


Clinical Presentation
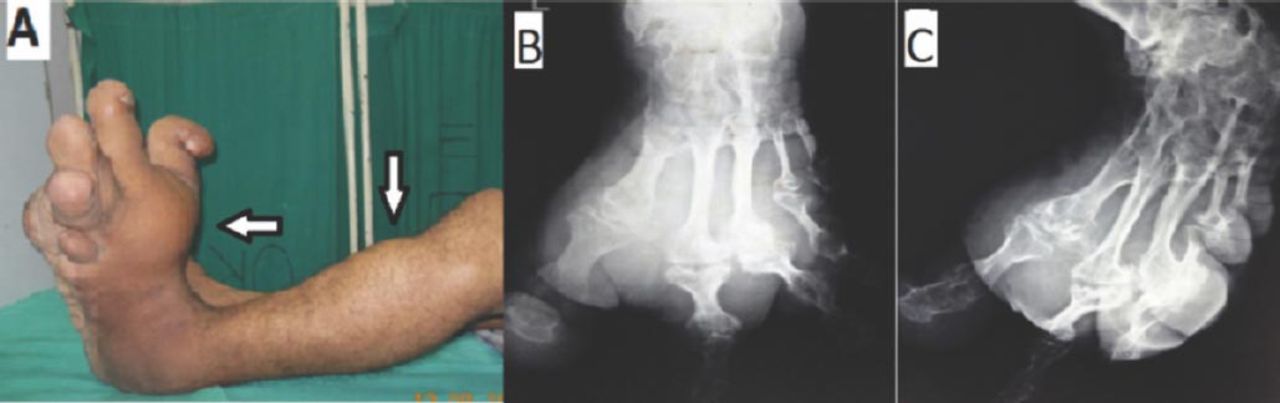
A 28-year-old male patient presented to us with the history of swelling over the left foot, the proximal left leg, and another separate swelling over the left greater trochanteric region since birth. The rate of enlargement of digits was disproportionate to age. For the last 2 years, he started complaining of decreased sensation over the dorsum of the left foot and sole. The physical examination confirmed the presence of megalodactyly in all digits except the little toe that was associated with the presence of soft, fibrolipomatous tissue over the dorsum of the left foot. The size of the swelling was 20 cm x 8 cm and was soft in consistency, non-fluctuant, non-pulsatile, and non-adherent to the underlying structures. There was no bruit or edema in the involved extremity. The affected limb was 8 cm longer than the opposite limb due to increased thickness of the sole (Figure 1A). The swelling over the greater trochanter and proximal leg were asymptomatic and of a similar nature to the swelling in foot. Anteroposterior and oblique radiographs of the foot were advised (Figures 1B & 1C).
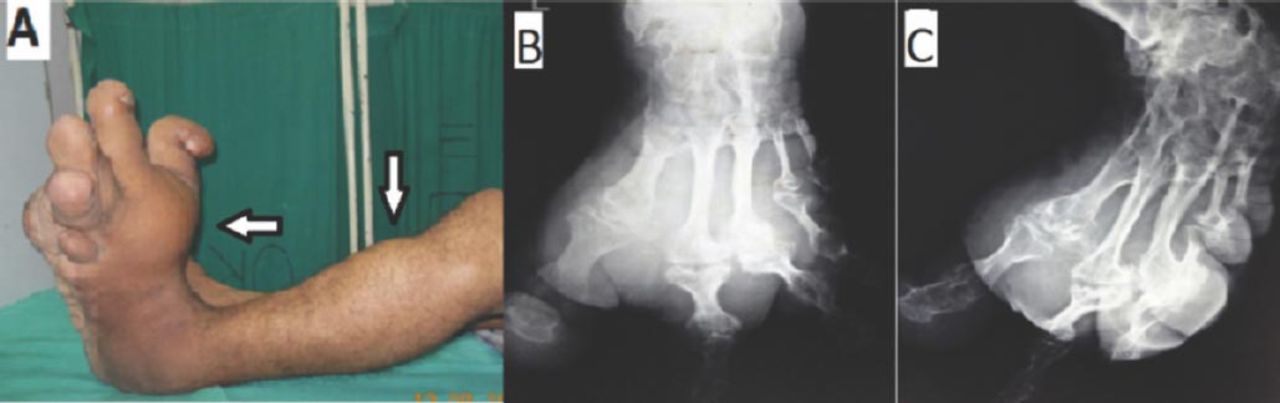
Clinical photograph shows disproportionate enlargement of digits and huge swelling over foot. Fatty hump also present over proximal leg A) Plain radiographs, anteroposterior and oblique views show hypertrophy of the bones B & C) Advanced degenerative changes are also seen in the involved joints.
Questions
What are the findings on plain x-ray?
What is the diagnosis?
What is the management in this case?
Answers
Anteroposterior and oblique radiograph of foot (Figures 1B & 1C) showed hypertrophy of bones (in the form of lengthening and broadening) and soft tissues along the medial aspect of foot (involving the 1st, 2nd, and 3rd digits and metatarsals) with advanced degenerative changes seen in the involved joints.
The diagnosis is macrodystrophia lipomatosa of the lower limb. This is a clinic-radiological diagnosis and confirmed by histopathological examination.
The patient was informed of the multiple debulking surgeries, but he was not ready for this. Hence, after proper informed consent from the patient and his father, below knee amputation was performed. He is now walking with a patellar-tendon-bearing (PTB) prosthesis and doing his all routine activities satisfactorily. He has been advised to follow-up every 6 months for the swelling over the greater trochanter and proximal leg.
Discussion
Macrodystrophia lipomatosa is a rare nonhereditary, congenital condition, which is characterized by local gigantism of hands and feet. Progressive proliferation of all mesenchymal elements, with a disproportionate increase in fibroadipose tissue results in macrodactyly and megalodactyly. It usually involves areas of distribution of the plantar and median nerves.1,2 The localized gigantism is almost invariably recognized at birth as in our case, but starts to cause problems as the child grows. There may be difficulty in walking and in performing routine activities, but cosmetics are the main issue concerning the patient requiring consultation with surgeons. This disease is usually unilateral. The growth velocity may differ from digit to digit, and the abnormal growth usually ceases at puberty. The lower limb is more frequently involved than the upper limb. The abnormal area is usually along a specific sclerotome. The second and third digit of the hand and feet are most frequently involved, corresponding to the median nerve and medial plantar nerve supply in the upper and lower limb.3 The etiology of the macrodystrophia lipomatosa remains unclear. As the child grows there may be degenerative changes of small joints and compression of neurovascular structure. Histopathologically, cut sections are rich in adipose tissue sprinkled in a fine lattice like fibrous tissue as in our case.4 Plain radiographs demonstrate abnormalities in both the soft tissues and bony elements. The affected phalanges and metatarsal bones show an increase in width and length, and are often splayed at their distal ends, giving a mushroom like appearance. The articular surface may slant and in late childhood, severe secondary degenerative changes may affect the joints.3 Ultrasound can assess the soft tissue and changes in the nerve. These are better visualized on MRI. A CT is better to evaluate the changes in bone. The differential diagnosis of macrodystrophia lipomatosa includes lymphangiomas, hemangioma, Klippel-Trenaunay-Weber syndrome, neurofibromatosis, proteus syndrome, and fibrolipomatosis.2 Surgical correction is the treatment of choice. The main surgical principle in treating this condition is to improve the cosmetic appearance, and to preserve the neurological function as far as possible.4 Surgery is usually carried out after puberty when growth ceases. Cautious and planned use of multiple debulking procedures, epiphysiodesis, and various osteotomies are recommended to achieve the best results. However, complications associated with overzealous debulking procedure lead to nerve injury with an incidence reported as high as 30-50%. A localized recurrence rate of 33-60% makes the management of macrodystrophia lipomatosa more demanding.
In conclusion, our case is unique as there was a separate swelling at the greater trochanter and proximal leg (not supplied by median and plantar nerves). A proper clinical examination, plain radiography, and ultrasound can diagnose macrodystrophia lipomatosa confidently, thus obviating the need for MRI, especially in a poor socio-economic set up. Amputation with prosthesis can be performed with satisfactory results if the gigantism is very huge and the patient is not ready for multiple debulking surgeries.
Acknowledgment
We gratefully acknowledge Dr. Rahul Ranjan, Junior Resident, Department of Orthopedic surgery, for valuable assistance in the management of this patient and preparing this manuscript.
Footnotes
Notice: Authors are encouraged to submit quizzes for possible publication in the Journal. These may be in any specialty, and should approximately follow the format used here (maximum of 2 figures). Please address any submissions to: Editor, Saudi Medical Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. Tel. +966 (11) 4777714 Ext. 42846.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.