


Abstract
Objectives To assess the clinical role of flat-panel cone beam CT (CBCT) in performing percutaneous needle biopsy (PNB) of bone lesions. Flat-panel cone beam CT systems have been used as a guidance tool for performing percutaneous biopsy. Real-time fluoroscopy and virtual navigation systems help simplify needle path planning and shorten procedure times.
Methods From March 2012 to March 2016, 80 patients with 80 bone lesions were retrospectively enrolled in the study in Zhengzhou city of China. Technical success, diagnostic accuracy, puncture performance, procedure time, complications, and effective radiation exposure were calculated.
Results All biopsies were technically successful (100%). Sufficient tissue for histopathological analysis was obtained in 75 of 80 cases. The sensitivity of PNB of bone lesions was 95.5%, the specificity was 83.3%, and accuracy was 93.7%. The mean scoring of puncture performance was 3.9 ± 1.3. The mean total procedure time was 13.20 ± 4.4 min, resulting in a mean exposure dose of 11.3 ± 5.1 mSv. The complication rate was 8.7%.
Conclusion Percutaneous bone biopsy using CBCT is a safe and effective method that simplifies needle path planning and shortens procedure times.
Accurately diagnosing bone tumors is crucial because appropriate treatment varies according to pathological type.1 However, current imaging techniques are not yet able to accurately diagnose bone lesions, and surgical biopsies are costly and traumatic to patients. Currently, ultrasound or computed tomography (CT)-guided percutaneous needle biopsy (PNB) is becoming popular for its convenience and accuracy.2-4 However, conventional CT guidance has limitations given its lack of real-time monitoring and gantry tilting for a more accessible needle pathway to the target lesion. Along with the development of cone beam CT (CBCT), a novel technique for PNB has recently emerged. It combines advanced real-time fluoroscopy and virtual navigation functions, which simplifies needle path planning and shortens procedure times, and reduces exposure dose and complications, while enhancing diagnostic accuracy.5 Cone beam CT-guided PNB of mediastinal lesions, pulmonary nodules, lumbo-sacrum, and cervical bone have been reported.6-8 The purpose of this study was to evaluate the diagnostic accuracy of CBCT-guided PNB in bone tumors.
Methods
Given the retrospective nature of the study and the use of anonymized data, requirements for informed consent were waived. This study was conducted in accordance with Declaration of Helsinki. The inclusion criteria were patients being able to tolerate this mini-invasive procedure. The exclusion criteria were patients who combined with severe cardiopulmonary failure or coagulation dysfunction. After institutional review board, approval was obtained from the authors’ hospital, a total of 80 patients (43 male, 37 female; mean age 49.00±12.21 years, range 15- 77 years) with 80 lesions were retrospectively enrolled from March 2012 to March 2016 from the authors’ department (Table 1). All patients underwent enhanced CT or MRI to confirm musculoskeletal lesions. Before the biopsy procedure, a history of bleeding diathesis, coagulation parameters, including platelet count, partial thromboplastin time and prothrombin time, were evaluated. After the operation, all patients were asked to stay at the hospital for 24 hours.
Lesion characteristics and procedure records.
All PNBs were performed under local anesthesia in supine or prone positions according to the location of the lesion and the large vessels, as well as the surrounding structures. A 13- or 16-gauge needle, and 16-gauge semi-automatic biopsy gun (Quick-Core, Cook Medical Inc, Bloomington, IN, USA), were used. Before biopsy, a pre-procedural scan under CBCT was performed to identify the safest and best access to the target lesion, avoiding obstruction and reducing distance. After each 8 DR scan, CBCT images were transferred to a detailed medical imaging workstation, where the most safe and effective skin puncture points and needle pathways could be calculated. After the virtual navigation system was adjusted, the needle was advanced along the planned path into the target lesions, with the help of x-ray film and virtual color overlap (Figures 1 & 2). Percutaneous needle biopsys were performed by one highly experienced bone radiologist and under the supervision of one chest radiologist (Han XW, 30 years’ experience in image-guided PNB). After biopsy, post-procedure CT images were acquired to identify procedure-related complications.

The hole procedure of percutaneous biopsy of a L1 bone lesion in a 70-year-old man. A pre-procedure cone beam CT (CBCT) scan was carried out, the lesion was marked with a circle and a cross; a) axial view; b) sagittal view. Laser crosshair projected on the skin and the fixed lever placed around the needle to aid in laser alignment in the bull`s-eye view; c) The real-time fluoroscopy could help us to check the needld path; d) The planned needle path (in white) was overlaid on real-time fluoroscopy; e) The needle was aligned and inserted at the skin entry site using the bull`s-eye view; f) Another CBCT was carried out to ensure the needle located within the lesion.

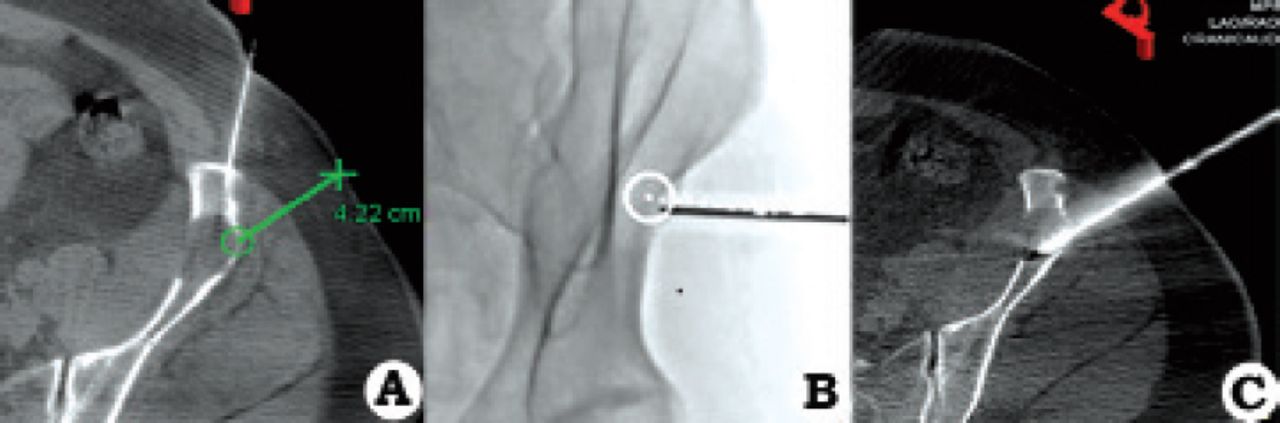
Percutaneous biopsy of the left iliac bone lesion in a 55-year-old woman. a) Located the shortest distance before the procedure in the sagittal plane. b) The planned needle path (in white) was overlaid on real-time fluoroscopy. c) An updated cone beam CT (CBCT) acquired with collimated field of view confirmed the placement of the needle near or within the lesion in axial plane. (Please refer to this Figure in the Text)
The puncture time was defined as the time between the first scan and the completion of the procedure. Technical success was defined as appropriate localization of the biopsy needle within target nodules on procedural CBCT images and adequate tissue sampling on visual inspection. The puncture performance level was assessed using the following method: unsuccessful puncture scored 1; successful puncture with >4 needle repositionings or reinsertions (adjustments) scored 2; with 3-4 adjustments scored 3; with 1-2 adjustments scored 4; and without needle adjustment scored 5.
Benign PNB results were considered to be true negative if the target lesion did not receive any treatment, or the size of the lesion remained stable or reduced by ≥20% in the CT examination 6 months later, or surgical resection specimens exhibited certain benign diseases such as fibrosteoma or chondroma. Conversely, if the PNB result was benign and surgical excision of the specimen was malignant, this condition was termed false negative. Percutaneous needle biopsy-related complications consisted of small hematoma(s) and mild pain.
Statistical analysis
All data analyses were performed using Excel 2010 (Microsoft Corporation, Redmond, WA, USA) and the Statistical Package for the Social Science (SPSS) version 19.0 (IBM Corp., Armonk, NY, USA). Numerical data are reported as mean ± standard deviation.
Results
Lesion and procedural records
A detailed description of the lesion characteristics and procedure records is summarized in Table 1. The mean maximum lesion diameter was 3.7±2.4 cm. Among the 80 nodules, 70 lesions were osteolytic, 8 were sclerotic, and 2 were mixed. Thirty-two lesions were vertebral, 13 were located in the leg, 11 were in the pelvis, 10 in the sternum, 8 in the ribs, and 6 in the arm. The mean number of biopsies was 2.4±1.2 and CBCT acquisitions were 3.0 ± 1.1. The mean total procedure time was 13.2±4.4 min. During the entire process, the mean effective exposure dose was 11.3±5.1 mSv.
Pathological results
Detailed pathological results are summarized in Table 2. Among the 80 nodules, 65 were malignant, 10 were benign, and 5 lacked sufficient tissue for diagnosis. The 65 malignant tumors consisted of 19 osteosarcoma, 15 chondrosarcoma, 4 leiomyosarcoma, 3 angiosarcoma, 6 fibrosarcoma, and 18 metastatic tumor. The final diagnosis of malignancy was made on the basis of surgical pathology (n=36), specific malignant biopsy results (n=8), and symptoms of advanced stage or distant metastasis receiving local radiation and chemotherapy (n=21). Among the benign tumors, 5 were giant cell tumors, 2 were fibromas, and 3 were aneurysmal bone cysts. Diagnosis of the benign tumor was made according to surgical pathology (n=4), follow-up observation (n=6). These lesions did not receive any treatment; however, the size of the lesion remained stable or was reduced by ≥20% in the CT examination 6 months later. Accurate pathological diagnosis was not possible in the remaining 5 lesions because of inadequate or unspecific tissue, with results exhibiting necrotic bone and blood clot. To verify the characterization of these bone lesions, surgical bone biopsy was performed several days after PNB. The pathology results revealed that 3 of 5 were malignant (2 angiosarcoma, 1 leiomyosarcoma), the remaining 2 were benign (aneurysmal). The final correct diagnosis rate was 93.7%, and the sensitivity of PNB of bone lesions was 95.5%, specificity was 83.3%, and accuracy was 93.7%.
Pathologic outcomes.
Complications included small hematoma and mild pain, occurring in 7 of 80 (8.7%) procedures. The symptoms disappeared after local compression was applied and pain relief drugs were administered within 24 h (Table 3).
The accuracy and complication rate of PNB procedure.
Discussion
Percutaneous needle biopsy is conventionally performed under CT or x-ray fluoroscopic guidance, which has been shown to be safe, accurate, and effective in targeting lesions with high diagnostic yield.9,10 However, these imaging techniques have many drawbacks including lack of real-time surveillance or 3-dimensional imaging.
Cone beam CT technologies can offer excellent visualization of the target lesion and surrounding tissue, provide a virtual pathway for needle approach to the target lesion, and facilitate navigation of the needle into the target. Cone beam CT-guided PNB has been applied in many areas for its high diagnostic yield, short total procedure time, low exposure dose, and minimal rate of complications in mediastinal lesions, pulmonary nodules, the lumbosacrum, cervical bone, and adrenals.11
Our study demonstrates that the technical success rate of PNB under this CBCT virtual navigation system was 100.0%, which corresponds to the rate reported by Tselikas et al,12 who investigated bone biopsy under CT and CBCT (both 100%). In our study, sufficient tissue for histopathological analysis was obtained in 93.7% of lesions. The mean total procedure time was 13.20±4.4 min (range 8-32 min), which was in sharp contrast to the median puncture time of 32-91 min using CT-guidance reported in other studies.13
The effective mean exposure dose was 11.3±5.1 mSv, which is lower than the dose for musculoskeletal procedures (14.7 mSv-19.2mSv) reported before. In our study, no serious complications occurred, either vascular or nerve injuries. There were no tumor recurrences along any biopsy pathway, only small complications such as hematomas and mild pain.
A major drawback of our study was its retrospective design. Additionally, the limited number of certain patient subgroups, such as those with primary or metastasizing tumors. However, our investigation was an observational research project, and we lacked comparative data. Finally, the resolution ratio of CBCT was lower than spiral CT with high-resolution. Motion artifacts produced by respiration or slight body movement cannot be ignored.
In conclusion, this study illustrates the promising potential of CBCT virtual navigation systems to diagnose bone lesions. It is now a better choice to perform bone biopsies under FP-CBCT guidance considering its safety and validity, and lower radiation exposure. We expect that with increased experience, more task-specific protocols and larger sample sizes, the effective radiation dose and procedure times for software-assisted cases will decrease even more in the near future.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 14, 2017.
- Accepted March 7, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.