


Abstract
Objectives: To assess duplex ultrasound (DUS) parameters, and predicti the outcome of varicocele ligation in male infertility.
Methods: This retrospective and follow up study was conducted at Dr. Sulaiman Al Habib Hospital, AlQassim, Saudi Arabia between January 2011 and December 2012. Eighty-two patients were selected, who presented with clinical/subclinical varicocele and male infertility. All these patients had DUS of the scrotum and underwent for low ligation varicocelectomy. These patients were followed for a period of 12-24 months after surgery for the occurrence of paternity. We reviewed pre-operative scrotal DUS of these 82 patients for the testicular size and volume, pampiniform veins caliber and duration of reflux in the dilated veins at rest, and after valsalva maneuver. These DUS parameters were correlated with the postoperative paternity rate.
Results: Postoperative paternity was achieved in 18 patients (31.6%) with normal-sized testes, and in 3 patients (12%) with small size testes. The positive paternity rate was higher (38.5%) in patients with clinically detected varicocele, compared with only 16.7% of patients with subclinical varicocele (detected by ultrasound only). In addition, postoperative paternity was significantly higher in patients with bilateral varicocele (70.6%), with shunt-type varicocele (71.4%), and patients with a permanent grade of venous reflux (62.5%).
Conclusion: Selection of patients for the successful paternity after varicocele repair depends mainly on DUS parameters, which includes normal size testicles with shunt type of bilateral varicocele and continuous reflux.
Varicocele is defined as dilatation of the pampiniform venous plexus draining the testes. It is much more common on the left side compared with the right side, owing to long length of left testicular vein, the acute angle of insertion of left testicular vein into the left renal vein, lack of effective anti-reflux valves, which may transmit the high pressure of renal vein, making left testicular vein more vulnerable to varicocele.1,2 Varicocele is the most frequently identified male factor for infertility, present in up to 40% of cases. Long duration persistent varicocele is associated with adverse effects on sperm count, sperm motility and morphology, decrease testicular size, abnormal testosterone hormone level and decrease pregnancy rates.3-5 Scrotal physical examination is the preferred method for the diagnosis of varicocele. The Dubin grading system classifies the varicocele into 3 grades. Grade 1: varicocele is visible and palpable at rest; Grade 2: varicocele is palpable, but not visible; and Grade 3: varicocele is palpable only during valsalva maneuver. Duplex ultrasound (DUS) allows accurate diagnosis of varicoceles, even subclinical varicocele, which is not apparent on physical examination. Duplex ultrasound is performed at rest and during Valsalva maneuver.6,7 The scrotal vessels are assessed for the degree of dilatation, augmentation and direction of flow during Valsalva and duration of reflux. In this way, CDU is helpful to select the patient for varicocele repair.8-11 Many studies following varicocelectomy have reported approximately 66-70% improvement in semen parameters and 40-60% of patients have increased conception rates.12-15 Although, the outcome and prognosis after varicocelectomy are still controversial, and there are many preoperative parameters that determine the probability of success of the operation.16-18 There is a great need for research to improve preoperative selection of patients with varicocele. This study was carried out to assess the DUS (DUS includes grey scale ultrasound and color doppler ultrasound) parameters including the testicular size, degree of varicocele, type, and duration of reflux that could predict the outcome of varicocele repair in terms of paternity.
Methods
Selection of patients
Literature search was carried out by internet websites such as PubMed and Google scholar. This is a retrospective study carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki as revised in Tokyo 2004) for humans and was approved by the local Ethics Committee of the College of Medicine, Qassim University, AlQassim, Saudi Arabia, between January 2011 and December 2012. We searched the files of patient who visited Dr. Sulaiman Al Habib Hospital, Qassim region of Saudi Arabia for the evaluation and management of male infertility.
We traced the records of 225 male patients between 23-47 years of age, who underwent for scrotal sonography and color-doppler ultrasound (Duplex Ultrasound, DUS) for male infertility with unilateral/bilateral varicocele. Out of these, 33 patients with female partners who have had infertility factor were excluded from this study. Ninety patients with associated scrotal/testicular diseases such as epidydimal cyst, spermatocele, hydrocele, testicular cyst, epididymo-orchitis, and so forth were also excluded from the study.
The remaining 102 patients were questioned for the male infertility with abnormal semen analysis (oligospermia, azospermia, asthenospermia) without female infertility and diagnosed clinically with unilateral/bilateral varicocele as well as by DUS, and without any associated scrotal/testicular diseases were included in this study. Of these, 92 patients underwent varicocelectomy by using a low ligation technique with sub-inguinal approach by a senior consultant urologist from our hospital. Eighty-two patients were followed up after the varicocele ligation for an average period of 12-24 months to determine the paternity after the varicocele repair.
Imaging interpretation
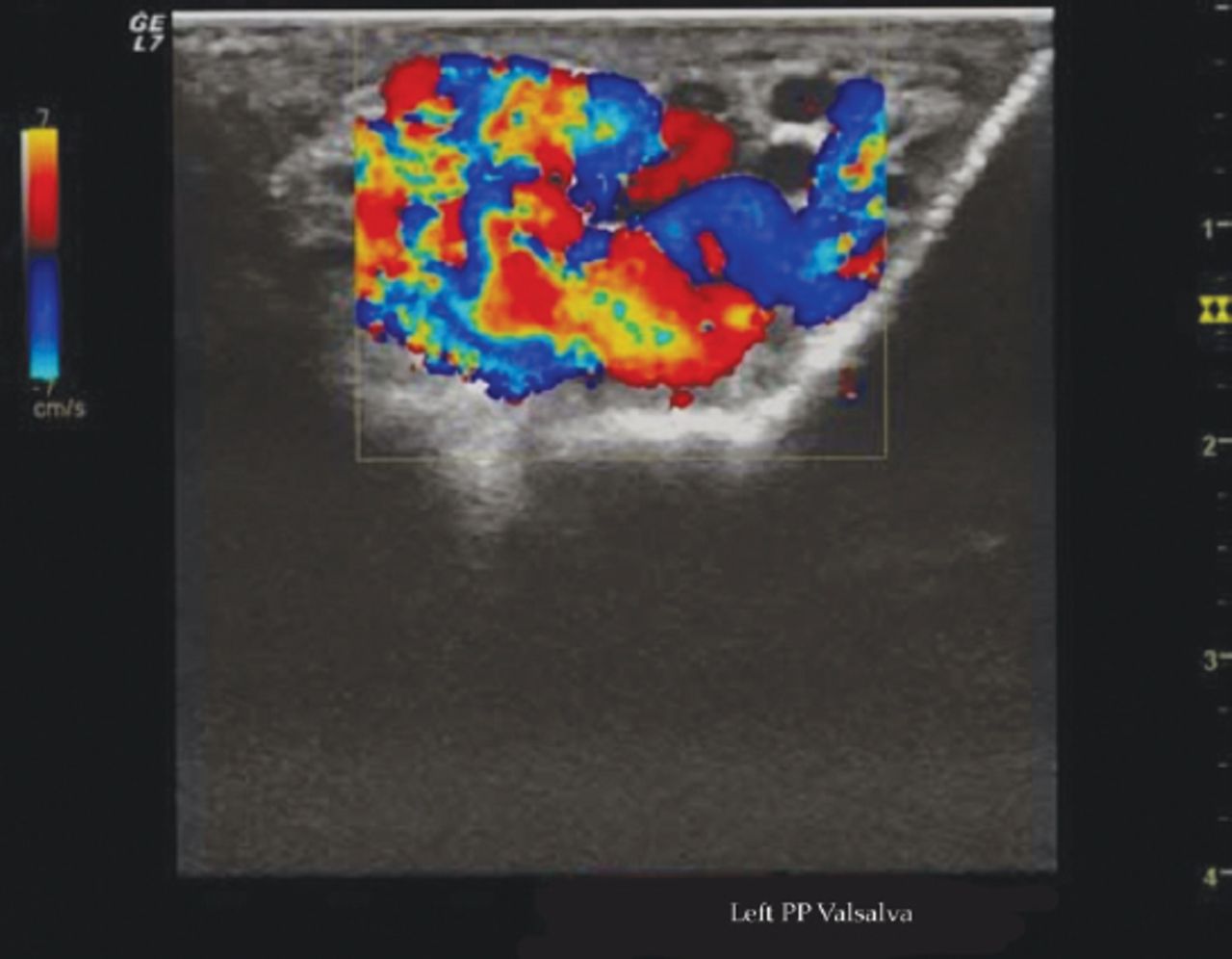
The records of all patients shows that the DUS of the scrotum were performed in the radiology department by 2 senior radiologists with at least 10 years of experience. The patients were scanned with the linear high-frequency (7 MHz) transducer using LOGIQ-9 (GE) (General Electronics (GE), New York, USA) ultrasound machine and sagittal, and transverse images were obtained. Additional views were also obtained in coronal and oblique planes with the patient being supine and upright positions, after performing the Valsalva maneuver (Figure 1).

Color Doppler ultrasound of the scrotum showing dilated left pampiniform venous plexus with augmentation after Valsalva maneuver.
Both the testes were assessed for the presence, size, and volume with grey scale ultrasound.19 The volume of each testis was calculated by: length x width x anteroposterior depth x 0.53 = volume in cubic centimeters. The pampiniform venous plexus were evaluated at the lateral, posterior, and superior aspect of testes, leading towards inguinal canal.20 The dilated veins appeared on grey-scale ultrasound as numerous, tortuous, and tubular channels in the peri-testicular regions measuring >2.5 mm in diameter at rest, and increased in size on straining (Valsalva maneuver) were recorded as varicocele. Veins which measured <2 mm were recorded as normal. The grades of varicocele are shown in Table 1.
Grades of varicocele.
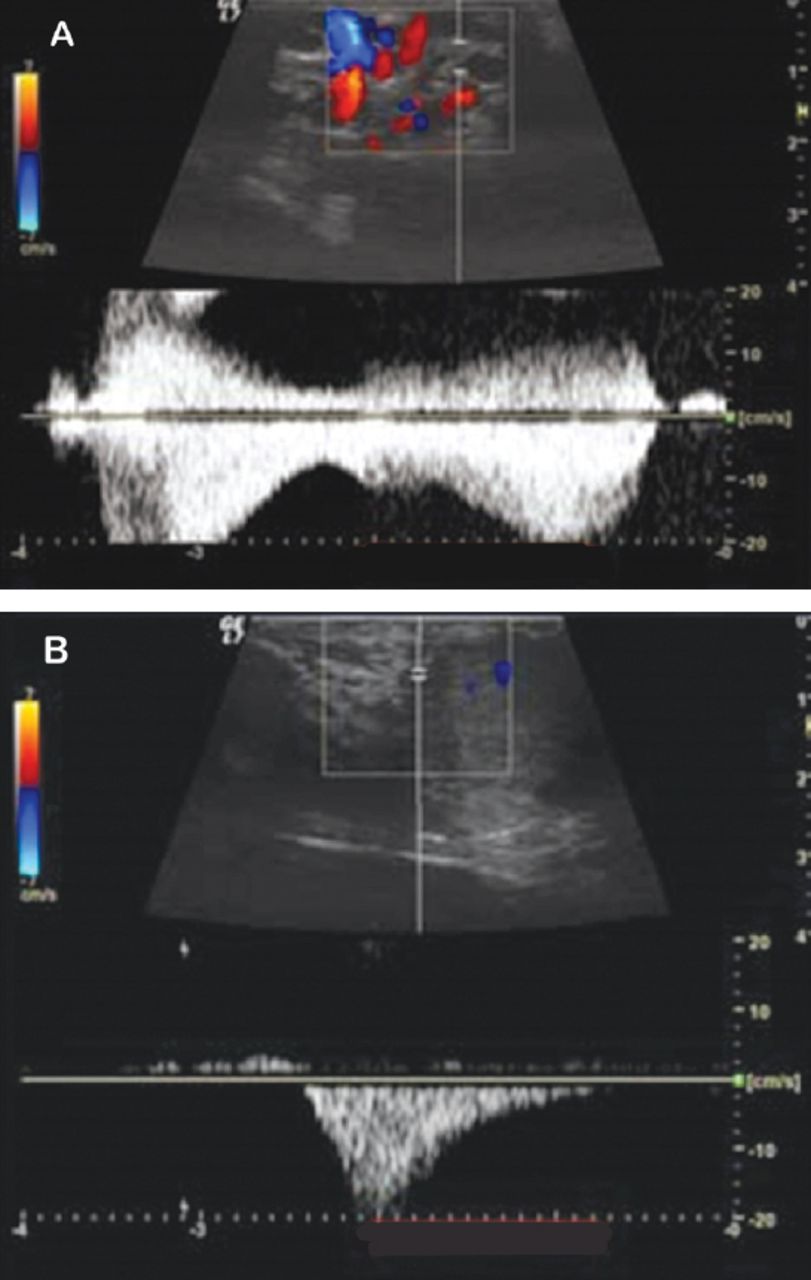
The degree of venous reflux at Valsalva maneuver was quantified as brief reflux lasting >1 second, moderate reflux lasting 1-2 seconds and continuous/permanent reflux lasting >2 s seconds.21 On the basis of color Doppler sonographic findings, varicocele was classified hemodynamicaly into 2 different types: Shunt type and stop/pressure type.22 Shunt-type varicocele showed continuous reflux during Valsalva in both retrograde and orthograde directions (Figure 2A). The stop/pressure type varicocele showed short phase of initial retrograde flow during Valsalva maneuver (Figure 2B).

Color Doppler ultrasound in 2 different patients showing types of varicocele with spectral analysis. A) Stop type varicocele showing retrograde flow only. B) Shunt type varicocele showing retrograde and orthograde flow.
Statistical analysis
Data was computed and analyzed by using Statistical Package of Social Sciences Version 19.0 (SPSS Inc., Chicago, IL, USA) and expressed as means ± SD, frequencies and percentages. Student t-test was used for statistical analysis of the means while the x2 test was used for statistical analysis of the percentages. P<0.05 was considered to indicate a statistically significant difference.
Results
Postoperative follow up showed paternity was achieved in 18 patients (31.6%) having clinical varicocele with normal sized testes and 3 patients (12%) with subnormal testes. A significant improvement in paternity was noted in patients with normal testicular volume (>15 cm3) (p=0.04) (Figure 3).

Relationship between testicular volume and positive post-operative paternity rate. Group 1 patients have normal testicular volume (>15 cm3). Group 2 patients have subnormal testicular volume (<15 cm3)
Varicocele was diagnosed clinically by palpation (clinical varicocele) and confirmed by sonography in 39 patients, whereas sonography alone (without clinical palpation) detected varicocele in 18 patients (subclinical varicocele). The positive paternity rate was higher (38.5%) in patients with clinical varicocele, compared with only 16.7% of patients with subclinical varicocele (p=0.001) (Figure 4).

Relationship between clinical and subclinical varicocele and postoperative paternity rate in group 1 patients.
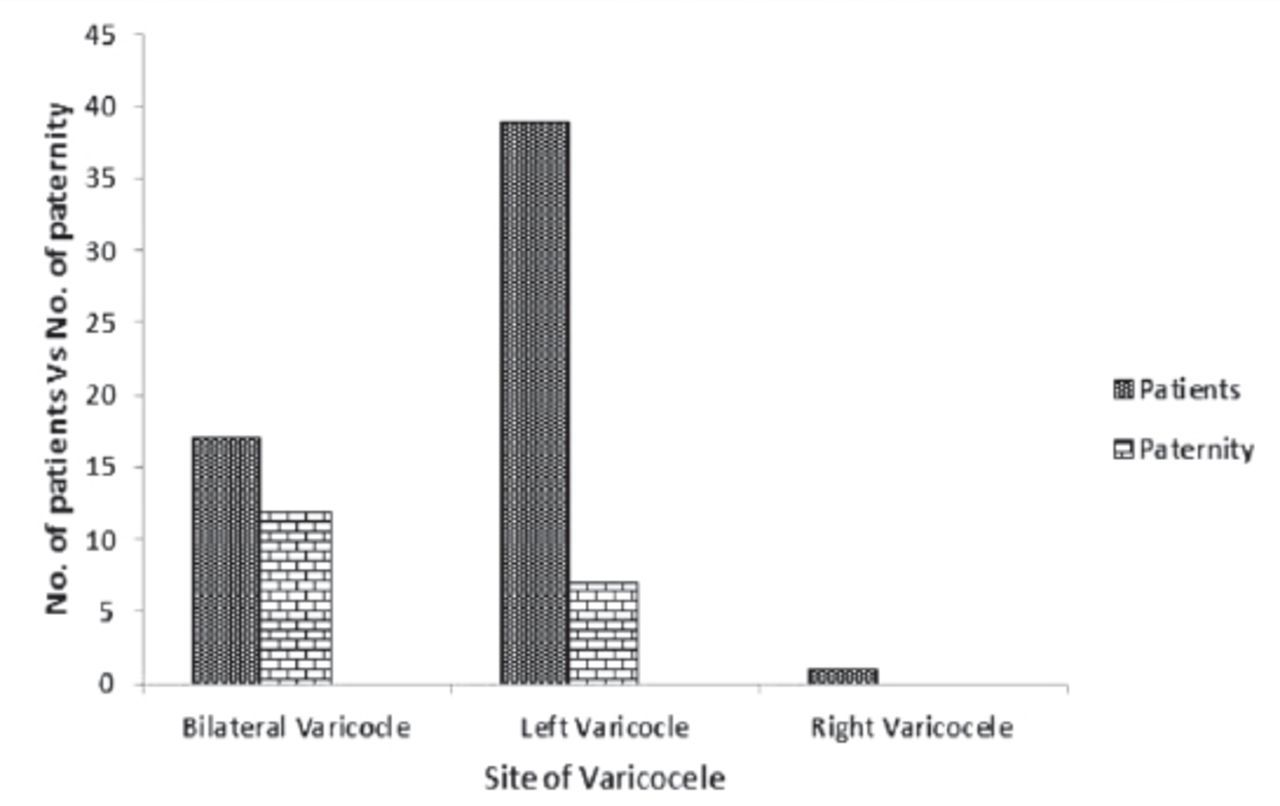
Varicocele was reported bilateral in 17 patients (29.8%), left sided in 39 patients (68.4%), and right sided in one patient (1.75%). The postoperative follow up of patient revealed paternity rate was significantly higher (70.6%) in patients with bilateral varicocele (p=0.04), compared with 17.9% patients with left sided varicocele and none in the right side varicocele (Figure 5). Patients with severe/large varicocele were 40 and 17 with mild to moderate varicocele, but there was no statistical significance in the postoperative paternity rate between mild, moderate, and large varicocele patients (p=0.694), (Figure 6).

Relationship between site of varicocele and post-operative positive paternity rate in group 1 patients.

Relationship between site of varicocele and post-operative positive paternity rate in group 1 patients.
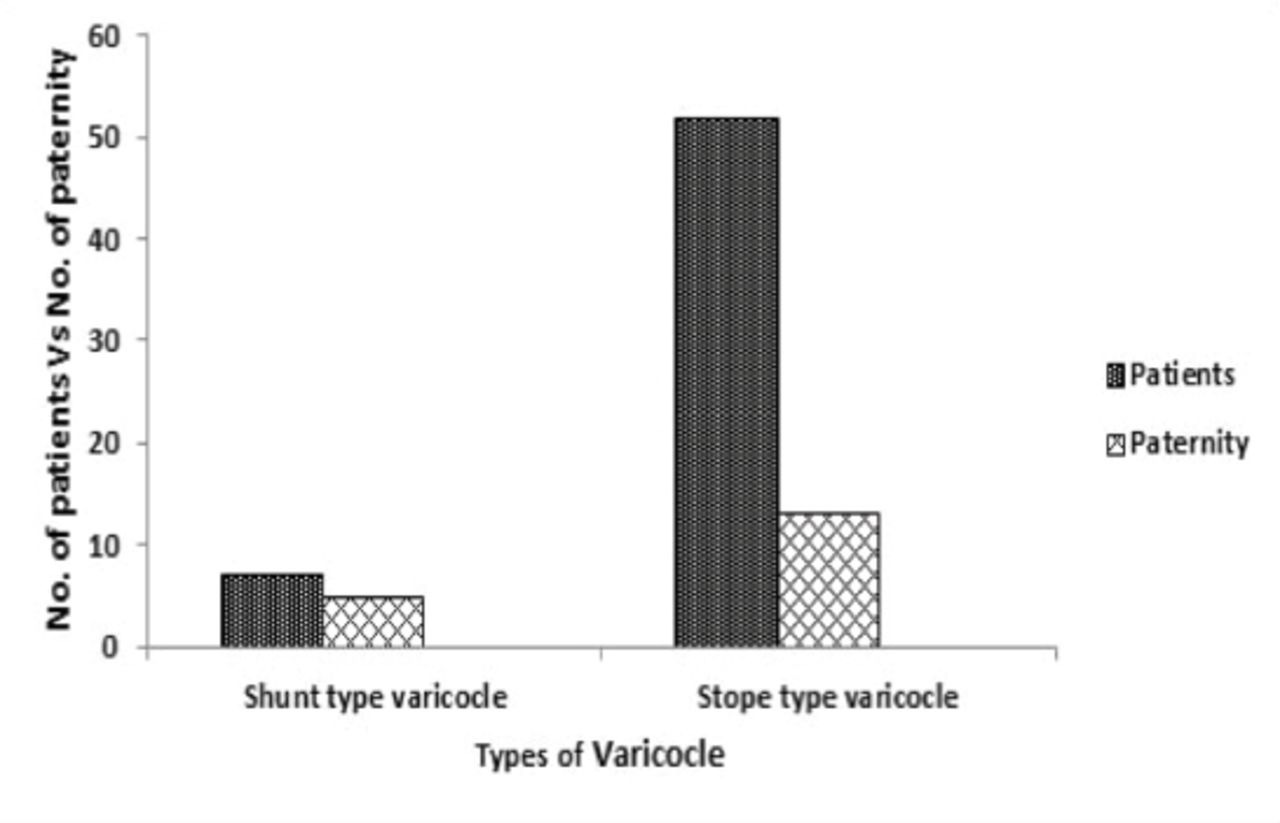
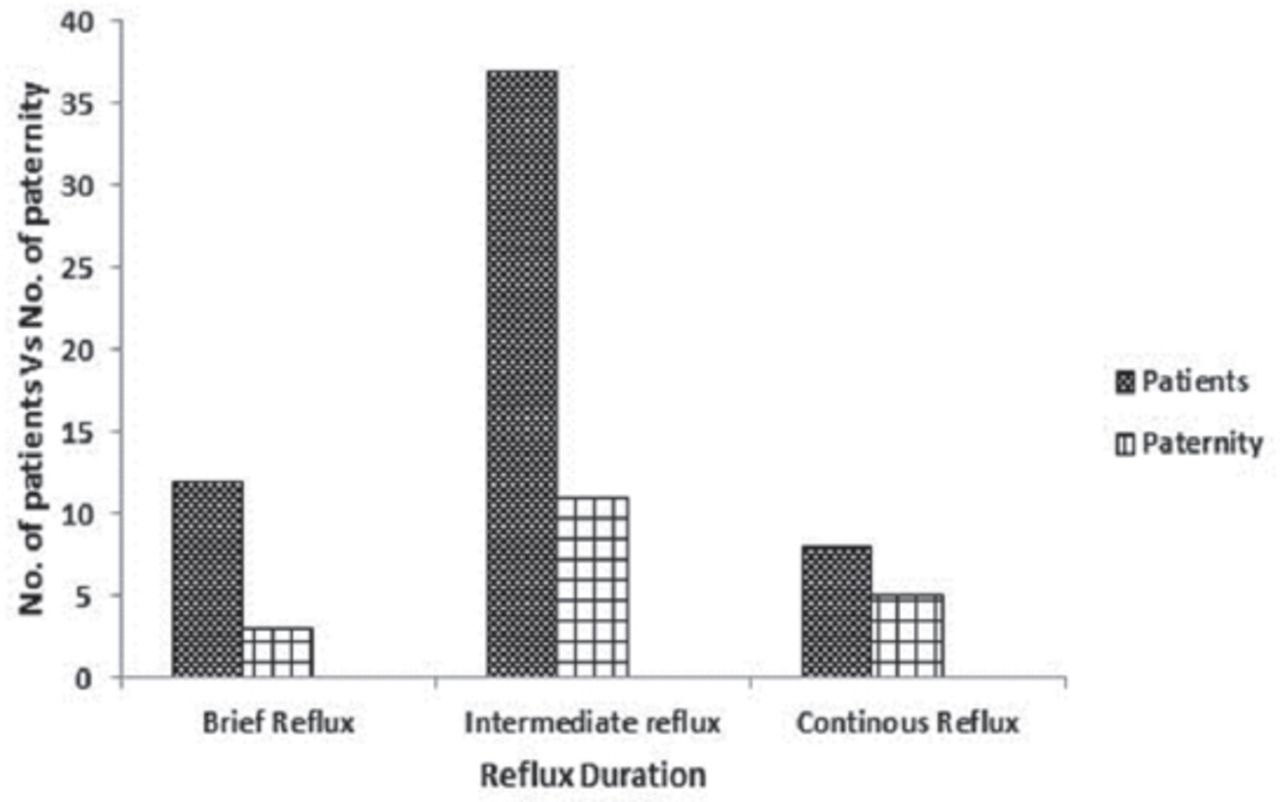
The relationship between type of varicocele (shunt or stop) and postoperative paternity rates are shown in Figure 7, where postoperative paternity was significantly higher in shunt-type varicocele (p=0.012). Regarding duration of reflux, there were increased in number of patients with reflux lasting up to 2 seconds, but less number of patients with reflux lasting for >2 seconds. However, patients with a continuous degree of venous reflux had a significantly higher paternity rate compared with intermediate/brief reflux (p=0.045) (Figure 8).

Relationship between site of varicocele and post-operative positive paternity rate in group 1 patients.

Relationship between site of varicocele and post-operative positive paternity rate in group 1 patients.
Discussion
Varicocele is the most common treatable cause of infertility in men.23 Many studies revealed that approximately two-thirds of varicocele patients showed improvement in various semen parameters and subsequent fertility rates not only in patients with clinically evident varicocele, but also in sub-clinical varicocele cases.24-27 However, some studies claimed that there is no significant improvement in sperm count, motility, and morphology after ligation of dilated testicular veins.28,29 In this study, we detected the sonographic and doppler ultrasound parameters, which can predict patients with varicocele and get benefit from the varicocele ligation. Duplex doppler ultrasound is a reliable and noninvasive method that is useful not only for diagnosis, but also for post-varicocele repair follow-up.30-32 This study showed that there was a statistically significant improvement in the paternity rate after repair of varicocele in patients with normal-sized testes (31.6%) compared with the varicocele patients with small volume testes (12%). This observation may be explained by the proven irreversible damage of testicular tissues exerted by varicocele. In the current study, paternity rate achieved in patients with normal-sized testes was higher than that in a study carried out by Evers and Collins,33 with an overall pregnancy rate of 21.7%. The higher paternity rate in our study was due to the selected criteria of our patients. Our results are similar to the study carried out by Donkol & Salem34 using the same sonographic parameters. The current study showed that the postoperative paternity rate was higher after varicocele repair in patients with clinically palpable varicocele with normal sized testes (38.5%) than that of patients with subclinical non-palpable varicocele (16.7%). This observation is supported by another study by Kiuchi et al,35 who reported that varicocele detected by physical examination was associated with greater postoperative improvement in semen parameters than that detected sonographically, and repair of subclinical varicocele did not seem to improve semen parameters significantly. Regarding the parameter of bilateral versus unilateral varicocele, this study showed that there is a significant improvement in paternity after bilateral varicocelectomy (70.6%)than unilateral varicocelectomy (17.5%). This result is supported by Donkol & Salem34 who also reported that bilateral varicocelectomy resulted in significantly greater improvement in postoperative seminal parameters and paternity rates. Regarding the DUS parameter of caliber of dilated veins in varicocele; the present study showed that there was no statistical significance between postoperative paternity rates whether the veins were markedly dilated (>4 mm in caliber) or mild to moderately dilated (2-4 mm in caliber). This result is in agreement with the results of Mohamed et al36 that varicocele detected by physical examination is more predictive of a good clinical outcome compared with the degree of dilatation of the veins measured by sonography alone.
This study showed that paternity after varicocele repair was significantly higher for shunt-type (71.4%)than stop-type varicocele (25%) and also in those having permanent reflux. This can be explained by the fact that there is continuous refluxing of blood to the testes in shunt-type varicocele, whereas in stop-type varicocele, reflux occurs only during straining. This can be confirmed by the observation of Mohseni et al22 who reported that shunting appears to be a precondition for significant varicocele and therefore might have some prognostic importance for the subfertility associated with varicocele.
Study limitation
This is a retrospective small scale study. Other limitation of this study was we did not assess the DUS parameters in patients with subnormal volume of testes, due to less number of patients’ records. Further prospective studies on large scale in both groups of patients and with scoring system of DUS parameters can open the new doors for selection of varicocele patients before surgical ligation to get more positive paternity rates.
In conclusion, proper selection of candidates prior to varicocele repair is the key for increased paternity rate. The DUS of the scrotum is the preferred method of investigation, which helps to select patients with varicocele who can be benefited by varicocelectomy. The DUS parameters of normal testicular volume (>15 cm3), bilateral varicocele, shunt type varicocele (retrograde and orthograde flow), and continuous reflux (>2 second), irrespective of caliber dilatation proved to be the most important criteria for the successful varicocelectomy and high paternity rates in patients with clinically palpable varicocele. The paternity rates after varicocelectomy appears low in patients having subclinical varicocele (non-palpable varicocele, detected by DUS only), subnormal volume of testes (<15 cm3), unilateral varicocele, stop-type of varicocele (retrograde flow only), and brief/intermediate (non-continuous) reflux.
Clinical Practice Guidelines
Clinical Practice Guidelines must include a short abstract. There should be an Introduction section addressing the objective in producing the guideline, what the guideline is about and who will benefit from the guideline. It should describe the population, conditions, health care setting and clinical management/diagnostic test. Authors should adequately describe the methods used to collect and analyze evidence, recommendations and validation. If it is adapted, authors should include the source, how, and why it is adapted? The guidelines should include not more than 50 references, 2-4 illustrations/tables, and an algorithm.
Acknowledgment
The authors would like to thank Dr. Zafar Rasheed, College of Medicine, Qassim University, AlQassim, Kingdom of Saudi Arabia for the critical review of the manuscript.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received July 12, 2015.
- Accepted October 14, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.