


Abstract
Objectives: To test the hypothesis that identification and blockade of the intercostobrachial nerve (ICBN) can be achieved under ultrasound (US) guidance using a small volume of local anesthetic.
Methods: Twenty-eight adult male volunteers were examined at King Khalid University Hospital, Riyadh, Kingdom of Saudi Arabia from November 2012 to September 2013. Intercostobrachial nerve blockade was performed using one ml of 2% lidocaine under US guidance. A sensory map of the blocked area was developed relative to the medial aspect of the humeral head.
Results: The ICBN appears as a hyper-echoic structure. The nerve diameter was 2.3±0.28 mm, and the depth was 9±0.28 mm. The measurements of the sensory-blocked area relative to the medial aspect of the humeral head were as follows: 6.3±1.6 cm anteriorly; 6.2±2.9 cm posteriorly; 9.4±2.9 cm proximally; and 9.2±4.4 cm distally. Intercostobrachial nerve blockade using one ml of local anesthetic was successful in all cases.
Conclusion: The present study described the sonographic anatomical details of the ICBN and its sensory distribution to successfully perform selective US-guided ICBN blockade.
The intercostobrachial nerve (ICBN) is a pure sensory nerve that arises primarily from the second intercostal nerve (T2) with occasional contribution from T3. Therefore, ICBN is not a component of the brachial plexus and is not anesthetized by brachial plexus blockade. In its extra-thoracic course, the ICBN runs parallel to the axillary vein at a distance of approximately 1.5 cm in a vertical dimension and provides sensory supply to the axilla, upper medial arm, and a small area at the upper lateral chest.1,2 Clinically, ICBN blockade is necessary for any surgical procedure where the surgical incision extends into the axilla, or upper medial arm.3 Selective ICBN blockade techniques have not been described in the literature; only the subcutaneous ring infiltration to block nerve endings has been referred to.4 Ultrasound (US) has proven to be a valuable tool for direct identification of small nerves, such as the medial antebrachial cutaneous nerve of the forearm, and great auricular nerve.5,6 Consequently, the ICBN can also be identified by US. We designed a prospective, volunteer study to describe a technique for US visualization and guided blockade of the ICBN followed by the mapping of its sensory skin supply. Our objective in presenting this particular study is to highlight the feasability of accurately identifying small nerves, such as ICBN using US technology.
Methods
After receiving approval from the institutional review board, informed written consent was obtained from all volunteers prior to their recruitment. Thirty-nine hospital staff members were interviewed, and 11 staff members were excluded according to the exclusion criteria of the study. Inclusion criteria were as follows: adult male patients; body mass index <30; and agreed and consented to US examination with subsequent blockade of the ICBN. Exclusion criteria were as follows: history of allergy to local anesthetics; previous surgery, at or near the site of study; pre-existing neurological disease; and patients on anticoagulant therapy, or with a history of coagulopathy. The study included 28 volunteers at the King Khalid University Hospital, Riyadh, Kingdom of Saudi Arabia who were recruited from November 2012 to September 2013. All of the volunteers underwent US identification and subsequent blockade of the ICBN.
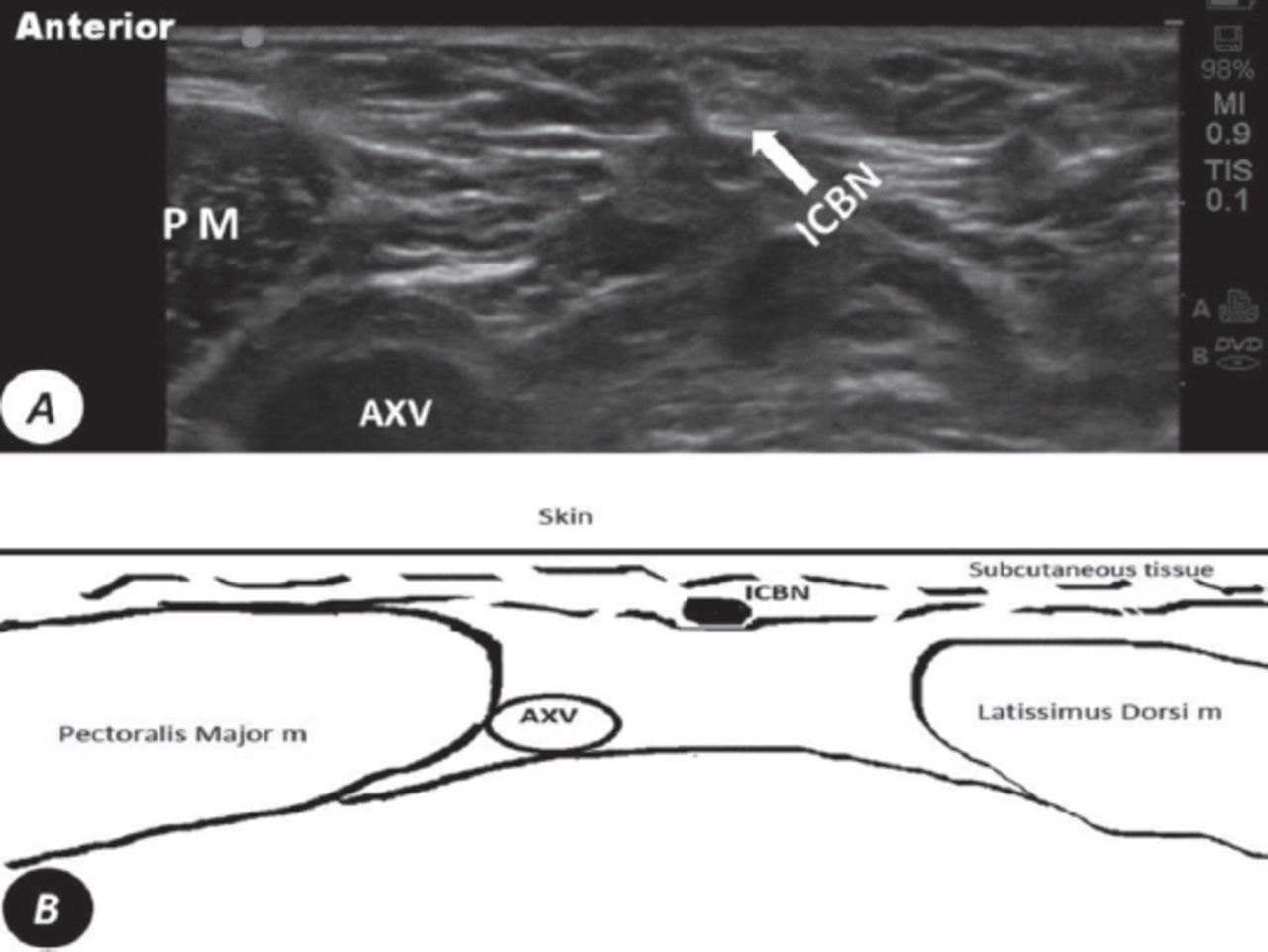
On the day of the study, volunteers were admitted to the block room, and an intravenous line was established. Each volunteer was placed in supine position with the arm abducted and elevated above the head level. A US scan was performed using a 6-15 MHz, 50-mm linear probe (Sonosite M-Turbo; Sonosite Inc., Bothell, WA, USA). The probe was positioned at the apex of the axillary fossa to scan the axillary vein in the short axis view. The depth on the US screen was set to 2.7 cm. The US probe was slid proximally toward the base of the axilla, at a distance of approximately 6 cm proximal to the medial aspect of the humeral head (Figure 1), and the axillary vein became deeper on the US screen and inferior to the postero-lateral border of the pectoralis major muscle (Figure 2A). The probe was then positioned slightly oblique, and the depth on the US screen was reduced to 1.5 cm for clear identification of the nerve in the cross-sectional view. At this point, the ICBN appeared as a hyper-echoic oval structure surrounded by a fascial split, superior and posterior to the axillary vein, midway on an imaginary line crossing the borders of the pectoralis major and latissimus dorsi muscles as illustrated in Figure 2B. Releasing the pressure applied on the US probe frequently revealed small, hypoechoic, rounded collapsible vessels anterior or posterior to the nerve. The pressure on the probe was reapplied. The area of interest was zoomed, and the US built-in measuring tool was used to measure the horizontal nerve diameter and its depth, in addition to the distance from the nerve to the axillary vein, and from the nerve to the lateral border of the pectoralis major muscle. The medial aspect of the humeral head was identified, and the midpoint on the skin covering this anatomical landmark was marked with a surgeon’s marker pen (Medical Action Industries, Inc., Arden, NC, USA). The point was labeled as humeral head (HH), and the distance from the nerve to the HH point was measured using a measuring tape. Subsequently, the nerve was traced toward its distal end as it became more superficial, and divided into 2 or 3 smaller branches.

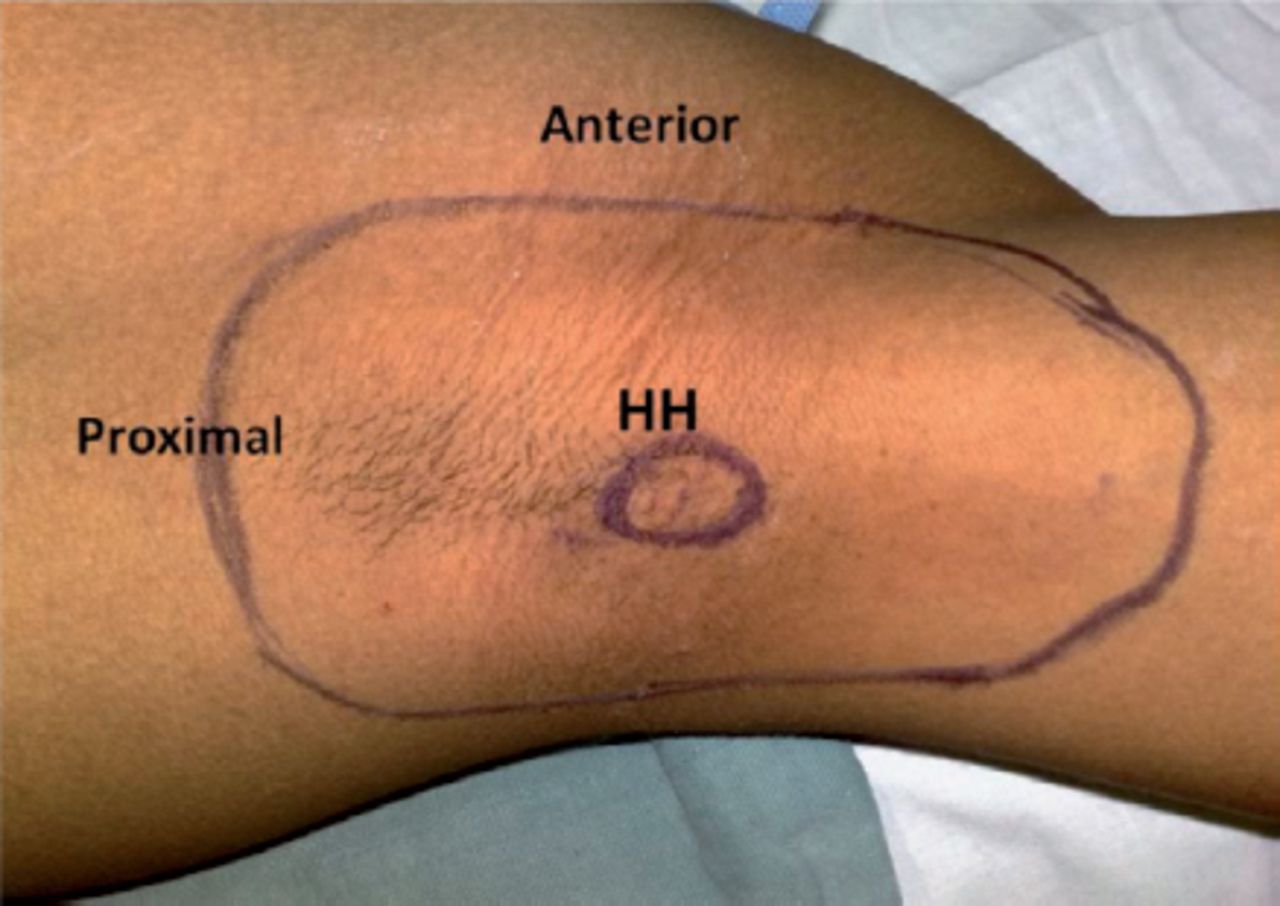
Simulation of ultrasound probe and needle position for in-plane intercostobrachial nerve block technique. Midpoint on the skin covering the medial aspect of the humeral head (HH). The curved line denotes the lateral border of the pectoralis major.
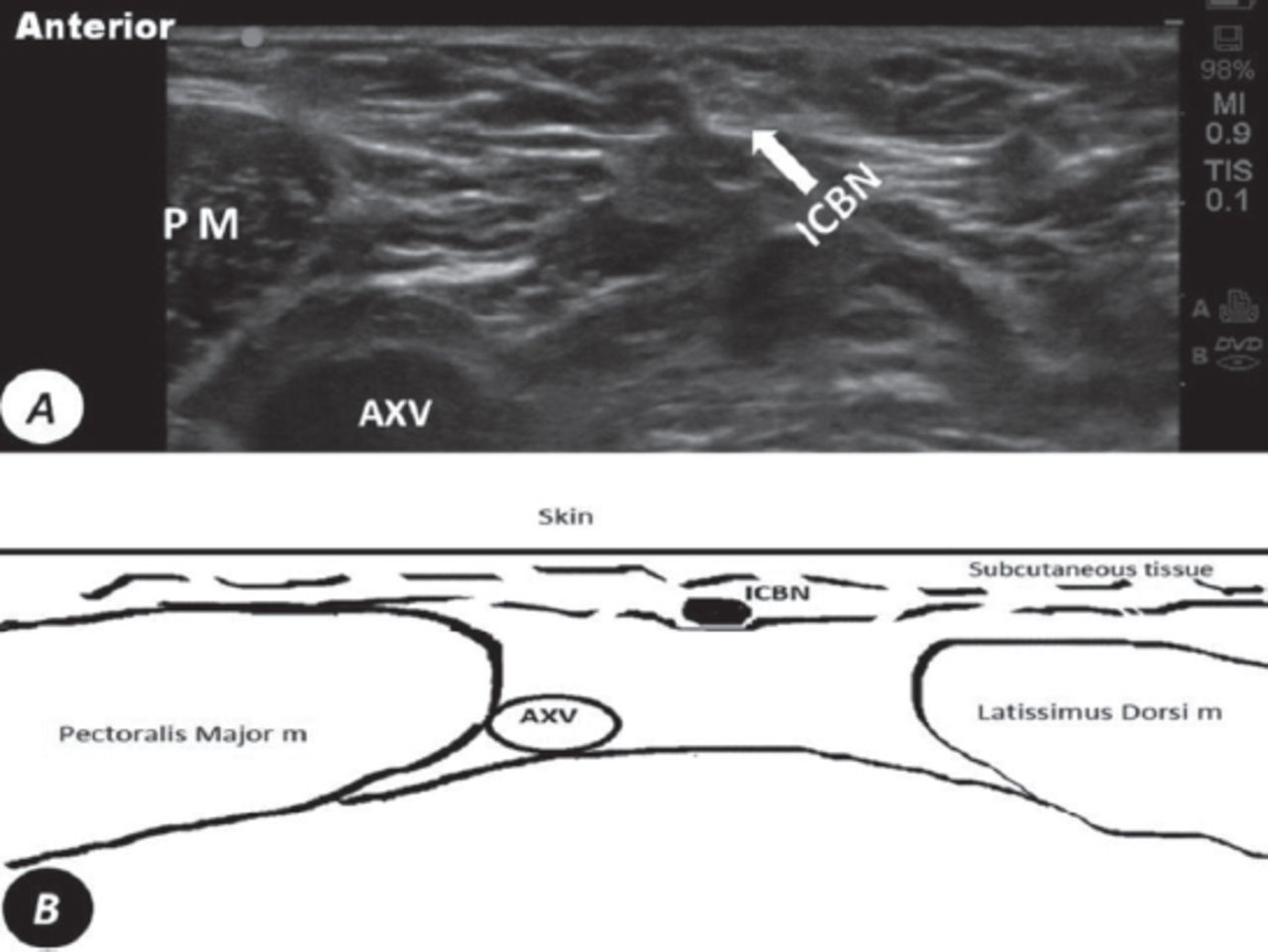
A) Ultrasound short axis view at the base of the axillary area shows the intercostobrachial nerve (ICBN) as an oval shaped hyper-echoic structure posterior to lateral border of the pectoralis major muscle, superior, and posterior to the axillary vein (AXV). B) Diagram of short axis view at the base of the axillary area. PM - pectoralis major muscle
After surgical disinfection of the axillary area and sterile preparation of the US probe, blockade of the ICBN was performed with a pre-filled, 22-gauge, 50-mm facet tip needle (Pajunk, Geisingen, Germany) using an in-plain technique. After negative aspiration, one ml of lidocaine 2% (Hospira, Inc., Lake Forest, IL, USA) was injected under direct US visualization, and the local anesthetic that encircled the nerve was visualized. All of the blocks were performed by the same anesthesiologist. Sensory blockade was assessed by another investigator every 2 minutes for the first 10 minutes. The onset of the block was determined by loss of cold sensation at the skin of the axillary area. The blocked area was tested using a pinprick and compared with the contralateral side. The sensory block was graded on a scale from 0 to 10, with “0” representing complete absence of sensation and “10” representing no difference compared with the other side. Finally, a sensory map was drawn relative to the marked point HH, which represents grade 0 on the scale, indicating a complete sensory blockade. Twenty-four hours after performance of the ICBN block, the sensory integrity of the particular area was re-tested and compared with the contralateral side, and the puncture site was investigated for signs of hematoma and infection.
Results. Twenty-eight male volunteers were included in the study analysis. The mean (±standard deviation [SD]) age was 35±12 years and body mass index was 24.6±3 kg/m2. Ultrasound visualization of the ICBN was possible in all cases. The mean horizontal nerve diameter was 2.3±0.28 mm, and the mean depth was 9±0.28 mm. The nerve was located superior and posterior to the axillary vein at a point where the axillary vein approached the posterolateral border of the pectoralis major muscle. The mean distance between the nerve and axillary vein was 1.48±0.17 cm. The nerve was visualized posterior to the lateral border of the pectoralis major muscle at a mean distance of 1.7±0.54 cm. The nerve was located 5.6±1.4 cm proximal to the HH point. Blockade of the ICBN was successful in all volunteers. Comparing the sensory block distribution of all the volunteers revealed a constant sensory-blocked area relative to the HH point as follows: 6.3±1.6 cm anteriorly, 6.2±2.9 cm posteriorly, 9.4±2.9 cm proximally, and 9.2±4.4 cm distally with the arm in the abduction elevation position. Figure 3 illustrates an example of the sensory distribution of a successful ICBN block. We did not detect any related side effects, such as hematoma, infection, or persistent numbness within 24 hours after the nerve blockade.

Illustration of a case of a sensory block distribution 10 min after intercostobrachial nerve blockade. Midpoint on the skin covering the medial aspect of the humeral head (HH).
Discussion
This study describes the sono-anatomy of the ICBN with subsequent blockade of this small sensory nerve under real-time US guidance. We could show that US visualization of the ICBN within a fascial pocket was possible in all cases. The ICBN can be blocked together with other nerves, such as the pectoral, intercostal, and long thoracic nerves in a recently described technique named PECS II. This new block inspired by the infraclavicular brachial plexus block approach and the transversus abdominis plane blockade requires a relatively large volume (35 ml) of local anesthetic.7 Axillary subcutaneous infiltration to peripherally block the ICBN endings remained the most popular approach. This approach involves the injection of 5-10 ml of local anesthetic subcutaneously, forming a wheal along the axillary crease from the anterior head of the deltoid muscle to the long head of the triceps muscle.4 However, the above mentioned techniques cannot be labeled as selective blocks of the ICBN and require a large volume of local anesthetic. Selective ICBN blockade can be useful for the identification and treatment of the nerves involved in the neuropathic pain syndrome following surgery involving the breast and the axillary areas.8
A recent systematic review9 found 7 studies related to the neural blockade to treat neuropathic pain after breast surgery, but none of these studies focused on the ICBN blockade. These finding highlights the feasability of identifying the small nerve, such as ICBN, using US.
We learned from our earlier experience that small nerves can be visualized using US, and that successful blockade is feasible; the operator should rely on prominent anatomical sono-landmarks. The identification of the axillary vein and lateral border of the pectoralis major muscle, and more importantly, the relationship between the above 2 anatomical structures, are required to localize the potential area of the ICBN. The ICBN is best identified where the axillary vein approaches the lateral border of the pectoralis major muscle. Additionally, dynamic images are more helpful than static ones. Because the US probe was moved toward the apex of the axilla, the nerve fibers are divided into smaller branches running on a more superficial plane. Moreover, the ICBN either passes near or crosses over the axillary lymph node,10 and the dynamic image in such a case is a more reliable method to outline the ICBN from the neighboring structures.
The operator should consider the superficial course of the ICBN in the axillary fossa and not confuse it with other nerves running at a deeper plane, such as the long thoracic and thoracodorsal nerves. The blocked sensory area had a semi-rounded shape and was distributed around the medial aspect of the humeral head; therefore, to obtain an informative map, we chose this anatomical bony landmark to be the center of the ICBN sensory map. Moreover, many volunteers experienced a numbed area reaching distally along the medial upper arm, but we chose to map the area graded as “0” on the sensory scale only. The volunteers in this study were all males and had a normal or low body mass index; therefore, our observation might not be accurate for patients with a higher body mass index or who are female.
In conclusion, our results showed that US can be used reliably to visualize the ICBN, and the injection of one ml of local anesthetic under direct US visualization can successfully block the ICBN; therefore, this technique can be used as a supplemental block for upper limb anesthesia. We recommend further studies to support and apply these findings to improve patient care.
Related Articles
Degirmenci NA, Ozakyol AH, Atlanoglu S, Akcan E, Susuz S. Increased incidence of abnormal reflux flow in lower extremity veins of cirrhotic patients by Doppler ultrasonography. Saudi Med J 2013; 34: 276-281.
Wang YH, Zheng QC, Yuan GX, Ren JH. The application of ultrasound B-flow imaging in detection of carotid atherosclerotic micro-vessel with ischemic cerebrovascular disease. Saudi Med J 2012; 33: 1080-1086.
Al Bannay RA, Husain AA. Role of tissue Doppler imaging in assessing left ventricular diastolic dysfunction severity. Does it hold the same ability? Saudi Med J 2012; 33: 34-38.
Raddaoui EM. Endoscopic ultrasound-guided fine needle aspiration in the evaluation of pancreatic neuroendocrine neoplasms. Saudi Med J 2010; 31: 1271-1273.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 5, 2015.
- Accepted August 20, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.