


Abstract
Objectives: To evaluate Parker Flex-It stylet as an alternative to GlideRite Rigid stylet to aid tracheal intubation with the Glidescope.
Methods: This prospective randomized trial was conducted at King Abdulaziz University Hospital, College of Medicine, King Saud University, Riyadh, Saudi Arabia between May and December 2014. Sixty American Society of Anesthesiologists I-II patients were randomly assigned to one of 2 equal groups receiving intubation by Glidescope using either GlideRite Rigid stylet (Group GS) or Parker Flex-It stylet (Group PS). The total intubation time, ease of intubation, incidences of successful intubation at first attempt, number of intubation attempts, use of optimization maneuvers, and possible complications were recorded.
Results: No significant differences between both groups regarding the total intubation time (p=0.08) was observed. Intubation was significantly easier in group PS compared with group GS as measured by visual analogue scale (p=0.001) with no significant differences between the groups regarding the rate of successful tracheal intubation from first attempt (p=0.524). However, the number of attempts at intubation and usage of external laryngeal manipulation were similar in both groups (p>0.05). The incidence of sore throat, dysphagia, hoarseness, and trauma were significantly higher in group GS (p<0.05).
Conclusion: Parker Flex-It stylet is as effective as GlideRite Rigid stylet when used by experienced operators in patients with normal airways using Glidescope; however, it is easier and less traumatic.
The GlideScope Ranger (GVL; Verathon Medical Inc., Bothell, WA, USA) is a novel portable, reusable video laryngoscope that has provided superior laryngeal visualization to facilitate tracheal intubation especially in the management of difficult airways; it provides indirect visualization of the glottis with a pronounced angle of 60° in the blade.1 It has a separate monitor connected to the handle via a cable. The tip of the blade is equipped with a high-resolution digital video camera, an LED light, and an antifogging system.2,3 Unlike the Macintosh laryngoscope, an indirect laryngoscope such as the GlideScope device provides a view of the glottis without the need to align the oral pharyngeal and laryngeal axes facilitating an excellent glottic visualization.4 However, insertion and advancement of the endotracheal tube (ETT) may be more difficult to pass through the vocal cords than direct laryngoscopy,5,6 and trauma is possible.7,8 The GlideScope have shown to function better when used in conjunction with use of a stylet to guide insertion of endotracheal tube.9,10 The GlideRite Rigid stylet (GRS) is a reusable rigid steel stylet, specifically designed by the manufacturer to resemble the distal part of the Glidescope video laryngoscopy blade for clear view of the airway, enabling quick intubation, its curvature approaches 90° with a radius of curvature of approximately 6 cm.11 Various investigators have recommended different curvatures of the ETT/stylet to optimally direct it into the trachea, including matching the blade’s 60° angle,11 configuring the ETT with a 90° bend,6,12 or using a J-shaped ETT.13 Other potential strategies may include the use of a flexible stylet that allows active modification of the tip of the tracheal tube during use.14,15 The Parker Flex-It Directional Stylet (FIS, Parker Medical, Highlands Ranch, CO) is a 2-piece plastic stylet that can be used for oral intubation, and allows continuous adjustment of the tube curvature during an intubation to enable the tube to follow the curvature of the airway.14,16 We hypothesized that the use of Parker Flex-It stylet to guide ETT might offer some benefit over the GRS. Therefore, the purpose of this study was to determine the optimal stylet-tracheal tube strategy for use with the GlideScope® laryngoscope. We compared efficacy of the 2 intubating aids including GRS versus Parker Flex-It stylet for orotracheal intubation in terms of the total intubation time (primary outcome), ease of intubation, the number of intubation attempts, the number of optimization manoeuvres, and possible trauma (secondary outcomes) when used by experienced GlideScope operators.
Methods
After obtaining Institutional Review Board approval and written informed consent for each patient, we studied 60 patients of American Society of Anesthesia (ASA) physical status I & II, of both gender, aged 18-50 years, with body mass index (BMI) <35, and scheduled for elective non-cardiac surgery that required general anesthesia with orotracheal intubation. This randomized clinical trial was conducted at King Abdulaziz University Hospital, College of Medicine, King Saud University, Riyadh, Saudi Arabia between May and December 2014. The trial has been performed according to the World Medical Association Declaration of Helsinki Ethical Principles for medical research, and it was registered at the ClinicalTrials.gov (NCT02439606).
Exclusion criteria
Anticipated difficult airway, need for rapid sequence induction, ASA physical status III-V, increase risk of gastric aspiration such as gastro- oesophageal reflux, pregnancy, patients who had no teeth, loose teeth, or oral trauma, known pathology, or previous surgery to the mouth, pharynx, larynx, or cervical spine, and any reason why the GlideScope is not, or could not be used. Potentially difficult intubation was defined if the patient had Mallampati class >III, thyromental distance of <6.0 cm, mouth opening of <2.5 cm, or history of previous difficult tracheal intubation.17
All patients were submitted to the routine pre-operative evaluation including airway assessment according to the hospital’s standard. Patients were randomly allocated using a computer-generated random code enclosed within a sealed opaque envelope, which opened as the patient entered the operative theatre into 2 equal groups, to receive orotracheal intubation using 2 different interventions in each airway setting. Patients in the Group GS (GlideRite Rigid stylet group) had their tracheas intubated with the GlideScope® video-laryngoscope, and the standard styletted tracheal tube using manufacturer’s GRS (GVL-ST1; Verathon Medical Inc., Bothell, WA, USA), whereas in the Group PS (Parker-Flex-It directional stylet group), intubation was performed with the GlideScope® video-laryngoscope and the styletted tracheal tube using Parker-Flex-It directional stylet (Parker Medical, Colorado, USA) (Flexi-Stylet) (Figure 1).

Photograph of A) Gliderite® rigid stylet and B) Parker Flex-It stylet.
Before the induction of anesthesia, the patient was positioned on the table with the head placed in a neutral position, and standardized monitoring techniques were applied. After pre-oxygenation using 100% oxygen for 3 minutes via a facemask, all patients received a standardized anesthetic technique that included induction with propofol 2-3 mg/kg IV (Propofol 1% Fresenius, Fresenius Kabi, GmbH, Graz, Austria), fentanyl 2 ug/kg IV (Janssen-Cilag, Beerse, Belgium), and cisatracurium 0.15 mg/kg IV (GlaxoSmithKline S.p.A. Parma, Italy) to facilitate tracheal intubation, then the patient’s lungs was ventilated by a face mask with sevoflurane (2.0-2.5%) in 100% oxygen for at least 90 second to allow full relaxation of the jaw and until no twitches by nerve stimulator monitor were present, at which point all patients received orotracheal intubation by GlideScope® videolaryngoscope of appropriate size according to the manufacturer’s label information. The ETTs (Rüschelit; Teleflex Medical, Research Triangle Park, NC, USA) used were styletted in accordance to the randomized allotment.
An ETT with each of the stylets was prepared by one of the study investigators, who had no further involvement with patient’s clinical care or outcome assessment. The GRS was used as according to the instructions supplied by the manufacturer. After successful endotracheal intubation, the target intracuff pressure of the endotracheal tube was set to less than 20 mm Hg, then the lungs were mechanically ventilated in the ventilation parameters that maintain an end-tidal carbon dioxide tension at 35-40 mm Hg. Anesthesia was maintained with 50% oxygen in air and 2-2.5% sevoflurane (Aesica Queenborough Ltd., for Abbott Laboratories Ltd., UK). Neuromuscular blockade was maintained by administering intermittent boluses of cisatracurium, if needed. One of the 2 attending anesthesiologists (operators) not involved in the collection or analysis of the data performed all intubations. All of them had experience in endotracheal intubation with GlideScope device, and are skilled in using of both stylets (at least successfully performed 15 GVL intubations using each stylet) before participation in the trial in order to eliminate a learning process bias. The ETT was then revealed, and the patient was intubated with the ETT and assigned stylet. External laryngeal manipulation (ELM) was permitted by co-investigator to improve the glottic view, or to facilitate intubation if requested by the operator. Every time the operator removed the blade of the GVL or ETT from the mouth, this was counted as an additional attempt at intubation. After the intubation was completed, the operator marked the ease of ETT insertion score using a visual analogue scale (VAS) (0= extremely easy to 100= extremely difficult) by the same tape measure throughout the study.18
The primary outcome was the total intubation time as measured by a blinded observer. The total intubation time was defined as the time from insertion of the blade of the GlideScope into the oral airway to the appearance of end-tidal carbon dioxide (ETCO2) curve of at least 30 mm Hg on the anesthesia monitor after insertion of the tracheal tube. The blind observer, who turned on the stop watch, was focusing on the anesthesia monitor so that he was blinded to the ETT or stylet. The total intubation time was not divulged to the operator until after the data collection sheet had been completed. Three failed attempts or passage of more than 120 seconds was considered a failed tracheal intubation, and the airway was managed using different intubation technique as deemed appropriate by the attending anesthesiologist, and those cases are excluded from the analysis.
Adequate depth of anesthesia was verified by clinical assessment and between attempts; incremental doses of propofol and intermittent mask ventilation with sevoflurane (2.0-2.5%) in 100% oxygen were permitted when needed to avoid arterial oxygen desaturation in these patients. The time required for intermittent mask ventilation was subtracted from the total time of intubation. Secondary outcomes for each group included: ease of intubation and the number of intubation attempts before successful intubation. Further, the number of optimization manoeuvres required, such as external laryngeal pressure, and whether the ETT was advanced off the stylet by an assistant were also recorded. Every time the tube was newly advanced to the glottic entrance, it was recorded as a new attempt. A common digital stop watch was used for all evaluations. To eliminate observer interpreter bias, data were collected by one investigator, and were available only to him throughout the study trial. This observer was trained on the use of GlideScope screen recording. Patients were examined by a trained blinded anesthetist for complications such as lip, mouth, and pharynx injury, or teeth damage. One hour after admission of the patients in the post anesthesia care unit and again 24 hours after surgery, they were interviewed by an independent investigator blinded to group allotment and all patients were asked to phonate and to report if they had any degree of hoarseness of voice, sore throat or dysphagia. Occurrence of adverse events during intubation such as severe hypoxemia (peripheral oxygen saturation [SpO2] <90%), laryngospasm, and bronchospasm were also reported.
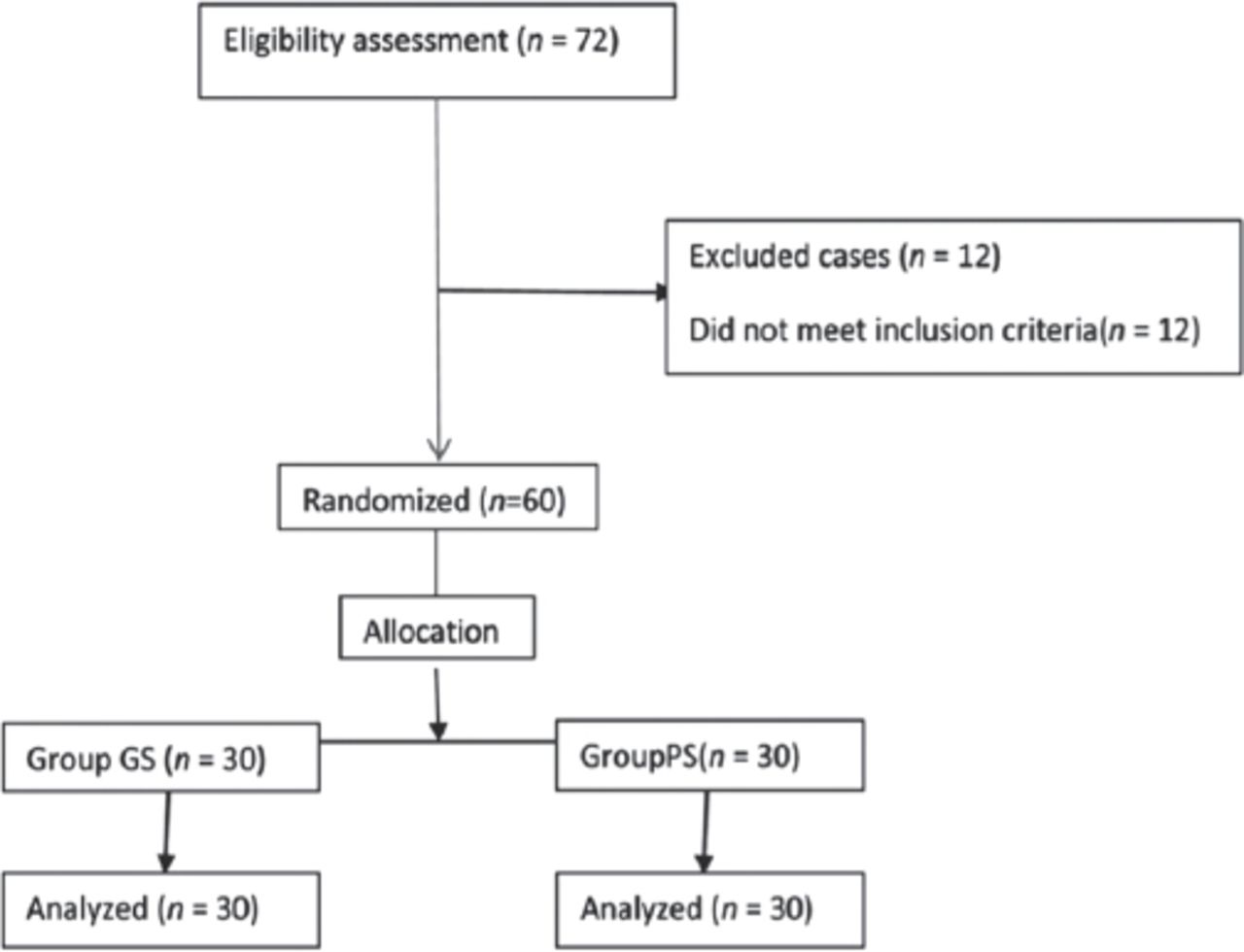
Figure 2 shows 72 patients on the surgical list screened for this study. Of these, 12 patients were not eligible due to exclusion criteria. The remaining 60 patients fulfilled all criteria, subsequently consented and were enrolled to participate in the study (n=30 per group), with no patient drop-outs.

Flowchart of the 72 patients on the surgical list screened.
Statistical analysis
A priori power analysis was performed on the basis of mean intubation time data obtained from a pilot study on 10 patients using GRS in 5 cases and Parker-Flex-It Directional stylet in 5 cases, all were not allocated in the study. The calculated sample size of 28 patients per group was estimated to have at least an 80% power (a=0.05, ß=0.2) to detect a difference of 30%, but a total sample size of 60 patients was selected in order to account for possible patient dropouts.
Statistical analysis was performed by the SPSS System (version 12.0, SPSS Inc., Chicago, IL, USA). Values were expressed as Means ±SD or as percentages. between-group comparisons for the numerical data were analyzed with Student’s t-test and the Mann-Whitney U test when indicated. Chi-square or Fisher’s exact test (when indicated) were used as appropriate for categorical data. The limit of statistical significance was set at p<0.05.
Results
Baseline demographics and size of endotracheal tube were similar between study groups as shown in Table 1. No significant differences between group GS and group PS regarding the total intubation time (34.6±3.6 versus 36.4±5.9; p=0.08, Table 2). Intubation was significantly easier in group PS compared with group GS as measured by visual analogue scale (VAS) reported by the operator (16.7±7.2 versus 29.1±8.9; p=0.001, Table 2). All intubations in both groups were performed within 120 seconds, with no significant differences between groups regarding the rate of successful intubation of the trachea from first attempt (p=0.524, Table 2). The number of attempts at intubation (p=0.331), usage of external laryngeal manipulation (p=0.452), and cases in which the ETT was advanced along the stylet by an assistant (p=0.365) were similar in both groups (Table 2).
Demographic data of 60 patients scheduled for elective non-cardiac surgery that required general anesthesia with orotracheal intubation.
Intubation data of 60 patients scheduled for elective non-cardiac surgery that required general anesthesia.
Additionally, no bronchospasm, or severe hypoxemia (SpO2 <90%) during intubation were observed in either group. The incidence of sore throat (p=0.023), dysphagia (p=0.039), hoarseness of voice (p=0.048), and trauma to the mouth and lips (p=0.049) were statistically significantly higher in the group GS compared to the group (Table 3).
Incidence of complications of 60 patients scheduled for elective non-cardiac surgery that required general anesthesia.
Discussion
In this prospective, randomized study, both GRS and Parker Flex-It stylet are equally efficient to aid tube placement during Glidescope video laryngoscopy in patients with normal airways as reflected by intubation time. However, Parker Flex-It intubating stylet benefits in performing relatively easier intubation (as indicated by VAS reported by the operator), and being less traumatic. The designed 60° upward angulation of the distal half of the GVL blade, coupled with the embedded camera, usually provides excellent glottic visualization, nonetheless, directing an endotracheal tube (ETT) through the vocal cords using the original stylet (GRS) could occasionally yield to 2 important concerns; making intubation difficult and moreover, it might impinge on laryngeal structures around the vocal cords with potential risk of trauma.7 Various modifications have been advocated to make intubation with the GlideScope easier principally using an altered stylet type or changing its angulation. The type of stylet used or the ideal configuration of a styletted-ETT for orotracheal intubation has been investigated.
The use of either standard malleable stylet or GRS in conjunction with the GlideScope videolaryngoscope was compared.15 The standard malleable stylet demonstrates similar performance characteristics to the GRS to perform orotracheal intubation in patients with normal airways and both stylets are suitable for orotracheal intubation even by beginner operators. In a different approach, a previous randomized clinical trial involving experienced operators to investigate the efficacy of the dedicated GlideScope-specific rigid stylet with the curvature adjusted to approximately 90° to the standard 90° angled malleable stylet in indirect laryngoscopy using the GlideScope was performed.19 Similarly, results showed that the dedicated GlideScope-specific rigid stylet and the standard malleable ETT stylet are equally effective in facilitating endotracheal intubation.
Alternatively, the most optimal configuration of a styletted-ETT for orotracheal intubation was studied in a previous research by Jones et al,12 a randomized controlled trial using experienced GVL operators on a heterogeneous group of patients to determine which of 2 ETT angles (60° versus 90°) and bends (forward versus reverse) was better, showed that a malleable stylet with a 90° bend resulted in faster intubation and it resulted in easier intubation than matching the GVL blade’s 60° angle, with no benefit from reverse loading. On the other hand, Dupanović et al20 confirmed that the 90° malleable stylet with reverse loading of the ETT is superior to 60° malleable stylet for ETT delivery to the glottic opening, and had a higher success. In the current study, the technique of GlideScope laryngoscopy was modified by the aid of the Flex-It stylet instead of its original stylet GRS. Flex-It™ stylet was designed originally for the use of Macintosh laryngoscope. The idea was that the Flex-It™ stylet has the capability of actively angulate the distal tracheal tube, which can facilitate insertion and advancement of the ETT. Therefore, it should be efficient in the same way during GlideScope laryngoscopy. Our results showed that flexible stylet with GlideScope laryngoscopy was as efficient as GRS yet it was perceived as easier intubation. Conversely, Turkstra et al14 reported that the Flex-It stylet is less effective for orotracheal intubation, when compared to 90° curved malleable stylet. The author attributed the previous results to the fact that most of their operators had greater prior experience with the malleable stylet and had practiced with the flexible stylet on mannequins. Analyzing the results of ease of intubation should be taken cautiously. Visual analogue scale came in favor of Parker Flex-It intubating stylet. The capability of the operator to continually manipulate the angle of the ETT during intubation with Flex-It stylet may be responsible for the previous result.16 However, if ease of intubation is perceived from other perspectives; the number of attempts, frequency of usage of external laryngeal manipulation, and advancement of ETT along the stylet by an assistant, both groups were similar in these respects.
Operators in our study were aware that the total intubation time was recorded, and this could have led to better clinical performance; however, any improvement in performance would likely have been distributed equally between the groups minimizing the impact of this effect. The endpoint of intubation time was set to observation of end-tidal CO2 on the anesthesia monitor, to provide an objective blinded endpoint.
Rare cases of palatal injuries have been described with both the GRS7 and the malleable stylet.8,21 Tonsillar and pharyngeal injuries were related to use of a rigid stylet, and the passage of the styled tracheal tube from the mouth opening to the vocal cords within the ‘potential blind spot’ of the GlideScope when attention is focused mainly on the GlideScope” screen.21,22 Leong et al23 also reported perforation of palate-pharyngeal wall during tracheal intubation using a GlideScope causing a sore throat and minor bleeding, which might be attributed to the use of a rigid stylet, big size blade, and excessive force during advancing the ETT through the glottis. Magboul et al24 reported the first case of serious lingual nerve injury in morbidly obese 80-year-old female, caused by the GRS. They recommended the use of soft stylets and soft tipped ETT to prevent trauma. Rigid stylets have been modified to reduce damage by different authors who studied different angles and types of stylet. However, irrespective of the stylet chosen to facilitate GVL, ETTs must be inserted carefully with minimal force. In the present study, the incidence of trauma after tracheal intubation with the Parker Flex-It stylet was significantly less compared to the use of GRS, which can be explained by the lower incidence of the ETT touching the vocal cords or other laryngeal structures,7 particularly when the stylet can be malleable and flexible; the essential distinguishing feature of Flex-It™ stylet.
Study limitations
Firstly, blinding of the anesthesiologist who performed tracheal intubation to the stylet being used was not possible. Secondly, all tracheal intubations were performed by experienced anesthesiologists; therefore, our results may vary if a less experienced anesthesiologists use the same technique. Finally, this study only investigated patients with normal airways. Therefore, further research should be undertaken in patients with difficult airways
In conclusion, during orotracheal intubation with GlideScope video laryngoscopy, Parker Flex-It intubating stylet is as effective as GRS when used by experienced operators in patients with normal airways; however, it is easier and less traumatic.
Saudi Medical Journal Online features
* Instructions to Authors
* Uniform Requirements
* STARD
* Free access to the Journal’s Current issue
* Future Contents
* Advertising and Subscription Information
All Subscribers have access to full text articles in HTML and PDF format. Abstracts and Editorials are available to all Online Guests free of charge.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 18, 2015.
- Accepted September 29, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}