


Clinical Presentation
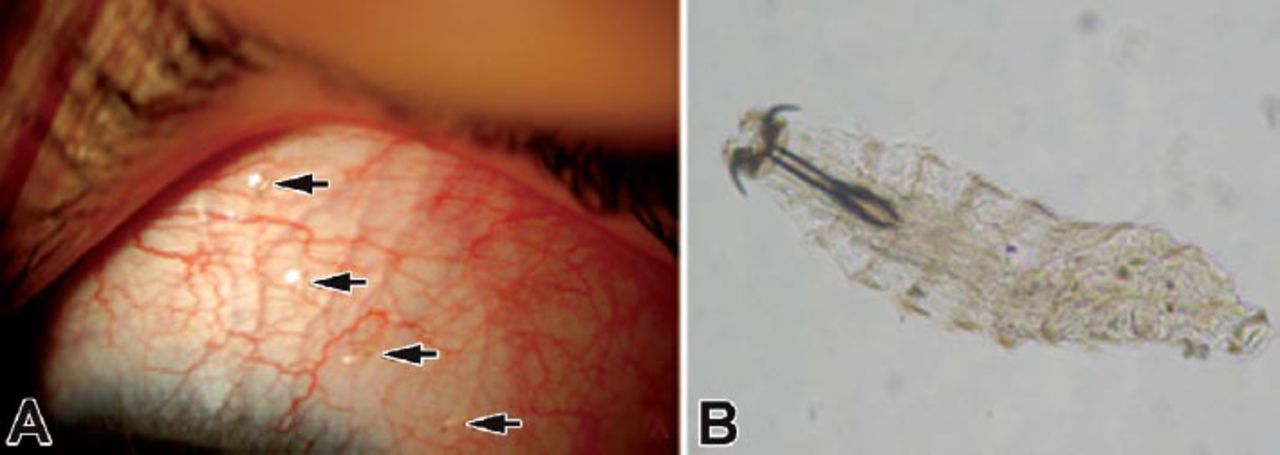
A 35-year-old woman was referred to our Ophthalmology Department with severe tearing, red eye, foreign body sensation, and itching on her left eye after a hit by a fly several hours ago. Her visual acuities were 20/20 in both eyes. Slit lamp examination revealed a dozen larvae moving on the bulbar conjunctiva and in the fornices associated with mild redness, chemosis, and lid edema (Figure 1A).

Photograph showing: A) Oestrus ovis larvae over the conjunctiva (arrows); and B) microphotograph of the first stage larva of Oestrus ovis.
Questions
What is the diagnosis?
What is the management?
What is the etiology of this infestation?
Answers
Due to the history and typical clinical appearance, a diagnosis of ophthalmomyiasis externa was considered.
After the instillation of 0.5 % proparacaine HCl as an anesthetic eye drop (Alcaine, Alcon Laboratories, Fort Worth, TX, USA), the larvae was removed by plain forceps, but the larvae actively avoided the bright light of the slit lamp, and escaped deep into conjunctival fornices. However, 15 minutes after instilling 2 drops of cyclopentolate 1% (Sikloplejin 1%, Abdi Ibahim, Istanbul, Turkey) the larvae were moving more slowly, nearly inactive, and could not actively escape from the bright light. It was easier to remove by plain forceps because they could not attach to the conjunctiva as strong as before. Topical antibiotic and steroid drops were prescribed for a week. Follow-up examination on subsequent day showed no residual larvae.
The specimen were sent to the Parasitology Department, mounted on a microscope slide, and photographed under a microscope. The larvae were transparent, segmented, and had black mouth parts in the anterior region, and they were identified as first stage Oestrus ovis (Figure 1B).
Discussion
Ophthalmomyiasis externa is the infestation of conjunctiva by the larvae of Oestrus ovis, which is a large, yellowish-gray fly approximately 10-12 mm long, and mostly located in the sheep’s nasal cavity.1 The fly can eject the larvae in a milky fluid while in flight, and it is not necessary to hit the eye directly for infestation of humans, especially in sheepherding areas.2 Three types of ophthalmomyiasis are: external type - where the infestation is on the external ocular surface; internal type - where the larvae penetrate into the globe; and the third type, which is most destructive, is the orbital myiasis, where the larvae penetrate deep into the orbital cavity and destruct the tissues.3 Our case is the external type, where the larvae were seen on the conjunctival surface with normal fundus and orbita. The most common clinical presentation of external ophthalmomyiasis is acute catarrhal conjunctivitis associated with marked redness, lacrimation, pain, and foreign body sensation.3 Routine treatment is the removal of larvae with fine forceps after instillation of topical anesthetic drops.1 Different treatment options include topical tobacco dilution, ether, potassium permanganate, chloroform, pig’s fat, basil, chewing gum, and ivermectin.4 Irrigation of conjunctival sac with saline solution is not so effective alone because the larvae bite the conjunctival firmly by their hooks. It is essential to remove the larvae immediately, prevent residual larvae, and its potential complication of internal and orbital ophthalmomyiasis. As the larvae escapes from the bright light of slit lamp, the clinician should try to find the larvae in the folds of the conjunctival sac. The larvae bite the conjunctiva with their hooks and there may be conjunctival damage during the mechanical removal of the larvae. A comparison between removal after proparacaine eye drop and combination of cyclopentolate with proparacaine eye drop revealed that the larvae were moving more slowly, nearly inactive, and could not actively escape from the bright light in the latter.
Cyclopentolate is a parasympatholytic anticholinergic agent, such as atropine and scopolamine, and it blocks the muscarinic receptors, and induces relaxation of the sphincter of the iris and the ciliary muscles.5 We suppose that the drug may cause muscle paralyses of the larva. To the best of our knowledge, the effect of cyclopentolate on Oestrus ovis larvae had not been reported before.
As a novel finding in this report, topical cyclopentolate 1% drop instillation with pressure to medial canthus for a minute might affect the larvae, and make the collection of larvae easier, and we recommend to investigate this association with further in vitro studies. Topical cyclopentolate 1% drop, as a part of routine ophthalmic examination, as a part of ruling out internal ophthalmomyiasis, makes the collection of larvae easier, and safer.
Footnotes
Notice: Authors are encouraged to submit quizzes for possible publication in the Journal. These may be in any specialty, and should approximately follow the format used here (maximum of 2 figures). Please address any submissions to: Editor, Saudi Medical Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. Tel. +966 (11) 4777714 Ext. 42846.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.