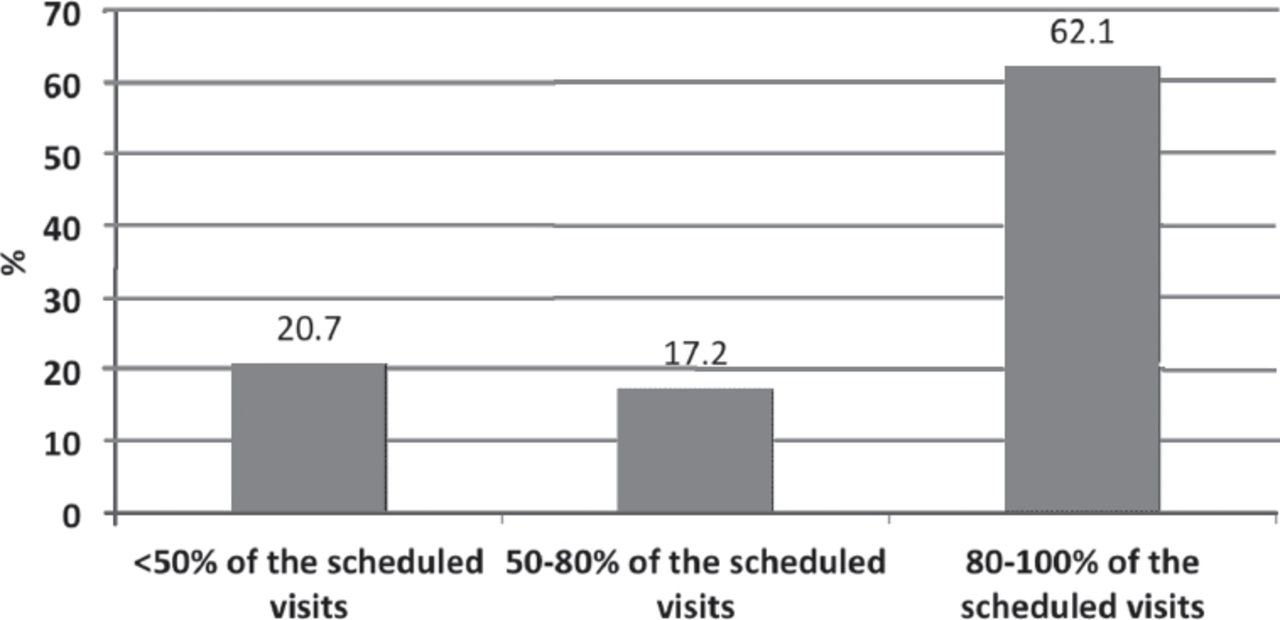
Results: Patients who underwent major lower limb amputations between January 2007 and April 2012 (n=121) were included in the study. There were 84 (69.4%) male and 37 (30.6%) female patients with a mean ± standard deviation of 63.3±17.4 years old. Diabetes mellitus was the most frequent cause in 63.6% of patients. Only one-third of the amputees (32.2%) have records of completion of their rehabilitation programs, although 20.7% of them completed the <50% of the scheduled rehabilitation sessions, 17.2% attended between 50% and 80%, and the remaining 62.1% attended more than 80% of the scheduled sessions. Muscle power scores in each side of the upper and lower limbs were significantly better following rehabilitation (p<0.0001). Basic functions of mobility and transfer have also significantly improved (p<0.05).
Conclusions: Overall dependency and functional performance were significantly better following implementation of the physical rehabilitation programs. A multidisciplinary team approach is mandatory to improve compliance of patients toward the rehabilitation programs.
Major lower limb amputation leads to losing the ability to move and to remain independent. It affects both physical and psychological well-being of patients. The main causes of major lower limb amputation include diabetes mellitus, vascular occlusive disease, trauma, and congenital deformities. Most commonly are due to vascular problems.1-3 Although more aggressive and improved vascular revascularization methodologies demonstrated decreases in amputation rates in some individual reports, identification of the high-risk populations, early detection, and proper risk management will remain the cornerstone for all attempts to reduce the incidence of non-revascularizable lower extremity vascular pathology requiring amputation.4
Rehabilitation programs are designed to restore mobility and regain an acceptable level of functioning. Functional outcomes of amputee patients have been reported to be associated with early rehabilitation intervention, adherence rate of the patients to rehabilitation,5 and level of the amputation.6 Other predictors include age of the patient, physical condition, and presence of comorbidities (cardiopulmonary diseases or diseases of the locomotor system).2,6,7 The available literature focused on prosthetic use, although integrated rehabilitation programs (community-based rehabilitation) that include patient education and periodic assessment of the prostheses and assistive devices showed better functional outcomes.8
The current study focused on determining patterns and impacts of the rehabilitation programs on dependency and functional performance of patients with major lower limb amputations in King Abdulaziz Medical City, Jeddah, Saudi Arabia.
Methods
This retrospective chart review was conducted between July and August 2012 at King Abdulaziz Medical City, western region (KAMC-WR) (a tertiary care healthcare facility with a 500-bed hospital). All medical records of patients with major lower limb amputations during the period from 2007 to 2012 were reviewed. No specific exclusion criteria were applied. Those patients included were National Guard military personnel and their families (father, mother, and siblings) who are eligible for services in KAMC-WR.
Data were collected using a checklist of demographic and clinical data (age, gender, comorbidities), amputation assessment (cause, type and date of amputation), and dependency assessment (namely, mobility and transfer, sitting and standing balance and ambulation if independent, assistive device, wheel chair, or bedridden) before and after the physical rehabilitation intervention.
This study was approved by the Institutional Review Board of King Abdullah International Medical Research Center, Jeddah, Saudi Arabia.
Statistical analysis
Data were collected and statistically analyzed using the IBM SPSS Statistics for Windows version 20.0 (IBMCorp, Armonk, NY, USA). Descriptive statistics including number, percent, mean, and standard deviation were used. Paired t test was used to compare mean scores of muscle power before and after rehabilitation. Chi square test or Fisher’s exact test were applied to compare association between mobility and transfer functions and degree of dependency. Level of significance was determined at p<0.05.
Results
The total number of patients who underwent major lower limb amputation between January 2007 and April 2012 was 121. The number of amputation cases was distributed by year as follows: 2007 (n=25), 2008 (n=18), 2009 (n=23), 2010 (n=21), 2011 (n=25), and April 2012 (n=9). There were 84 (69.4%) male and 37 (30.6%) female patients with a mean ± standard deviations age of 63.3 ± 17.4 years (range 15-95 years). Diabetes mellitus was the most frequent cause during the first amputation (Table 1). All amputations among diabetic patients were non-traumatic (Table 1). An equal percentage of patients had below and above knee amputation. Only one-third of the amputees received rehabilitation at King Abdulaziz Medical City Hospital (Table 1).
Demographic and clinical characteristics of 121 patients who underwent major lower limb amputation.
Figure 1 shows the compliance of patients with scheduled rehabilitation intervention sessions

Compliance of patients with scheduled rehabilitation intervention sessions at King Abdulaziz Medical City, Western Region, Saudi Arabia (n=39).
Among patients who received physical rehabilitation intervention at the study hospital (n=39), the mean muscle power score in each side of the upper and lower limbs was significantly better following rehabilitation (p=0.001) (Figure 2).

Muscle power scores in each side of the upper limbs (UL)and lower limbs (LL) before and after rehabilitation among patients who received rehabilitation (n=39) (p=0.001).
Table 2 summarized the percentage of patients who were able to perform the basic functions of getting up and down from the bed, rolling, lying to setting, sitting to standing, and bed to chair/chair to bed independently increased to more than double following rehabilitation. The degree of dependency statistically improved the following rehabilitation (p<0.05). The overall mortality among the studied patients following amputation was reported as 4% after 3 months and 20% after 3 years.
Patients perform different mobility and transfer functions independently, with assistance, or totally dependent before and after rehabilitation (n=27).
Discussion
This study showed an almost consistent number of patients who underwent major lower limb amputation throughout the years between 2007 and 2012. This consistency may not reflect the overall trend of amputation rates in Saudi Arabia because of the single-center experience and limited population served in the study hospital. Several studies in the Western countries showed decline in the overall amputation rates in the past 20-30 years.9-11 Factors contributed to the decline included early detection, frequent referral for diagnostic imaging, and the substantial advances in diagnostic modalities, peripheral vascular techniques, and endovascular technology. Socioeconomic status and access to care have been discussed and may affect the geographic variation of amputation rates in the United States.9-11
Diabetes mellitus continues to be the major risk factor associated with amputation among the studied population and previous similar studies.12 The prevalence of diabetes mellitus has been estimated to affect approximately one-third of the population in Saudi Arabia and according to the World Health Organization, it is estimated to double by 2030.13 The increasing trend in the incidence of diabetes mellitus in association with other factors (lack of early detection of peripheral artery disease) may add to the disease burden and affect rates of lower extremities amputations.
More than two-thirds of the amputee patients in the current study did not receive rehabilitation services following amputation and approximately 40% of those who underwent rehabilitation did not complete the scheduled services. Lack of rehabilitation services, or false lack due to the possibility that they received service in other hospital/center; however, this possibility is very unlikely as the rehabilitation services are provided for free for all eligible patients. In the meantime, rehabilitation completion rates might be also affected by the mortality and other postoperative complications.
The functional outcome data in the current study was collected based on physical therapy and rehabilitation notes, and follow-up history and examination in the vascular surgery clinics. It showed significant improvement of muscle power of the upper and lower limbs as well as the functional mobility and transfer following implementation of the rehabilitation program.
Ambulation is the main target of intervention programs following lower limb amputation;14 accordingly, when the ambulation could not be achieved, long-term interventions are required.15
A 5-year review of US patients revealed 7.5-year survival rates of 20% following above-knee amputation and 28% below-knee amputation operations.16 Previous studies17 in the United States showed a 26% mortality rate and 36% in Finland within one year following amputation. The overall mortality rate in the current study was 20% after 3 years. Similar to Carlos et al,4 the high mortality rates and poor survival probabilities observed are reflective of the multiple comorbidities seen in this population. Additionally, other factors may contribute to the increased mortality including what has been reported by Abou-Zamzam et al18 one-fourth of the amputees present to the attention of the vascular surgeon at very late stages into their vascular pathology with extensive gangrene or infection that precludes limb salvage. This study represents an experience of a cohort of patients with major lower limb amputations in a single hospital over a 6-year period.
Study limitations are related to the retrospective design and incomplete data in the medical records. Getting information from patients was also a challenge partly due to the unavailability of correct contact numbers of some patients, or inability of patients to recall rehabilitation service history. Further studies are needed to confirm and compare findings using wider prospective multicenter data that focuses on determining predictors of a wide range of functional outcomes following lower limb amputations (including physical, mental, and social characteristics of the patients and rehabilitation specific factors, such as duration, type).
In conclusion, diabetes mellitus was the most frequent cause of amputation. Only one-third of the amputees received rehabilitation at King Abdulaziz City hospital. Muscle power of the upper and lower limbs as well as independent performance of functions of getting up and down from the bed, rolling, lying to setting, sitting to standing, and bed to chair/chair improved significantly following rehabilitation interventions.
Improving awareness of patients and their caregivers and counseling on post-amputation goals would enhance patients’ compliance with the clinically decided rehabilitation programs. A multidisciplinary team approach and in-depth understanding of the functional consequences of amputation and systemic and detailed consideration of the patients and their environment should be the basis for the post-amputation follow up programs.19
Acknowledgment
This study was conducted as part of the Students’ Research Summer School at King Abdullah International Medical Research Center, Jeddah, Saudi Arabia.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 31, 2016.
- Accepted July 29, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.