


Abstract
Objectives: To compare laparoscopic extraperitoneal colostomy with transperitoneal colostomy for construction of a permanent stoma by measuring the incidence of parastomal hernia, and other postoperative complications related to colostomy.
Methods: The meta-analysis was carried out in the General Surgery Department of the Second Affiliated Hospital of Soochow University, Suzhou, Jiangsu Province, China in 2014. A literature search of Medline, EMBASE, Cochrane database, and the Chinese Biomedical Literature Database (CBM) from the years 1990 to 2014 was performed. The literature searches were carried out using medical subject headings and free-text words: extraperitoneal colostomy, transperitoneal colostomy, laparoscopic extraperitoneal colostomy, rectal cancer, laparoscopic abdominoperineal resection, parastomal hernia, permanent stoma, and colostomy-related complications. Two different reviewers carried out the search and evaluated studies independently.
Results: One randomized controlled trial and 6 retrospective studies were included. A total of 378 patients (209 extraperitoneal colostomy and 169 transperitoneal colostomy) were identified. Our analysis showed that there was a significantly lower rate of parastomal hernia (odds ratio 0.10; 95% confidence interval 0.03-0.29, p<0.0001) in the extraperitoneal colostomy group. However, the other stoma-related complications were not significantly different between the 2 groups.
Conclusion: Colostomy construction via the extraperitoneal route using a laparoscopic approach can largely reduce the incidence of parastomal hernia. Laparoscopic permanent sigmoid stoma creation through the extraperitoneal route should be the first choice after laparoscopic abdominoperineal resection.
Although the sphincter-preserving operation is widely used for the treatment of low rectal cancer, approximately 10-20% of patients still need a permanent colostomy after abdominoperineal resection (APR).1 The stoma relates to the quality of life of patients after APR. The existence of stoma changes the bowel evacuation habits of the patients and puts them under enormous psychological pressure; stoma-related complications make it harder for them. Of all the complications, parastomal hernia is one of the most common troublesome complication in patients with a permanent stoma. The incidence ranges from 4-48.1%.2 In open surgery, several techniques have reported to prevent parastomal hernia.3 The extraperitoneal route for stoma construction, which first reported by Goligher 4 in 1958, has been widely used. Many studies have proved that the extraperitoneal approach for sigmoid colostomy in open surgery presents a lower risk of herniation in comparison with the transperitoneal route. Lian et al5 recently revealed a significantly lower rate of parastomal hernia in the extraperitoneal colostomy group in his meta-analysis. Lian’s meta-analysis, which compared extraperitoneal colostomy with transperitoneal colostomy, provides guidance for surgeons to choose the route for stoma construction.
With the further development of laparoscopic rectal surgery, a permanent stoma can be constructed using the laparoscopic technique following APR.6 Hamada et al7 developed a laparoscopic technique to create an end-sigmoid colostomy through the extraperitoneal route and achieved good short-term outcomes. He also compared laparoscopic extraperitoneal colostomy with the transperitoneal colostomy, using the application of CT to follow up, and found that laparoscopic extraperitoneal stoma can reduce the incidence of postoperative parastomal hernia.7,8 Akamoto9 used a special retractor to make extraperitoneal laparoscopic sigmoid colostomy easier and more feasible.9
However, an extraperitoneal colostomy is technically much more difficult in laparoscopic APR than open APR, because the laparoscopic dissection via the extraperitoneal route is a technically demanding procedure.8 Because of its difficulty, laparoscopic extraperitoneal colostomy construction is rarely practiced. Although the transperitoneal route for laparoscopic construction of a sigmoid colostomy increases the chance of a parastomal hernia, it still used after laparoscopic APR. The choice of the extraperitoneal or transperitoneal route for permanent stoma is still confusing for many surgeons. Therefore, the aim of this study is to compare these 2 different route in terms of the operation time, and the incidence of stoma-related complications after laparoscopic APR. This study was designed to address whether an extraperitoneal route for colostomy in laparoscopic APR surgery can reduce the risk of stoma-related complications.
Methods
Search strategy
The meta-analysis was carried out in the General Surgery Department of the Second Affiliated Hospital of Soochow University, Suzhou, Jiangsu Province, China. A literature search of Medline, EMBASE, Cochrane database, and the Chinese Biomedical Literature Database (CBM) for the years 1990 to 2014 was performed. The literature searches were carried out using medical subject headings and free-text words: “extraperitoneal colostomy”, “transperitoneal colostomy”, “laparoscopic extraperitoneal colostomy”, “rectal cancer”, “LAPR” “laparoscopic abdominoperineal resection”, “parastomal hernia”, “PSH”, “permanent stoma”, and “colostomy-related complications”. Two different reviewers carried out the search and evaluated studies independently.
Inclusion criterion
All randomized, and non-randomized controlled clinical trials, which compared extraperitoneal with the transperitoneal route for patients undergoing permanent colostomy using a laparoscopic approach, and which reported the incidence of parastomal hernia or other postoperative complications related to the colostomy were included.
Exclusion criterion
Studies were excluded from the analysis if 1) the out-comes were not clearly reported for the 2 different routes, 2) it was impossible to extract the appropriate data from the published results such as abstracts, comments. Case reports, and conference proceedings were not included in the review. We also excluded studies with small-sized groups (<10 patients), or with no long term follow-up.
Date collection
The search was carried out by 2 investigators independently. All disagreements were resolved through discussion. Publications were included if they compared laparoscopic permanent sigmoid stoma creation through the extraperitoneal route to the transperitoneal route. Non-comparative studies, cases series, and case reports were excluded.
Statistical analysis
We used Review Manager 5.2 (RevMan, The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark) to conduct the review. The Mantel-Haenszel method was used for the statistical analysis of the operation time, parastomal hernia, and other postoperative complications related to the colostomy. Dichotomous data was analyzed for odds ratio (OR) and 95% effectiveness confidence interval (CI). The results were displayed by forest plot graph. P≤0.05 was considered statistically significant.
Results
To reduce the chance of small sample events, studies with small-sized groups (<10 patients) were excluded. Many stoma-related complications can still appear several years after the operation; therefore, studies with no long time follow-up were also excluded. Finally, one randomized controlled trial and 6 retrospective studies are included. A total of 386 patients 209 (55.3%) extraperitoneal colostomy, and 169 (44.7%) transperitoneal colostomy) were identified. These studies are detailed in Table 1.
Summary of published information from retrospective controlled studies on patients with EPC and patients with TPC.
Parastomal hernia
All 7 studies reported a lower rate of parastomal hernia in the extraperitoneal route, including the RCT. In our statistical analysis, among the 378 patients, the extraperitoneal route using a laparoscopic approach had a lower incidence of parastomal hernia when compared with the traditional transperitoneal route. There was a significantly lower rate of parastomal hernia (OR 0.10; 95% CI: 0.03-0.29, p<0.0001) in the extraperitoneal colostomy group (Figure 1).
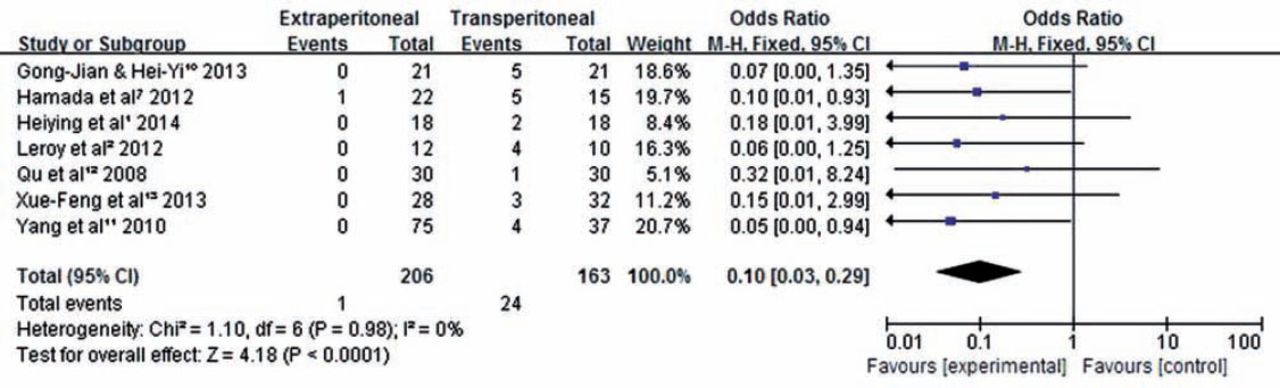
Analysis of controlled studies of EPC versus TPC in patients with rectal cancer. Outcome: parastomal hernia, 95% CI - 95% confidence interval, M-H - Mantel-Haenszel, df - degrees of freedom, OR - odds ratio, EPC - extraperitoneal colostomy after laparoscopic abdominoperineal resection surgery, TPC - transperitoneal colostomy after laparoscopic abdominoperineal resection surgery
Other stoma-related complications
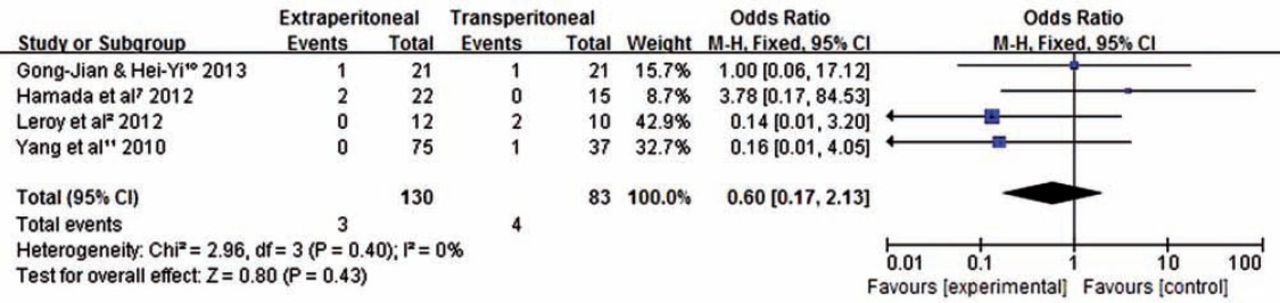
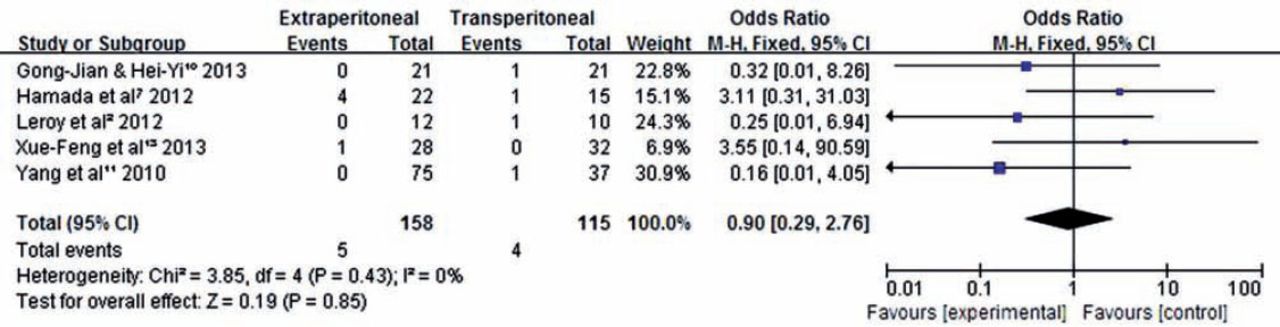
Four studies reported on necrosis of the stoma, but the difference did not reach statistical significance (OR 0.6; 95% CI: 0.17-2.13, p=0.43) (Figure 2). Another 5 studies reported on infection of the stoma, but again this did not reach statistical significance (OR 0.90, 95% CI: 0.29-2.76, p=0.85) (Figure 3).

Analysis of controlled studies of EPC versus TPC in patients with rectal cancer. Outcome: necrosis of the stoma, 95% CI - 95% confidence interval, M-H - Mantel-Haenszel, df - degrees of freedom, OR - odds ratio, EPC - extraperitoneal colostomy after laparoscopic abdominoperineal resection surgery, TPC - transperitoneal colostomy after laparoscopic abdominoperineal resection surgery

Analysis of controlled studies of EPC versus TPC in patients with rectal cancer. Outcome: infection of the stoma, 95% CI - 95% confidence interval, M-H - Mantel-Haenszel, df - degrees of freedom, OR - odds ratio, EPC - extraperitoneal colostomy after laparoscopic abdominoperineal resection surgery, TPC - transperitoneal colostomy after laparoscopic abdominoperineal resection surgery
The operation time
Four studies reported on the operation time, 2 studies focused on the entire operation time, and 2 studies focused on the time for the colostomy construction. Our analysis shows that there is no statistically significant difference regarding the length of the entire operation time (total 34 patients; heterogeneity: Chi2=4.84, p=0.36) (Figure 4). However, the time for colostomy construction via the extraperitoneal route using a laparoscopic approach is longer than the transperitoneal route (total 39 patients; heterogeneity: Chi2=0.85, p<0.00001) (Figure 5).

Analysis of controlled studies of EPC versus TPC in patients with rectal cancer. Outcome: operation time, 95% CI - 95% confidence interval, M-H - Mantel-Haenszel, df - degrees of freedom, OR - odds ratio, EPC - extraperitoneal colostomy after laparoscopic abdominoperineal resection surgery, TPC - transperitoneal colostomy after laparoscopic abdominoperineal resection surgery

Analysis of controlled studies of EPC versus TPC in patients with rectal cancer. Outcome: operation time of colostomy construction, 95% CI - 95% confidence interval, M-H - Mantel-Haenszel, df - degrees of freedom, OR - odds ratio, EPC - extraperitoneal colostomy after laparoscopic abdominoperineal resection surgery, TPC - transperitoneal colostomy after laparoscopic abdominoperineal resection surgery
Discussion
Compared with open surgery, laparoscopic permanent sigmoid stoma creation through the extraperitoneal route has the potential to minimize damage to the abdominal wall, so this route is also worth considering for laparoscopic surgery.7 With the further development of laparoscopic rectal surgery; permanent stoma creation will be widely used in many cases. This meta-analysis is an assessment of laparoscopic extraperitoneal colostomy with regard to the incidence of parastomal hernia and other colostomy-related complications.
Our results showed no statistical differences in the whole operation time, the rate of necrosis, or the occurrence of infection of the stoma. However, the incidence of parastomal hernia was higher using the laparoscopic transperitoneal colostomy compared with the extraperitoneal route (OR 0.10; 95% CI: 0.03-0.29, p<0.0001). The main reason for the occurrence of the parastomal hernia is that the junction between the colon and the abdominal wall is not dense enough.10 The lateral peritoneum was sutured with the intestinal wall in the transperitoneal route, which will cause a gap between the abdominal cavity and the stoma. What makes it different is that the colon was pulled out through the tunnel of the lateral peritoneum using a laparoscopic approach via the extraperitoneal route, which makes the gap between the abdominal cavity and the stoma disappear compared with open surgery. This may explain the lower incidence of the parastomal hernia after extraperitoneal colostomy. Our analysis showed laparoscopic permanent sigmoid stoma creation through the extraperitoneal route can reduce the incidence of the parastomal hernia.
The time of colostomy construction via the extraperitoneal route using a laparoscopic approach is longer than the transperitoneal route. Compared with the transperitoneal route, extraperitoneal route using a laparoscopic approach required additional procedures. The sigmoid colon is stretched through the extraperitoneal tunnel, and the seromuscular layer of the sigmoid colon is sutured with the side of the peritoneum under laparoscopic. These steps are difficult and time consuming for many young surgeons, and is why the time for colostomy construction via the extraperitoneal route using a laparoscopic approach takes longer than the transperitoneal route.
Regarding other post-operation complications, Hamada et al7 reported an 18.2% infection rate in the extraperitoneal route compared with 6.6% in the transperitoneal route, and necrosis of the stoma was 9.1% higher than the transperitoneal route. However, there was no significant difference between the groups.7 In our meta-analysis, the chance of infection of the stoma was also not significantly reduced after the extraperitoneal route using a laparoscopic approach, the same as the chance of the necrosis of the stoma.
The main limitation of our study is the small number of RCTs, and we therefore included some retrospective studies in the statistical analysis. A prospective RCT is warranted to further determine the role of the extraperitoneal route in the prevention of stoma-related complications.
In conclusion, colostomy construction via an extraperitoneal route using a laparoscopic approach may take a little more time compared with the transperitoneal colostomy, but this route can largely reduce the incidence of parastomal hernia without increasing the chances of necrosis or infection of the stoma. With the development of laparoscopic techniques, laparoscopic permanent sigmoid stoma creation through the extraperitoneal route will become the first choice for many surgeons.
- Received September 25, 2014.
- Accepted December 15, 2014.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.